Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
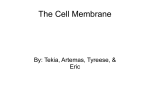
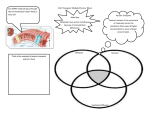
CLINICAL SCIENCES Characterization of Retrokeratoprosthetic Membranes in the Boston Type 1 Keratoprosthesis Rebecca C. Stacy, MD, PhD; Frederick A. Jakobiec, MD, DSc; Norman A. Michaud, MS; Claes H. Dohlman, MD, PhD; Kathryn A. Colby, MD, PhD Objective: To evaluate retroprosthetic membranes that can occur in 25% to 65% of patients with the Boston type 1 keratoprosthesis (KPro). Methods: Two patients with Peter anomaly and 2 with neurotrophic scarred corneas underwent revisions of their type 1 KPros because of visually compromising retroprosthetic membranes. The excised membranes were studied by light microscopy with hematoxylin-eosin, periodic acid– Schiff, and toluidine blue stains. Immunohistochemical and transmission electron microscopic examination were also used. Results: Light microscopic examination revealed that the retro-KPro fibrous membranes originated from the host’s corneal stroma. These mildly to moderately vascularized membranes grew through gaps in the Descemet membrane to reach behind the KPro back plate and adhere to the anterior iris surface, which had undergone partial lysis. In 2 cases, the fibrous membranes merged at the pupil with matrical portions of metaplastic lens epithelium, forming a bilayered structure that crossed the optical axis. Retro-KPro membranes stained positively for ␣–smooth muscle actin but negatively for pancytokeratin. Electron microscopy confirmed the presence of actin filaments within myofibroblasts and small surviving clusters of metaplastic lens epithelial cells. Conclusions: Stromal downgrowth, rather than epithelial downgrowth, was the major element of the retroKPro membranes in this series. Metaplastic lens epithelium also contributed to opacification of the visual axis. Florid membranous inflammation was not a prominent finding and thus probably not a requisite stimulus for membrane development. Further advances in prosthetic design and newer antifibroproliferative agents may reduce membrane formation. Arch Ophthalmol. 2011;129(3):310-316 T Author Affiliations: David G. Cogan Laboratory of Ophthalmic Pathology (Drs Stacy and Jakobiec), Howe Laboratory (Mr Michaud), and Cornea and Refractive Surgery (Drs Dohlman and Colby), Massachusetts Eye and Ear Infirmary and Harvard Medical School, Boston, Massachusetts. HE BOSTON TYPE 1 KERATOprosthesis (KPro) has been successfully used to restore vision in cases of chronic corneal disease and graft failure. This device, which consists of a clear polymethyl methacrylate optic and back plate (flange) with a titanium locking ring, is implanted in a corneal graft that is then transplanted into the patient’s eye.1 The back plate is made of polymethyl methacrylate, or more recently, titanium,2 and is perforated by holes to allow aqueous nourishment of the donor cornea. The back plate, which is inserted into the patient’s cornea, is slightly larger (by 0.5 mm) than the trephined punch in the patient’s eye. This design was intended to create a slightly overriding back plate for promoting a tight junction between the host’s and donor’s stroma at the wound site. The host corneal tissue may swell at this interface, however, (REPRINTED) ARCH OPHTHALMOL / VOL 129 (NO. 3), MAR 2011 310 protruding slightly posteriorly into the anterior chamber (Figure 1A). The clear optic provides excellent visual acuity, and the Boston KPro is generally well retained.3-6 The postoperative development of retroprosthetic membranes is unfortunately relatively common, occurring in 25% to 65% of patients within a year after KPro implantation. Up to 45% of these cases require eventual treatment.3-5,7 In most cases, the membrane can be cleared with YAG membranotomy, but approximately 11% require surgical revision with explantation of the KPro device and associated membranous and corneal tissue.3 The histopathologic features of such retro-KPro membranes have previously received limited attention.8 In this series of 4 cases, we report in greater detail the histopathological characteristics and origins of retro K-Pro membranes from 4 explanted grafts, with WWW.ARCHOPHTHALMOL.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/ophth/10235/ on 04/30/2017 A B ∗ Donor cornea ∗ Host cornea Descemet membrane Figure 1. The structure and anatomy of an in situ type 1 keratoprosthesis (KPro) and a retro-KPro membrane. A, The host cornea is slightly swollen at the edge of the KPro back plate (which attaches circumferentially to the optic as a flange), resulting in an overhang of corneal tissue that protrudes into the anterior chamber. The resulting gap in the Descemet membrane (*) permits migration of proliferating fibroblasts. B, A subtle retro-KPro membrane (arrow) obscures the visual axis behind the clear optical center of the KPro. The holes in this titanium KPro back plate to facilitate nourishment of the overlying stroma are visible through the donor cornea. supplemental immunohistochemical and transmission electron microscopic findings. METHODS Four explanted Boston type 1 KPros with attached retro-KPro membranes were received by the David G. Cogan Laboratory of Ophthalmic Pathology at the Massachusetts Eye and Ear Infirmary between September 2009 and April 2010. Each patient’s initial KPro surgery and the surgical revisions were performed at the same institution by 1 of 2 primary surgeons (C.H.D. and K.A.C.), 1 of whom did 3 of the surgeries. During the surgical revisions, the patient’s existing KPro was removed intact with its attached retroprosthetic membrane and surrounding donor corneal tissue. This complex was placed in formalin, and after a minimum of 48 hours, the donor cornea and retroprosthetic membranes were dissected off of the polymethyl methacrylate or titanium KPro back plate. Under a grossing microscope, the donor cornea was bisected or trisected radially, and each piece was then peeled off the front surface of the KPro. The back plate was then flipped over for continued dissection of the retro-KPro membrane, which was peeled away, while still attached to the corneal donor tissue at the edge. This resulted in 2 or 3 U-shaped pieces of tissue per KPro, with 1 leg of the U formed by the donor cornea and the other by the retro-KPro membrane. Care was maintained to preserve the connection between the donor cornea and fibrous membrane during dissection. The tissue was further sectioned, embedded in paraffin, and stained with hematoxylin-eosin. Immunohistochemical stains for ␣–smooth muscle actin (SMA) (prediluted mouse monoclonal IgG; Ventana Medical Systems, Tucson, Arizona) and pancytokeratin (mouse monoclonal IgG, 1:80 and 1:160; Becton Dickinson, San Jose, California, and Signet Laboratories, Dedham, Massachusetts) were used following standard staining protocols9,10 on Ventana Benchmark automated immunostainers (Ventana Medical Systems) at the Massachusetts General Hospital. In 2 cases, some of the tissue that had been peeled off of the back plate was submitted for transmission electron microscopy after fixation in Karnovsky fixative (glutaraldehyde, 2.5%, and formaldehyde, 2%, in 0.1M cacodylate buffer with 2.5mM calcium chloride). Tissue was processed through aqueous osmium tetroxide, 2%, and graded ethanol, transitioned with propylene oxide, and embedded in an epon substitute (t-Epon; Tousimis Research Corporation, Rockville, Mary- land). One-micron sections were stained with toluidine blue and 70-nm-thin sections were stained with saturated uranyl acetate and Sato lead stain. Sections were examined with transmission electron microscopy (Philips CM 10; Philips Scientifics, Eindhoven, the Netherlands). RESULTS CLINICAL CHARACTERISTICS Four patients with scarred and opacified corneas due to Peter anomaly (2 cases) or neurotrophic corneas (2 cases) received Boston type 1 KPros. Preoperative objective studies of trigeminal nerve dysfunction were not performed in the patients with Peter anomaly who had already had failed corneal transplants. In all patients, the diameter of the back plates was 8.5 mm, except for a 2-year-old who received a 7.0-mm back plate. Two patients had several failed penetrating keratoplasties before receiving the KPro, and 1 patient had a failed corneal patch graft. Further clinical characteristics of all 4 cases are summarized in the Table. Three patients developed clinically evident retroKPro membranes between 3 and 4 months after surgery (Figure 1B). Patient 1 displayed a retro-KPro membrane 3 months after her initial KPro placement. YAG capsulotomy (40 pulses at 2.8 mJ) failed to break through the retroprosthetic membrane; surgical excision was then performed. In patient 2, a retro-KPro membrane was observed 4 months after the initial KPro implant. YAG capsulotomy (18 pulses at 3 mJ) was attempted at 7 months postoperatively and was initially successful, but regrowth of the membrane within 6 weeks required surgical revision. Patient 3 was a 2-year-old child who developed a retro-KPro membrane 4 months after her initial surgery. At 5 months, she developed the additional complication of a partial KPro extrusion and proceeded to surgery without YAG treatment. Patient 4 had a KPro that was scheduled for surgical revision because of a descemetocele. A retro-KPro membrane had not been observed prior to surgery, but during the surgical repair and (REPRINTED) ARCH OPHTHALMOL / VOL 129 (NO. 3), MAR 2011 311 WWW.ARCHOPHTHALMOL.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/ophth/10235/ on 04/30/2017 Table. Clinical Characteristics of Patients With KPro Patient No./Sex/ Indication for Age, y Original KPro Other Ocular Diagnoses Previous Failed Corneal Surgeries Pseudophakia, PK ⫻4 glaucoma 1/F/27 Peter anomaly 2/M/57 Neurotropic, Pseudophakia, No prior vascularized retinal tear corneal ⫻2, surgery cornea with scar after hypotony decompensation OD, with silicone after vitrectomy oil Peter anomaly Glaucoma PK ⫻2 3/F/2 4/F/74 Neurotrophic cornea after graft needing valve for IOP control Ruptured globe 5 y prior, glaucoma, herpes simplex Patch graft for corneal perforation Preop VA Before Any KPro Time Before Membrane Seen/ Removed, Supplementary mo YAG CF 2 ft 3/4 CF 1 ft 4/10 VA Before KPro Explantation Original KPro Back Final VA Plate (Time After Diameter, Second KPro, mm; Material mo) 3 mo: 40 CF 2 ft 8.5; Titanium pulses at 2.8 mJ, failed 20/400 8.5; PMMA 7 mo:18 pulses at 3 mJ but then recurred after 6 wk No Roving eye 7.0; Titanium movements Roving eye 4/5 movements (toddler) No HM Not seen clinically, discovered when descemetocele repaired at 5 mo 20/70 8.5; Titanium 20/100 (4); No membrane seen 20/200 (2); Trace membrane Not noted (child) (1 d) HM (2.5); developed hypotony, sterile vitritis, choroidal effusions, no membrane Abbreviations: CF, count fingers; HM, hand motions; IOP, intraocular pressure: KPro, keratoprosthesis; OD, right eye; PK, penetrating keratoplasty; PMMA, polymethyl methacrylate; Preop, preoperative; VA, visual acuity. on gross examination, a delicate membrane was detected. All patients received a second KPro except for patient 3, who underwent a revision with a penetrating keratoplasty because of thinning at the surgical site and the primary need for tectonic stability. LIGHT MICROSCOPIC, ELECTRON MICROSCOPIC, AND IMMUNOHISTOCHEMICAL FINDINGS All cases were first examined and dissected under the grossing microscope, which revealed a fibrous membrane that emanated from the edges of the donor cornea on the anterior surface of the KPro. This membrane had an omnidirectional growth pattern in the anterior chamber, in addition to wrapping around the edge of the back plate and extending along its posterior surface to obscure the optical axis. Possible growth through holes in the retrocorneal titanium plate could not be evaluated because this material could not be sectioned. The membrane was composed of an inner layer of opaque fibrous tissue and an outer pigmented layer. In all cases, the fibrous membranes were found to be adherent to the back plate and required gentle, persistent traction to peel away, suggesting indirectly some growth and protrusion of the membrane within the holes in the back plate. In 2 cases, the connections between the retro-KPro membrane and the donor cornea were well preserved after processing and staining of the tissue. On low-power microscopy, the gap left by the KPro back plate between the donor cornea and retro-KPro membrane was evident (Figure 2A). The retro-KPro membrane was com- posed of 3 layers: a corneal stromal fibrous membrane, the iris stroma and pigmented posterior neuroectoderm, and metaplastic lens epithelium and elements of its persistent capsule. Evaluation of the healed wound interface between the host and donor cornea (Figure 2B) demonstrated that the fibrous retro-KPro membrane originated from the hypercellular host side and not the quiescent hypocellular donor aspect of the wound. Surface epithelial invasion of the wound, even partway, was not discovered. Adjacent sections disclosed gaps in the Descemet membrane; fragments of it had been displaced and swept along by the invading fibrous tissue (Figure 2C). The fibrous membrane adhered to, but did not invade, the friable and dissolving pigmented iris stroma. Despite the segmental disappearance of the stroma, the iris sphincter muscle was variably preserved (Figure 2D). The posterior pigmented neuroectodermal epithelium was observed to be displaced toward the pupil by traction (Figure 2E). The fibrous membrane extended toward the chamber angle as well as toward the pupil, where it merged with the metaplastic lens epithelium, capsular remnants, and its associated extracellular matrix (Figure 2D and E) to obscure the pupillary axis. New basement membranes that were brilliantly periodic acid–Schiff positive were generated by the metaplastic lens epithelium; they also contributed to the retro-KPro membrane in the pupillary zone (Figure 2D and E). The portion of the fibrous membrane that extended toward the chamber angle adhered to, and produced wrinkling of, the Descemet membrane (Figure 2E, inset). In 1 of the cases of a neurotrophic cornea (patient 2), moderate vascularization of the stromal membrane and (REPRINTED) ARCH OPHTHALMOL / VOL 129 (NO. 3), MAR 2011 312 WWW.ARCHOPHTHALMOL.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/ophth/10235/ on 04/30/2017 A B D D H 1 2 FM 3 C D FM S ∗ E C F H FM FM FM NE L Figure 2. Histopathologic and immunohistochemical features of retrokeratoprosthesis (retro-KPro) membranes. A, The donor cornea (D) above and the fibrous membrane (1) below delimit the empty space occupied by the back plate of the KPro (double-headed arrow). In addition to the fibrous downgrowth (1) from the corneal stroma making a “U” on the left (arrow), also seen are the disrupted iris (2) and the metaplastic lens epithelium with its capsule (3). B, Higher magnification of the host-graft junction (arrow) discloses origination of the fibrous membrane (FM) from the hypercellular stroma of the host’s cornea (H). The donor (D) corneal tissue at the interface is sharp and paucicellular. C, In adjacent sections, fragments of the Descemet membrane (arrows) have been displaced and trapped within the stromal downgrowth as it wraps around the KPro back plate to abut the underlying iris (*). D, Periodic acid–Schiff stain demonstrates growth of the fibrous membrane (FM) above the iris sphincter muscle (S) to merge on the right with the metaplastic lens epithelium and capsular remnants. The iris stroma has completely atrophied and been replaced by a thin scar. The thicker native lens capsule (arrows) contrasts with the thinner new basement membrane (crossed arrow) that has formed around clusters of metaplastic lens epithelial cells. E, Periodic acid–Schiff stain highlights the fibrous retro-KPro membrane (FM), displaying moderate vascularization (arrows). A remnant of the iris sphincter is seen within the iris stroma (crossed arrow). The lens capsule with metaplastic lens epithelium (L) lies posterior to the iris. The pupillary region (toward the bottom, right) has been plugged by a combination of the fibrous membrane, displaced posterior neuroectodermal iris pigmented epithelium (NE), and metaplastic lens epithelial membrane (L). Inset: In peripheral regions, the fibrous membrane (FM) adheres to the Descemet membrane (arrow) and through contraction pulls it away from the host cornea (H) to cause undulations. F, Top panel: The retro-KPro fibrous membrane (FM) is positive for smooth muscle actin. Note smooth muscle actin positivity in the deep corneal stroma (C) above the Descemet membrane (arrows). Bottom panel: The retro-KPro membrane is negative for pancytokeratin. (A-C, toluidine blue, original magnification ⫻25, ⫻100, and ⫻100, respectively; D, E, and E inset, periodic acid–Schiff, original magnification ⫻25; F top and bottom, immunoperoxidase reaction, original magnification ⫻100.) (REPRINTED) ARCH OPHTHALMOL / VOL 129 (NO. 3), MAR 2011 313 WWW.ARCHOPHTHALMOL.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/ophth/10235/ on 04/30/2017 A P N R R 2.0 µm, ×10 500 B LE C R R 5 µm, ×4600 there was an inflammatory response evidencing a plethora of neutrophils. Immunostaining with SMA in this membrane also revealed many myofibroblasts and nonpancytokeratin-staining cells. Actin positivity was also observed in surviving metaplastic lens epithelial cells in the 2 specimens displaying this feature. Electron microscopy of the retro-KPro fibrous membrane from a patient with Peter anomaly revealed an abundance of elongated myofibroblasts (Figure 3A). These cells had dichotomously branching rough endoplasmic reticulum and scattered thin (actin-type) subplasmalemmal cytoplasmic filaments with fusiform densities but betrayed no basement membrane formation. The extracellular space separating these cells was uniformly composed of collagen fibers. Examination of the most posterior layer of the membrane showed small, rounded lens epithelial cell groupings adjacent to the lens capsule (Figure 3B). Thin actin cytoplasmic filaments were also discerned in these cells along with abundant parallel profiles of rough surface endoplasmic reticulum. The cells were insulated from the matrix by surrounding, relatively prominent basement membranes that were not synthesized where adjacent epithelial cell membranes approximated each other (Figure 3B, inset). The extracellular matrix enveloping these cell clusters was amorphous, granular, and fibrillar and contained cellular detritus. M COMMENT 5 µm, ×2600 Figure 3. Transmission electron microscopy of the fibrous retrokeratoprosthesis (retro-KPro) membrane. A, Electron micrograph of the retro-KPro fibrous membrane demonstrates an elongated resident fibroblast without a basement membrane. It is endowed with abundant rough endoplasmic reticulum (R) and contains cytoplasmic subplasmalemmal filaments (arrow) with fusiform densities (crossed arrow). A delicate fibroblast cell process (P) is seen nearby. N indicates nucleus. B, Electron micrograph of a portion of the retro-KPro membrane composed of the lens epithelial cells (LE) found adjacent to the thick native lens capsule (C). The cells contain myriad parallel profiles of rough endoplasmic reticulum (R) and display subplasmalemmal thin actin-type filaments (crossed arrows in main panel and inset). The cells are surrounded by a prominent basement membrane (arrows). M indicates extracellular fibrillogranular matrix containing degenerated cell remnants. (A, electron micrograph, original magnification ⫻10 500; B and inset, electron micrograph, ⫻2600 and ⫻4600.) the iris surface was observed (Figure 2E). Vascularization of the retroprosthetic fibrous membrane emanated from the host’s, not the donor, corneal stroma. The fibrous component of the retro-KPro membranes of all 4 specimens stained positively for SMA (Figure 2F, top panel), with positive vessel walls serving as internal controls. The deep pre-Descemet keratocytes also expressed SMA (Figure 2F, top panel). Pancytokeratin staining, which immunoreacts with surface squamous epithelium and corneal metaplastic endothelium,11 was negative in the membrane (Figure 2F, bottom panel). The amount of intramembranous inflammation in our cases varied. Two retro-KPro membranes did not evince any significant inflammation. One patient with Peter anomaly (patient 1) had focal infiltrates of chronic inflammatory cells unrelated to vascularization. Finally, 1 patient with a neurotrophic scarred cornea and a descemetocele (patient 4) displayed a retro-KPro membrane with myxoid cellularity and a loosely woven collagenous appearance; The development of a retro-KPro membrane can be a sight-limiting complication to an otherwise successful solution for managing refractory corneal opacification. Even in initially successful YAG membranotomies, recurrence is possible because there is no deterrent to ongoing robust fibroplasia. These were the situations in 2 of our cases, which were among the most severe membranes encountered in our study. We have demonstrated that retro-KPro membranes, specifically those that are dense enough to resist YAG membranotomy, can be composed of multiple layers that include (1) a compact fibrous membrane behind the back plate consisting of stromal downgrowth from the host’s cornea; (2) the patient’s native iris stroma in varying states of preservation, which tightly adheres to the posterior surface of the membrane; and (3) a retroiridial membrane stemming from the metaplastic lens epithelium that synthesizes the matrix and merges with the anterior chamber retrocorneal fibrous membrane at the pupil to becloud it. In patient 4, who had an antecedent corneal perforation and a later descemetocele, the retro-KPro fibrous membrane was relatively thin and myxoid with an acute inflammatory reaction. This membrane had not been observed clinically (acuity was 20/70 at the time of explantation) and was only encountered on gross examination of the explanted KPro. In all other cases, the fibrous membranes were well collagenized, with minimally inflamed matrices that included mild vascularization originating from the host’s side of the wounded corneal stroma. The composition of the retro-KPro membrane may therefore vary, depending on antecedent clinical events. In the more recalcitrant membranes, the dense tissue had fused with (REPRINTED) ARCH OPHTHALMOL / VOL 129 (NO. 3), MAR 2011 314 WWW.ARCHOPHTHALMOL.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/ophth/10235/ on 04/30/2017 the anterior border layer of the iris stroma to cause the latter’s distortion, dissolution, and focal necrosis but did not invade it. Care must therefore be taken to remove all membranous components during excisions to clear the pupillary obstruction. Another earlier report of explanted Boston KPros described 4 fibrous membranes with epithelial migration partway into the wound,8 which was not observed in our case material. Different clinical features may help to explain the disparate incidences of epithelial downgrowth reported in the earlier and present studies. Autoimmune or inflammatory disease, which was present in 3 of the 4 previous patients with reported epithelial downgrowth, can promote intense vascularization of the retrocorneal stromal membrane that in turn can lend support to an epithelial downgrowth.12-16 Therefore, both stromal and epithelial anterior chamber invasion can develop together. None of our patients had systemic or local inflammatory conditions but were instead treated for developmental abnormalities or neurotrophic scarred corneas. The latter condition is known to be associated with defective corneal wound healing, which could be conducive to fibrous ingrowth around a prosthesis. In our opinion, another factor (besides inflammation) more likely contributes to membrane formation. Breaks in the Descemet membrane and displacement of Descemet fragments seen in our samples support the view that they allowed a pathway for migration of the host stroma into the anterior chamber. In our series, stromal downgrowth was only observed at these sites; furthermore, stromal cellularity was much more prominent on the host’s side of the corneal wound than on the donor’s side. As the host stroma swells, it can override the lateral border of the KPro back plate, and the fibrous ingrowth may then proliferate around this edge to cover the posterior aspect of the back plate. Myofibroblasts have been shown to arise from differentiated stromal keratocytes that are stimulated following corneal wound formation.17,18 The breaks in the Descemet membrane during the KPro surgery may trigger mechanisms for the ingrowth of myofibroblasts and the synthesis of extracellular membranous components, such as collagen and glycosaminoglycans.18-23 The specimens in our series stained negatively for pancytokeratin, a marker that is identified in retrocorneal membranes derived from epithelial downgrowth.11,24 Various cytokeratins can also be expressed along with SMA in damaged or metaplastic endothelial cells,11,25 but this cellular source for our membranes was ruled out by negative immunohistochemical staining for keratin. Similar results establishing a stromal source have been obtained in studies of retrocorneal membranes following penetrating keratoplasties.13,18,19,22 The presence of stromal myofibroblasts in our cases was confirmed by electron microscopy in accord with prior studies.17,18 The myofibroblasts displayed sufficient contractility to produce wrinkling of the Descemet membrane and displacement of its fragments,11 as shown in 2 of our specimens. The second component of our patients’ membranes was the coparticipation of remnants of lens capsule and epithelium. The epithelium underwent metaplasia and elaborated an extracellular collagenous matrix while still pre- serving ultrastructural features of an epithelium with the acquisition of thin cytoplasmic actin filaments. Patients 1 and 2 were pseudophakic before their initial KPro surgery (Table); it is possible but unprovable that the lens epithelium that comingled in membrane formation at the pupil had already begun to undergo metaplasia before the introduction of the KPro. Close approximation of the stromal wound is also a requirement to deter the fibrous downgrowth seen in the formation of retro-KPro membranes. The possibility of an unusually thick host peripheral cornea in the 2 patients with Peter anomaly leading to wound misalignment is intriguing but was not explored with preoperative anterior segment ultrasonography. A general redesign of the back plate (flange) so that it is 9.5 mm in diameter (1.0 mm greater than the current design) could conceivably clamp the corneal wound to a more marked degree, thereby creating a more effective barrier to stromal invasion. However, it would not completely abort the wound response, which stimulates migrating myofibroblasts. Other interventions requiring in-depth evaluation that may decrease retro-KPro membrane formation should focus on antiangiogenesis and antifibroplastic agents. Bevacizumab and its analogs may not be helpful in the context of stromal fibrous membranes if there is a paucity of neovascularization but may withhold support for epithelial and/or fibrous downgrowth and impede membrane formation in the subset of patients with ocular inflammatory conditions. Because of the rarity and random character of tissue availability represented, this study has 2 important limitations. While the surgeries were performed at the same institution, the participation of 2 different primary surgeons introduced an uncontrolled variable in surgical technique. The inclusion in this study of only 2 clinical entities furthermore does not reflect the full range of possible pathologic reactions, a subject that deserves further investigation as more varied tissues become available. Submitted for Publication: May 20, 2010; final revision received July 24, 2010; accepted July 28, 2010. Correspondence: Frederick A. Jakobiec, MD, DSc, Massachusetts Eye and Ear Infirmary, 243 Charles St, Ste 321, Boston, MA 02114 ([email protected]). Financial Disclosure: None reported. REFERENCES 1. Doane MG, Dohlman CH, Bearse G. Fabrication of a keratoprosthesis. Cornea. 1996;15(2):179-184. 2. Khan BF, Harissi-Dagher M, Khan DM, Dohlman CH. Advances in Boston keratoprosthesis: enhancing retention and prevention of infection and inflammation. Int Ophthalmol Clin. 2007;47(2):61-71. 3. Zerbe BL, Belin MW, Ciolino JB; Boston Type 1 Keratoprosthesis Study Group. Results from the multicenter Boston Type 1 Keratoprosthesis Study. Ophthalmology. 2006;113(10):1779, e1-e7. 4. Chew HF, Ayres BD, Hammersmith KM, et al. Boston keratoprosthesis outcomes and complications. Cornea. 2009;28(9):989-996. 5. Aldave AJ, Kamal KM, Vo RC, Yu F. The Boston type I keratoprosthesis: improving outcomes and expanding indications. Ophthalmology. 2009;116(4):640651. 6. Dunlap K, Chak G, Aquavella JV, Myrowitz E, Utine CA, Akpek E. Short-term visual outcomes of Boston type 1 keratoprosthesis implantation. Ophthalmology. 2010;117(4):687-692. (REPRINTED) ARCH OPHTHALMOL / VOL 129 (NO. 3), MAR 2011 315 WWW.ARCHOPHTHALMOL.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/ophth/10235/ on 04/30/2017 7. Bradley JC, Hernandez EG, Schwab IR, Mannis MJ. Boston type 1 keratoprosthesis: the University of California Davis experience. Cornea. 2009;28(3):321327. 8. Dudenhoefer EJ, Nouri M, Gipson IK, et al. Histopathology of explanted collar button keratoprostheses: a clinicopathologic correlation. Cornea. 2003;22(5): 424-428. 9. Bhat PV, Jakobiec FA, Papaliodis G, Sobrin L. Primary T-cell lymphoma of the retina and cerebellum: immunophenotypic and gene rearrangement confirmation. Am J Ophthalmol. 2009;148(3):350-360. 10. Jakobiec FA, Mehta M, Iwamoto M, Hatton MP, Thakker M, Fay A. Intratarsal keratinous cysts of the Meibomian gland: distinctive clinicopathologic and immunohistochemical features in 6 cases. Am J Ophthalmol. 2010;149(1): 82-94. 11. Jakobiec FA, Bhat P. Retrocorneal membranes: a comparative immunohistochemical analysis of keratocytic, endothelial, and epithelial origins. Am J Ophthalmol. 2010;150(2):230-242, e2. 12. Burris JE, Nordquist R, Rowsey JJ. Model of epithelial downgrowth, I: clinical correlations and light microscopy. Cornea. 1983;2(4):277-287. 13. Chen SH, Pineda R II. Epithelial and fibrous downgrowth: mechanisms of disease. Ophthalmol Clin North Am. 2002;15(1):41-48. 14. Chalam KV, Chokshi A, Agarwal S, Edward DP. Complications of AlphaCor keratoprosthesis: a clinicopathologic report. Cornea. 2007;26(10):1258-1260. 15. Lifshitz T, Oshry T, Rosenthal G. Retrocorneal membrane after penetrating keratoplasty. Ophthalmic Surg Lasers. 2001;32(2):159-161. 16. Mortemousque B, Dorot N, Poirier L, Williamson W, Brousse D, Verin P. Com- 17. 18. 19. 20. 21. 22. 23. 24. 25. plication of keratoprosthesis of posterior fixation: retroprosthetic membranes: apropos of 4 cases. J Fr Ophtalmol. 1995;18(10):608-613. Jester JV, Petroll WM, Barry PA, Cavanagh HD. Expression of alpha-smooth muscle (alpha-SM) actin during corneal stromal wound healing. Invest Ophthalmol Vis Sci. 1995;36(5):809-819. Cockerham GC, Hidayat AA. Retrocorneal membrane with myofibroblasts after perforating injury: an immunohistochemical and ultrastructural study of 11 cases. Cornea. 1999;18(6):700-706. Sherrard ES, Rycroft PV. Retrocorneal membranes, I: their origin and structure. Br J Ophthalmol. 1967;51(6):379-386. Sherrard ES, Rycroft PV. Retrocorneal membranes, II: factors influencing their growth. Br J Ophthalmol. 1967;51(6):387-393. Obata H, Tsuru T. Corneal wound healing from the perspective of keratoplasty specimens with special reference to the function of the Bowman layer and Descemet membrane. Cornea. 2007;26(9)(suppl 1):S82-S89. Kurz GH, D’Amico RA. Histopathology of corneal graft failures. Am J Ophthalmol. 1968;66(2):184-199. Banik R, Novick LH, Smith RE, Chuck RS. Retrocorneal membrane with Descemet’s detachment. Cornea. 2001;20(7):763-764. Prasher P, Muftuoglu O, Hsiao ML, Bowman RW, Hogan RN, Mootha VV. Epithelial downgrowth after Descemet stripping automated endothelial keratoplasty. Cornea. 2009;28(6):708-711. Pineda R II, Jain V, Gupta P, Jakobiec FA. Descemet’s stripping endothelial keratoplasty: an effective treatment for toxic anterior segment syndrome with histopathologic findings. Cornea. 2010;29(6):694-697. Visit www.archophthalmol.com. You can send an e-mail to a friend that includes a link to an article and a note if you wish. Links will go to short versions of articles whenever possible. (REPRINTED) ARCH OPHTHALMOL / VOL 129 (NO. 3), MAR 2011 316 WWW.ARCHOPHTHALMOL.COM ©2011 American Medical Association. All rights reserved. Downloaded From: http://archfaci.jamanetwork.com/pdfaccess.ashx?url=/data/journals/ophth/10235/ on 04/30/2017