Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
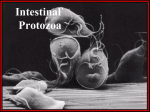
Protozoa (原虫) General Account • One-cell animal – monocellular or unicellular organisms with full vital functions • Species – total named species:65,000; parasitic: around 10,000 Classification of protozoa Amoebae Flagellates Sporozoa Ciliates Life cycle patterns One-host form 1. One stage form – Trophozoite 2. Two stage form – Trophozoite & Cyst Two-host form 1. Mammals 2. Mammals mammals insect vectors • Mode of Reproduction Asexual Reproduction Binary fission – result in 2 daughter cells Schizogony – multiple fission result in multiple cells Budding • Exogenous budding - by external budding result in multi- cells Endodyogony - by internal budding result in 2 cells Sexual Reproduction Conjugation – exchange of nuclear material of 2 Gametogony – sexually differentiated cells unite -- zygote Pathogenesis • Host Resistance – Innate immunity – Acquired immunity • Parasite Invasion – Toxin – Mechanically damage – Immune impair • Immune inhibition • hypersentivity Opportunistic & Accidental (protozoa) infections Opportunistic parasites • Opportunistic infection – An infection by a microorganism that normally does not cause disease but becomes pathogenic when the body's immune system is impaired and unable to fight off infection Amoebic Infections Entamoeba histolytica Acanthamoeba Naegleria Epidemiology • 4th leading cause of death from parasitic diseases worldwide Organism # of deaths/yr # infected Entamoeba ~75,000 ~300 million Ascaris Schistosoma Plasmodium (Malaria) ~200,000 ~750,000 2-3 million ~480 million ~200 million ~500 million • Amoebiasis is not restricted to the tropics and subtropics, it also occurs in temperate and even in arctic and antarctic zones Contaminated water is a source of infection. Infection is common in developing countries where sanitation is poor. Amoeba in alimentary tract • Entamoeba – – – – – E. E. E. E. E. histolytica (pathogenic) dispar (non-pathogenic) coli (big sister) hartmani (little brother) gingivalis (oral) • Endolimax nana (occasionally pathogenic) • Iodamoeba butschlii Morphology Entamoeba histolytica Cysts Trophozoites Thick wall Plasmalemma (thin) 1-4 ring-like nuclei 1 ring-like nucleus Chromatoid body (blunt) Lacking Round, 10-16 μm Irregular, 10-60 μm Concentratable Labile Morphology Ingested RBC Endoplasma Ectoplasma Nucleus with central karyosome and finely divided chromatin granules Pseudopod E. histolytica trophozoite Morphology Trophozoites Single nucleus with a central, dot-like karyosome Micrograph of a trophozoite ingesting a red blood cell deprived from its host. Morphology 1-4 ring-like nuclei with finely divided peripheral chromatin Cyst wall and round shape Mature E. histolytica Cyst Morphology Morphology E. Coli trophozoites • E. Coli cysts • Morphology E. histolytica Stages - CYSTS • Infective Stage for humans • Resistant walls maintain viability – If moist can last several weeks – Killed by desiccation or boiling • Diagnostic Stage in formed stools – Can be concentrated and stained easily – Not seen in liquid (diarrheic) stools or tissues E. histolytica Stages - TROPHOZOITES • Cause amoebiasis (damage tissue) • Spread throughout the body, but ... – Rarely transmit the infection to others • Labile in liquid stools or tissue, and – must be rapidly found or preserved (quick fixation & cold storage) for Diagnosis Life cycle Life cycle • Humans acquire E. histolytica by: – Ingesting cysts (4 nuclei mature) in fecally contaminated food or water – Rarely by directly inoculating trophozoites into colon or other sites – (anal sex?) • Fecal-Oral transmission (hand to mouth) Life cycle • The basic generation-cycle: cyst – lumen trophozoites – cyst • Trophozoites may invade intestine and spread • Cyst formation – essential factors: enviroment + time • Infective cysts and trophozoites pass in feces Pathogenesis General Types of Virulence Factors: • Adherence factors • 260kDa Gal/GalNAc lectin • Invasion factors • Amoeba pores • Cysteine proteinases • Endotoxins Pathogenesis Trophozoites ... – Attach to mucosal epithelial cells (MEC) – Lyse MEC – Ulcerate and invade mucosa – Cause dysentery (diarrhea + blood) – Metastasize via blood &/or lymph to – Form abscesses in extraintestinal sites ... Clinical Classification of Amoebiasis (World Health Organization) • Asymptomatic Infection:"Cyst Passers/carrier” • Symptomatic Infection: – Intestinal Amoebiasis: (colon and rectum盲肠、 升结肠、直肠、乙状结肠和阑尾) • Acute Dysenteric (dysentery) • Chronic Non-Dysenteric (“self-cured”) – Extra-Intestinal Amoebiasis: • Amoebic Liver Abscess (ALA) • Amoebic Pulmonary Abscess • Other sites (brain, skin, GU, ?) Clinical classification • Asymptomatic infection (carrier) >90% (E. dispar?) • Symptomatic cases <10% – 8% -10% dysentery, colitis, etc – 2% invasive amoebiasis – 0.1% deaths Clinical manifestation Acute Dysenteric Amoebiasis Symptoms: Bloody mucoid diarrhea RBCs and few WBCs in stools – Abdominal pain – weight loss – bloating, tenesmus(里急后重) and cramps Clinical manifestation Acute Dysenteric Amoebiasis Signs: Fever (33%) Tender (enlarged) liver Stools positive for trophozoites +/- WBC NO cyst in loose stools Clinical manifestation • Pinpoint lesion on mucous membrane Flask-shaped crateriform ulcers Pathological changes in large intestine Clinical manifestation Chronic Non-Dysenteric Amoebiasis “self-cured” carrier state Usually for 1 year, 37% symptomatic >5 years Intermittent diarrhea, mucus, abdominal pain, flatulence and/or weight loss E. histolytica trophs in loose stools Cysts in solid stools Positive serology and ulcerations on sigmoidoscopy or pathologic test Clinical manifestation Extra-Intestinal Amoebiasis Amoebic Liver Abscess (ALA) • Symptoms – History of dysentery (1 yr), weight loss, abdominal pain, chest or shoulder pain • Signs – fever, hepatomegaly – Diagnostic aspiration:non-odorous, reddish-brown in color aspirate (chocolate jam) "anchovy paste" – Might find trophozoites in the aspirate – Skin inflammation Clinical manifestation Ulcers caused by invasion of E. histolytica into the liver. Clinical manifestation • Clinical manifestation An Amoebic Liver Abscess Being Aspirated. • Note the reddish brown color of the pus (‘anchovy-sauce’). This color is due to the breakdown of liver cells. Gross pathology of amoebic abscess of liver. Tube of "chocolate" pus from abscess. Clinical manifestation X-ray of Amoebic Liver Abscess • Diagnosis • Pathogenic diagnosis – Stool examination: • Direct Fecal Smear (trophs and cysts) • Fecal concentration and iodine dye techniques (cysts) ZnSO4 or formalin-ether – Cultivation – DNA detection – Sigmoidoscopy • Serologic Tests (for chronic disease): ELISA, IHA (indirect hemagglutination) • Imaging: X-ray; CT Stool examination specimen method diseases remarks trophozoite cyst loose feces solid feces direct smear with normal saline direct smear with iodine stain amoebic dysentery chronic intestinal amoebiasis or carriers 1.container must clean 2.examined soon after they have been passed. 3.select bloody and mucous portion. Two microscopically indistinguishable Entamoeba sp. • E. histolytica – invades tissues – should always be treated • E. dispar – is non-pathogenic, even in AIDS – should not be treated Treatment of Amoebiasis • For invasive forms: metronidazole • For luminal forms: Iodoquinofonum, paromomycin, diloxanide • Do not treat asymptomatic intestinal E. dispar infection Treatment of Amoebiasis Location Clinical Class Drug Name Drug Action Asymptomatic Iodoquinofonnum(喹碘方) lumenal amebicide Mild to moderate intestinal disease Metronidazole(甲硝唑) tissue amebicide Severe intestinal disease Metronidazole plus a lumenal drug both Hepatic disease Metronidazole plus a lumenal drug both Intestinal Extraintestinal Prevention & Control • Individual measures • Diagnosis and treatment of E. histolytica patients • Safe drinking water (boiling or 0.22 µm filtration) • Cleaning of uncooked fruits and vegetables • Prevention of contamination of foods • Chemotherapeutic Trial Prevention & Control Community measures – Public services and utilities • Adequate disposal of human stools • Safe and adequate water supply – Primary health care systems • Health education (washing hands, cleaning and protecting food, controlling insects) • Specific surveillance programs and Control programs integrated into ongoing sanitation & diarrhea control – Health Regulations • Control of food vendors and food handlers • Control of flies and cockroaches Infections with Free Living Amoebae Naegleria 耐格里属 Acanthamoeba 棘阿米巴属 Free Living Amoebae Not seen in humans Naegleria i 10-35 µm (smaller than A. spp.) i with lobate pseudopodia i 15-45 µm with filiform pseudopodia Acanthamoeba cysts & trophs are seen in humans Acanthamoeba spp. Acanthamoeba trophozoites with acanthopodia Primary Amoebic Meningoencephalitis PAME An acute suppurative infection of the brain and meninges that is rapidly fatal and usually not diagnosed antemortem – Caused by Naegleria fowleri – Headache, lethargy and olfactory problems – Sore throat, runny nose, severe headache, vomiting, stiff neck, confusion leading to ... – Coma and death DIAGNOSIS PAME • Patient History (child) – Prior Health Excellent – Recent History of Swimming (fresh water/pools) – Cases peak during HOT months • Symptoms/Signs – Sore throat, runny nose, headache, vomiting, stiff neck, mental confusion, olfactory problems, lethargy, coma and death Treatment – None effective - few patients survive – Amphoteracin B +/- ? PAME Granulomatous Amoebic Encephalitis GAE A more slowly progressive, chronic form of the disease not associated with swimming (except in hot tubs) • cause: Acanthamoeba castellanii • history of subcutaneous nodules, eye or skin infection, progressive nasal congestion, headache ... • CNS lesions with negative serology for toxoplasmosis • in debilitated/immuno-compromised Pts with CD4+ TL <200/mm3 • disseminated infection: skin, sinuses, lungs, CNS/CSF Pathology GAE • abscesses/lesions (tissues) have – granulomatous inflammation – hemorrhagic necrosis and vasculitis – trophozoites & cysts with wrinkled-walls! • amoebae rarely seen in CSF Treatment GAE • No satisfactory or effective treatment ? – amphotericin B Acanthamoeba Keratitis AK Corneal infection with Acanthamoeba spp. trophozoites & cysts • Ulcerations & “Ring Infiltrate” of cornea • Induced by – trauma to eye, exposure to contaminated H2O – contact lens wear with tap water rinsing AK • Diagnosis – Examine corneal scrapings or smear – Histopathologic examination of cornea • Treatment – Triple Antiamoebic Therapy • neomycin-polymyxingramicidin/propamidine/miconazole – Penetrating keratoplasty (cadaver cornea) Plasmodium (疟原虫) History Malaria is an old infectious disease. The first documentation about it is at 1500BC. Until the end of the 19th century, it was commonly thought that malaria was caused by breathing bad air (mal-aria) and was associated with swamps History Important application of the knowledge about malaria: W. Gorgas successfully implemented control strategies for malaria and yellow fever during the construction of Panama Canal Global distribution Plasmodium that infect human Malaria current status Morphology • Plasmodium is the one-cell parasite, so the basic morphology is a nucleus (chromatin), cytoplasma and cell membrane • Wright or Giemsa stain gives the Cytoplasm – bluish; Chromatin - red to red-purple while the malarial pigments are yellow-brown • There are three stages and six main forms of plasmodium in RBC Plasmodium in RBC Trophozoites (滋养体期):ring form and developing trophozoites Schizonts (裂殖体期):immature and mature -- merozoites Gametocyte (配子体期): Microgametocytes and macrogametocytes Trophozoites • Fig. 1: normal red cell; Figs. 2-5: ring stage parasites (young trophozoites) Ring form trophozoites Thin blood film (Giemsa stained) • Ring like plasma with one nucleus at one side Mature trophozoites (amoeboid form) • The plasmodium grow with pseudopods, more cytoplasma and malarial pigment presented in the plasma • Red blood cell enlarged and became pale with Schüffner‘s dots(薛氏小点) Schizonts • Figs.: increasingly mature schizonts Macrogametocyte (female gametocyte) of P.v • Giemsa staining • compact nucleus, usually at edge of the parasite • scattered pigment granules • The gametocyte is completely filling its host cell Microgametocyte (male gametocyte) of P.v • Giemsa staining • large nucleus at the center of the cell • scattered pigment granules Macrogametocyte of P. f • The crescent-shaped gametocytes of P. falciparum are very distinctive, but tend to only appear late in the infection • Compact nucleus, red, usually at the center of the cell • Malarial pigments around the nucleus Microgametocyte of P. f • Sausage-shaped with two blunt end • Large nucleus at the center • Sometimes hard to distinguish from the female gametocytes exo-erythrocytic stage— merozoites in liver cells The vector – female Anopheles Development in the vector Gametocytes sporozoites zygote oocyst Life Cycle Life cycle • Infective stage:sporozoites • Transmission – – – – female Anopheles mosquito transfusion transplacental needle stick • Pathogenic stages:erythrocytic stage • Diagnositic stages:erythrocytic stage Pathogenesis Clinical features Incubation period (潜伏期) • Time interval between the mosquito bite and the onset of the clinical symptoms • Time for the sporozoite reaching liver and entering • Duration of the development in the liver • Time of development in the RBC to produce sufficient erythrocytic merozoites to cause clinical symptoms – P. falciparum 7 to 27 days – P. vivax 8 to 31 days – P. malarie 18 to 40 days – P. ovale 16 to 18 days Clinical features Typical malaria paroxysm(发作) Malarial paroxysm -symptom for erythrocytic phase – RBCs rupture releasing merozoites, malarial metabolites, endotoxin in blood – shaking chill(寒战) followed by fever (高热) (2-20 hrs) – profuse sweating when fever breaks(出汗退热) – repeated characteristic cycle for each species P. falciparum 36-48hrs P. vivax 48hrs P. malariae 72hrs P. ovale 48hrs Recrudescence versus relapse • Recrudescence (再燃) is the return of the symptom of malaria after apparent cure, which is due to a sudden increase in what was a persistent, low-level parasite population in the blood. – The periodic increase in numbers of parasites results from a residual population persisting at very low levels in the blood after inadequate or incomplete treatment of the initial infection. – The asymptomatic situation may last for as long as 53 years. Recrudescence versus relapse • Victims may suffer relapse (复发)after apparent recovery of malaria. This is caused by the long prepatent sporozoites (LPPs) or hypnozoites which remain dormant in the hepatocytes for an indefinite period. – P. vivax and P. ovale will develop hypnozoites in the liver responsible for relapse while patients infected with P. falciparum and P. malariae have no phenomenon of relapse • All four types of plasmodium can maintain low level of parasitemia and account for the recrudescence of the disease Clinical features • liver & spleen damage of long-term • complications from P. falciparum –Anemia – tropical splenomegaly syndrome –cerebral malaria - 50% of deaths •coma and renal failure due to tubular necrosis tropical splenomegaly syndrome Cerebral malaria Diagnosis • Travel history to endemic area & presence of symptoms, e.g., fever and chills • Thick smears - hard to read • Thin smears - see RBC morphology and parasite characteristics • serology - helps rule out fever of unknown origin • DNA probes- too slow & costly esp. in field Diagnosis Thick blood smear Thin blood smear Indirect fluorescent antibody test (IFA) DNA--PCR • Lane S: molecular base pair standard (50-bp ladder). Black arrows show the size of standard bands. • Lane 1: P. vivax (size: 120 bp) • Lane 2: the red arrow shows the P. malariae (size: 144 bp) • Lane 3: P. falciparum (size: 205 bp) • Lane 4: P. ovale (size: 800 bp) Treatment • Quinidine, chloroquine, primaquine, pyrimethanime, sulfadoxine, mefloquine, tetracycline, proguanil • affect parasite in different ways depending on stage when administered • different species react differently • emergence of drug-resistant malaria Prevention and control • Personal protection- netting, repellents, etc. • mosquito control or eradication - not easy • avoid sharing needles • develop vaccines - not currently available • select proper treatment for species and morphological forms