Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neonatal infection wikipedia , lookup
Infection control wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Sjögren syndrome wikipedia , lookup
Multiple sclerosis research wikipedia , lookup
Hygiene hypothesis wikipedia , lookup
Psychoneuroimmunology wikipedia , lookup
Multiple sclerosis signs and symptoms wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
DNA vaccination wikipedia , lookup
Management of multiple sclerosis wikipedia , lookup
Hepatitis C wikipedia , lookup
Hepatitis-2015
Orlando, USA
July 20 - 22 2015
Ehab Abd-El-Atty
HBV: Challenges to
cure in the future
Prof, Ehab Abd-El-Atty
Professor of Internal Medicine &
Gastroenterology & Hepatology &
Endoscopy
Faculty of Medicine, Menoufia University
Agenda
Epidemiology HBV
Natural history of HBV
Screening of HBV
Phases of chronic HBV
Prophylaxis of HBV
Treatment of HBV
Monitoring during therapy
Epidemiology
2 billions worldwide had past HBV
infection at a time
350 millions Chronic HBV
40.000 new cases each year
750,000 annual deaths are
attributed to HBV complications
HBV is the second known
carcinogen after smoking
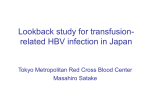
Geographical distribution of chronic HBV
HBV genotypes
Ten HBV genotypes (A-J).
Genotypes A and D results in higher rates of
chronicity than genotypes B and C.
Genotypes C and D have lower rates of
spontaneous HBeAg seroconversion as
compared with genotype A and B.
Genotype C and D are associated with
cirrhosis and HCC.
Genotype A and B shows better responses to
IFN-based therapy than genotypes C and D.
Natural history of HBV
Acute HBV
5-10% chronic HBV.
20% cirrhosis within 5 years (not treated)
20% decompensated cirrhosis within 5
years & HCC (not treated).
5 years survival will be 20%.
mass
Risk factors for progression to cirrhosis
Viral factors
Host Factors
High HBV DNA levels
Older age
HBV precore mutant
Male gender
HBV genotypes C & D
Advanced fibrosis
External Factors
Persistent ALT elevation
Recurrent hepatitis flares
HDV, HCV, HIV
coinfections
Obesity & steatosis
Alcohol
Risk factors for HCC development
Viral factors
Host Factors
High viral load
Older age
(≥ 104 copies/mL)
Male gender
HBV genotypes B &C
HBV mutations (preS,
precore, core promoter
region)
Advanced fibrosis
External Factors
Persistent ALT elevation
Recurrent hepatitis flares
HDV, HCV, HIV
coinfections
Obesity & steatosis
Cirrhosis
Low albumin & high
bilirubin
Alcohol
Aflatoxin
Family
history of
HCC
Who should be screened for HBV
Hyperendemic areas (Asia, Africa,
European Mediterranean)
Sexual contacts with HBV persons
Individuals infected with HCV or HIV
Renal dialysis
Pregnant women
Chronic elevation of ALT or AST
Family history of HCC or HBV
Before Anti TNFᾳ therapy
Serological Markers of HBV Infection
HBsAg
Acute/Chronic infection
Anti-HBc IgM
Recent infection
HBeAg
High infectivity
Anti-HBe
Low infectivity
Anti-HBs
Immunity
Anti-HBc IgG + HBsAg
Chronic infection
Anti-HBc IgG + anti-HBs
Resolved infection
Acute HBV
HBeAg +ve
HBsAg +ve
Anti-HBc IgM +ve
HBV DNA PCR +ve
Spontaneously resolution
90-95% adult
80% children
50% infants
10% neonates
Treat only acute fulminant hepatitis
Chronic HBV
Phases
Immune tolerant
HBe Ag +ve Immune active
HBe Ag –ve Immune active (Immune
escape)
Carrier
Occult
Egypt (90% genotype D)
(90% HBeAg -ve) (72% PCR +ve)
Immune Tolerant Phase
First 10-30 years of perinatally
acquired HBV infection
Asymptomatic
High HBV DNA levels but normal
ALT
HBe Ag +ve
HBe Ag +ve Immune Active Phase
Either after long years from perinatal
transmission or shortly after person to
person transmission
Relatively lower HBV DNA levels (>2000
IU/ml) with elevated ALT
HBe Ag +ve
Annual rate of spontaneous HBe Ag loss is
10%
It ends by seroconversion of HBe Ag
HBe Ag -ve Immune Active
Phase (Immune escape)
It is the late immune active
phase
HBe Ag -ve (precore mutation)
High serum HBV DNA
Elevated ALT
Carrier State
HBe Ag -ve, anti-HBe +ve
Serum HBV DNA < 2000 IU/ml
Persistently normal ALT for at least
one year
HBs Ag <1000 IU/ml
1% annual rate of spontaneous loss of
HBs Ag
Risk stratification for reactivation
Occult Chronic Hepatitis B
HBs Ag -ve
HBs Ab -ve
HBe Ag -ve
PCR <200 IU/ml
Normal ALT
HBc IgG Ab +ve
Serum hs-HBsAg could assist differentiation of occult
HBV patients from individuals with only past HBV
exposure.
Prophylaxis
Vaccine available 1982 worldwide
1992 in Egypt
Neonates of HBV +ve mother should
receive HBV immunoglobulin (HBIG)
and vaccine in the first 12 hours post
natal.
Screening for HCC every 6 month by US ±
AFP
Each HBsAg-positive should be screened
for anti-HDV
Treatment AASLD 2014 (40% require
treatment)
Goals of treatment
Long-term suppression of HBV
replication
Decrease hepatic necroinflammation
and fibrosis to prevent progression to
cirrhosis, liver failure and HCC.
In future (clearance of HBs Ag &
cccDNA {covalently closed circular DNA})
Candidates treated
HBe Ag +ve or -ve immune active phases i.e. with
PCR < 2000 and elevated ALT or with moderate to
severe liver inflammation ± fibrosis.
Cirrhotic patients with +ve PCR.
Carrier and occult HBV with +ve PCR under immune
suppression.
Acute fulminated HBV
Decompensated cirrhosis
Candidates not treated
Immunotolerant phase.
Carrier phase.
Occult phase.
Treatment options
Peg IFN (2005)
Nucleoside
Lamivudine (LAM) (1999)
Entecavir (2005)
Telbuvidine (2006)
Nucleotide
Adefovir (2003)
Tenofovir (2008)
Peg IFN
HBe Ag +ve only
HBe Ag Seroconversion at 24 w
Yes
No
Continue 48 w
Stop & shift to oral
Monitor during IFN therapy
CBC & liver profile /4 w
HBV DNA level / 12 w
HBs Ag 6-12 month after HBe Ag
seroconversion & undetectable HBV DNA
Response to Peg-IFN
Low viraemia & high ALT
Genotype A 47%
Genotype B 44%
Genotype C 28%
Genotype D 25%
HBe Ag –ve has poor response to
IFN.
Poor response in Egyptian patients with
predominant genotype D & HBe Ag –ve
HBe Ag -ve
Resistance to treatment is 15%,
therefore all Naïve patients are
candidates for the most potent drugs
with high barrier of resistance e.g.
Entecavir 0.5 mg or Tenofovir 300 mg
as a first line therapy.
Good response to therapy was found in
patients with detectable HBV DNA and
active inflammation
Tenofovir is preferred in:
Patients who received Lamivudine
previously.
Young women who plan to start a family.
Tenofovir is avoided in:
Decompensated & advanced cirrhosis
(renal impairment)
Entecavir is preferred in:
Older patients.
Patients with medical conditions that
increase risk of renal failure.
Patients already on treatment
Patients on regular Lamivudine or
combined Lamivudine & Adefovir
(undetectable HBV DNA) continue
treatment and HBV PCR every 3 to 6
months.
Newly developed resistance to
Lamivudine
Shift to Tenofovir.
Response to oral therapy
Entecavir
HBV PCR –ve in 70% after 1 year, 75% 2 year,
95% 5 year
HBe Ag seroconversion 30% after 2 year, 50%
after 5 year.
HBs Ag loss 1-2% every year
Tenofovir therapy
HBV PCR –ve in 93% after 3 year, 99% 6 year.
HBe Ag seroconversion 34% after 3 year, 50%
after 6 year.
HBs Ag loss 9 % after 3 year, 11% after 6 year
EASL 2015 Late breaking news
Combined Entecavir plus Tenofovir can
be used in HBeAg-positive with high
HBV DNA level
Peg IFN add-on to Entecavir results in
more sustained response
HBe Ag loss from 25% to 64%
ALT normalization from 25% to 79%
Duration of therapy
AASLD 2014 & EASL 2015 & APASL 2015
Ideal end point is sustained HBs Ag loss
and seroconversion into anti HBs Ab
+ve.
Peg IFN 48 week
In HBe Ag +ve patients, NA therapy can
be stopped 12 month after anti-HBe
seroconversion
life
long treatment in HBe Ag -ve
patients, HBe Ag +ve patients who did not
achieve seroconversion and cirrhotics.
Pitfalls of current therapy
Chronic suppression without cure
No HBsAg loss in most of patients.
Do not target defective immune
response and persistence of cccDNA in
the infected hepatocytes.
Emergence of drug resistance
Lamivudine resistance occurs at one
level only (YMDD)
Entecavir & Tenofovir resistance occurs
at 3 levels
Future strategies to eradicate HBV
AASLD 2014 & EASL 2015 & APASL 2015
Targeting the host
Immune therapy
Targeting the virus
Inhibitors of cccDNA formation
Inhibitors of HBV entry into the
hepatocyte
Immune therapy (AASLD 2014)
HBV-specific T cell impairment leads to failure
of HBV clearance,
Mechanism (improve impaired immunity
against HBV and can eradicate
cccDNA)
Thymosin-α1 (APASL)
Oral 1.6 mg twice weekly
Augments host Th1 immune response
HBV DNA–ve & HBeAg seroconversion
& normal ALT in 40%
Oxymatrine (APASL)
Suppress HBV replication (enhance
degradation of HBV mRNA)
Normalization of serum ALT 83%
HBeAg seroconversion 40% of patients
IFN-λ
Potent anti-HBV activity in vitro and in
transgenic mice
GS-9620 (oral agonist of TLR-7)
Prolonged suppression of HBV DNA in
serum and liver (HBV Ag +ve
hepatocytes)
Prolonged suppression of serum
HBsAg, HBeAg and.
It increases production of IFN-α and
various cytokines and chemokines.
Inhibitors of cccDNA formation (AASLD)
cccDNA plays a central role in HBV
infection persistence and its rebound
after stop of therapy.
In order to clear HBV, a durable,
curative antiviral therapy that directly
reduces the level of cccDNA without
killing infected hepatocytes is needed.
They induced rapid and multi-log
regression of viral DNA, HBsAg and
HBeAg with long duration of effect.
Inhibitors of cccDNA formation
Inactivation/elimination/degradation of
cccDNA.
Zinc-finger nucleases (ZFNs) directly
targets HBV cccDNA within cells (block
transcription of cccDNA).
CCC-0975 and CCC-0346, which were
confirmed as inhibitors of cccDNA
production,
ARC-520
Inhibitors of HBV entry into the hepatocyte
prevented viral spreading in between
hepatocytes, but also reduced levels of
HBV DNA, HBsAg and cccDNA.
Myrcludex-B is a synthetic lipopeptide
derived from the HBV envelope protein which
inactivates the HBV pre-S1 receptor (receptor
antagonists) and blocks HBV infection.
REP 9AC’, a nucleic acid-based polymer
which clears serum HBsAg by blocking HBV
subviral particle formation and release
(achieved seroconversion).
Targeting viral assembly/encapsidation
Bay 41-4109, inhibits viral replication
through inhibition or decrease stability
of normal capsids formation and
reduces half-life of the core protein.
It is active against HBV mutants resistant
to NAs.
Targeting HBs Ag secretion:
Antimicrobial nitazoxanide
It reduces extracellular HBsAg, HBeAg,
as well as intracellular HBcAg in a dosedependent manner.
It was a selective inhibitor of
intracellular HBV replication and
extracellular virus production, and
synergistic activity in combination with
Lamivudine or Adefovir
Targeting envelopment:
Glucosidase inhibitors
Inhibition viral morphogenesis and
infectivity.
They disrupt the development of HBV
envelope, thereby inhibit its ability to
bind target cells and establish infection.
Targeting viral mRNA
RNAi was able to inhibit all the steps of
HBV replication that occur in cell
culture and in mice.
Take home massage
HBV is the second known carcinogen
after smoking
Egypt (90% genotype D) (90% HBeAg ve)
Vaccination against HBV in infancy is
the most effective approach to prevent
HBV-related HCC
Neonates of HBV +ve mother should
receive HBV immunoglobulin and
vaccine in the first 12 hours post natal.
Goals of treatment
Suppression of HBV
replication
Decrease hepatic
necroinflammation and
fibrosis
Prevent progression to
cirrhosis, liver failure and HCC
Patients with minimal disease should
not be treated.
Patients at risk of developing
complications (cirrhosis & HCC) should
receive antiviral therapy
It is better to use the most potent drugs
with high barrier of resistance e.g.
Entecavir or Tenofovir as a first line
therapy.
All HBV patients must be screened for
HCC every 6 month by US ± AFP
Ideal end point of treatment is
sustained
HBs
Ag
loss
and
seroconversion into anti HBs Ab +ve.
In HBe Ag +ve patients, satisfactory
end point is seroconversion to HBe Ag
-ve.
life long treatment in HBe Ag -ve
patients, HBe Ag +ve patients who did
not
achieve
seroconversion
and
cirrhotics.
Egyptian patients with predominant
Genotype D had poor response Peg IFN
In Future
Combined Immune therapy and
antiviral therapy enhance
immunity and achieve
sustained control of infection,
improve impaired immunity
against HBV and can eradicate
cccDNA.
Meet the eminent gathering once again at
Hepatitis-2016
Dubai, UAE
October 17 - 19, 2016
Hepatitis– 2016 Website:
hepatitis.omicsgroup.com