Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
2661
Defibrillating Shocks Delivered to the Heart
Impair Efferent Sympathetic Responsiveness
Makoto Ito, MD; Harald P. Pride, BS; Douglas P. Zipes, MD
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
Background. Functional studies indicate that sympathetic efferents are located in the superficial
subepicardium and vagal efferents are located in the subendocardium. It is possible that electrical shocks
applied directly to the heart might affect the function of these autonomic nerves.
Methods and Results. Low- (<1 J), medium- (6 to 16 J), or high- (30 to 35 J) energy truncated
monophasic exponential shocks, synchronized to the R wave during sinus rhythm, were delivered over
implantable patches sutured inside the pericardium in anesthetized open-chest dogs. Shortening of
ventricular effective refractory period (ERP), produced by bilateral ansae subclaviae stimulation (SS),
was measured before and after shock delivery. High-energy shocks shifted the SS frequency-ERP response
curves downward and to the right (P<.001) for sites beneath and apical to the patches; ERP shortening
at basal sites remained unchanged. Such sympathetic attenuation occurred with shocks >10 J but not
with shocks < 10 J, was noted 15 minutes after the shock, and showed incomplete return to control values
at 3 hours. Neither low- nor high-energy shocks affected norepinephrine dose-ERP response curves,
indicating normal myocardial responsiveness. Low- and high-energy shocks did not attenuate bilateral
cervical vagal stimulation-induced ERP prolongation. High-energy shocks delivered over patches sutured
to the outside of the pericardium showed no effects on sympathetic response, suggesting a protective effect
of the pericardium against shock-induced sympathetic attenuation.
Conclusions. DC shocks >10 J delivered directly to the epicardium attenuated efferent sympathetic
neural function. Such changes may affect electrophysiological, as well as hemodynamic, responses to
sympathetic neural stimulation after cardioversion-defibrillation. (Circulation. 1993;88:2661-2673.)
KEY WoRDs * DC shock * electrodes * effective refractory period * autonomic neural function
Implantable cardioverter-defibrillators using epicardial patch systems effectively cardiovert ventricular tachycardia and defibrillate ventricular fibrillation.1"2 Antitachycardia devices undergoing clinical
investigation deliver discharges that can be set from 0.1
to 34 J.3 Excessive voltages cause myocardial damage,4-8
the extent of which correlates with shock strength and
shock intervals in experimental animals.5,7,8 Repeated
electrical shocks over implantable patches induce
pathological changes in humans.9 Electrical shocks affect central and peripheral nerves, altering neural function transiently, permanently, or progressively.10-12
We have shown that sympathetic efferent fibers are
located within the superficial subepicardium, while efferent vagal nerves en route to the ventricle cross
superficially at the atrioventricular groove and are then
concentrated in the subendocardium.13""4 Electrical
shocks over epicardial patch electrodes could influence
the function of these autonomic nerves and alter the
response that sympathetic and vagal stimulation produces in the myocardium. However, little is known
about the effects of DC shocks on efferent sympathetic
or vagal function to the heart. The purpose of this study
was to determine if the electrical shocks delivered
Received April 6, 1993; revision accepted June 28, 1993.
From the Krannert Institute of Cardiology, Indiana University
School of Medicine, Indianapolis, Ind.
Correspondence to Dr Douglas P. Zipes, Krannert Institute of
Cardiology, 1111 West 10th St, Indianapolis, IN 46202.
through an epicardial patch system modulated efferent
sympathetic and vagal function to the myocardium.
Methods
Surgical Preparation
Fifty-nine mongrel dogs of either sex weighing 20 to 36
kg were anesthetized with pentobarbital (30 mg/kg IV).
Additional amounts of pentobarbital were given as necessary to maintain anesthesia during the study. The dogs
were ventilated by means of a cuffed endotracheal tube
and volume-cycled respirator (model 607, Harvard Apparatus, South Natick, Mass). The chest was opened through
a median sternotomy. A fluid-filled catheter was placed in
the left femoral artery and connected to a transducer
(Statham P-23 Db, Gould, Cleveland, Ohio) to monitor
arterial blood pressure. The left femoral vein was cannulated to infuse normal saline at 100 to 200 mL/h to replace
spontaneous fluid losses. Dogs were placed on a heating
pad, and the thoracotomy was covered by a plastic sheet.
A thermistor (model 400, Yellow Springs Instrument,
Yellow Springs, Ohio) was used to monitor epicardial
temperature. An operating room table lamp was used to
maintain epicardial temperature at 36 to 38°C. Arterial
blood gases and pH were monitored and maintained
within the physiological range.
Patch Electrode Placement
The small size oval epicardial patch electrode (model
6871, the surface area of electrode=17 cm2, Medtronic
Inc, Minneapolis, Minn) was sutured to the inside of the
2662
Circulation Vol 88, No 6 December 1993
of the pericardium. When shocks were applied to the
heart, patches were fixed firmly over the heart surface to
create an even contact between patches and heart.
Cathodae
Anode
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
Electrode Placement for Measurement of Effective
Refractory Period
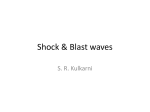
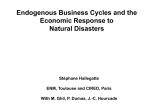
Using a 25-gauge needle, two hook electrodes made
from Teflon-coated wires, insulated except for their tips,
were placed in the left ventricular midmyocardium basal
to the left epicardial patch. Two electrodes were inserted in the left ventricular midmyocardium beneath
the patch, and three additional electrodes were inserted
in the left ventricular midmyocardium apical to the
patch (Fig 1). The electrodes served as the cathode for
unipolar stimulation to determine effective refractory
periods (ERPs). An anodal electrode consisting of a
33-mm-diameter metal disk was placed in the abdominal wall. A bipolar plunge electrode was inserted in the
myocardium of the right ventricular outflow tract to
record the ventricular responses. Another bipolar
plunge electrode was inserted in the myocardium of the
right ventricular apex and connected to the external
defibrillator unit. Data collection began 30 minutes
after the placement of the plunge electrodes.
Measurement of Effective Refractory Period
The ERP was determined at each electrode site by the
extrastimulus technique employing a programmable
stimulator (Krannert Medical Engineering, Indianapolis,
Ind) and a constant current isolator. Each ventricular test
site was driven with a 2-msec rectangular stimulus twice
diastolic threshold, which was measured during each
intervention. A train of eight stimuli (S1) was followed by
a late premature stimulus (S2) that produced a propagated ventricular response. The S1-Si interval was 230 to
240 msec and was kept constant throughout the experiment. The ventricular responses to S1 and S2 were
recorded from lead II ECG and from a right ventricular
FIG 1. Diagram of heart. Solid circles indicate sites of
plunge electrode placement; shaded areas, placement of
patch electrodes; AO, aorta; LA, left atrium; LAD, left
anterior descending coronary artery; LV, left ventricle; PA,
pulmonary artery; RA, right atrium; and RV, right ventricle.
pericardium overlying the left anterolateral ventricular
epicardium and served as the cathode. A second patch
electrode was sutured to the inside of the pericardium
and positioned over the right lateral ventricular wall and
served as the cathode (Fig 1). In groups 1 through 10,
the patches were positioned inside the pericardial sac.
In group 11, the patches were positioned on the outside
TABLE 1. Delivered Energy, Leading-Edge Voltage, Leading-Edge Current, Duration, Tilt, and Impedance of Truncated
Exponential Monophasic Shock Waves
Group 1 (N=6)
Delivered Shock Energy,
J (range)
Low:
0.90±0.01 (0.88-0.92)
30.8±+1.4 (25.0-33.7)
Low:
0.86±0.07 (0.54-1.00)
High: 31.6±3.1 (16.4-35.8)
Low:
0.88±0.05 (0.76-1.15)
High: 32.3±1.6 (23.3-35.8)
35.0+0.9 (31.8-38.4)
6.3±0.4 (5.8-7.4)
9.8±0.04 (9.7-9.8)
Low:
0.49±0.02 (0.43-0.52)
Medium: 15.7±0.5 (13.7-17.3)
15.9±2.5 (12.4-20.9)
High:
Group 3 (N=6)
Group 4 (N=7)
Group 5
Group 6
Group 7
Group 8
(N=7)
(N=3)
(N=3)
(N=6)
LeadingEdge
Voltage, V
138+1.5
771+ 12
LeadingEdge
Current, A
1.92+0.08
12.0+0.5
137±0.4
2.16±0.1
773+11
13.5+0.8
1.98+0.05
12.0+0.4
141+±0.7
767+6.5
765±4
339± 14
419±3
133±1.7
745±9
527±43
Group 9 (N=3)
16.3+0.4 (15.7-17.0)
764+8
Group 10 (N=3)
30.1±1.3 (25.8-33.6)
786±9
Group 11 (N=6)
Values are mean+SEM. N indicates number of test dogs.
12.2±0.4
5.5±0.6
Duration,
m8
7.8±0.2
7.4±0.4
7.0±0.5
6.9±0.6
Tilt, %
57±2
59± 1
64±2
62±1
8.2+0.6
66+1
76+3
8.0±0.4
8.5±0.3
62±0.4
63±2
62±0.4
61±2
8.1+±0.5
63+0.2
64+5
8.1 ±0.3
63±1
66±0.4
62±0.2
62±1
63±2
6.8+0.2
1.96+0.09
11.9+0.4
4.9±0.1
8.5±0.8
7.9+0.1
11.7+0.4
4.1+±0.1
10.3±0.4
8.4±0.8
4.0+0.1
62±1
61±2
Impedance,
(1
76+2
63±2
68+3
58±4
73+2
62±2
62±1
64+1
77±3
Ito et al DC Shocks and Autonomic Neural Function
bipolar electrogram and displayed on a storage oscilloscope. The S1-S2 interval was shortened in steps of 2
msec until S2 failed to produce a propagated ventricular
response. The S1-S2 interval was then increased by 5
msec and was shortened by 1-msec decrements until S2
failed to produce a propagated ventricular response. The
ERP was defined as the longest S1-S2 interval at which
S2 failed to produce a propagated response. The ERPs
were determined twice, and values were within 1 msec of
each other or the data were discarded and the determination was repeated.
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
Neural Stimulation
The ansae subclaviae were isolated bilaterally as they
exited from the stellate ganglia, doubly ligated, and cut.
The cervical vagi also were isolated bilaterally, doubly
ligated, and transected. Shielded bipolar electrodes
were placed on the right and left anterior and posterior
ansae subclaviae to stimulate the efferent cardiac sympathetic nerves with a stimulator (model SD-88, Grass
Instrument Co, Quincy, Mass). Stimuli were rectangular
4-msec pulses delivered at a frequency of 1 to 4 Hz and
at 1.0 to 4.0 mA. Determination of the ERP was started
2 minutes after the onset of ansae subclaviae stimulation. The cervical vagi were stimulated through two
Teflon-coated wire electrodes embedded in the cardiac
end of the cut nerve. Rectangular pulses of 4-msec
duration were delivered at a frequency of 20 Hz. The
current strength was 0.05 mA greater than that required
to produce asystole (>2 seconds) for the right vagus and
asystole or complete atrioventricular block during spontaneous rhythm for the left vagus. The effects of efferent
vagal stimulation on ventricular ERP were determined
during intravenous infusion of norepinephrine at a rate
of 0.25 jig kg-'. min` to achieve a constant background of sympathetic effect. The conditions of neural
stimulation were kept constant in each experiment.
DC Shocks
DC shocks were delivered by using an external cardioverter/defibrillator (model 2394, Medtronic Inc, Minne-
2663
apolis, Minn). The amount of voltage charged to the
output circuit for delivery to the lead system was set at
130 to 800 V, and capacitance was 50 to 120 uF. Shocks
were synchronized to the R wave of the local electrogram
recorded from the right ventricular apex during sinus
rhythm. Delivered voltage and current waveforms from
the defibrillator unit were displayed on a storage oscilloscope (model 5223 Digitizing Oscilloscope, Tektronix,
Beaverton, Ore) and photographed. Shocks were
monophasic truncated exponential waveforms. Durations
were defined by the tilt setting of 65% (dial setting) in 55
dogs. In another 4 dogs (2 dogs in group 1 and 2 dogs in
group 11), durations were set at 8.0 msec.
Protocols
Effects of low- and high-energy shocks on ansae subclaviae frequency- and norepinephrine dose-refractory period
response relations. Group 1. To analyze the effects of
low-energy and high-energy shocks on the efferent sympathetic response, we obtained the ansae subclaviae
stimulation-ERP response (frequency-ERP response)
curves in 6 dogs. In each dog, the ERP was determined
in the baseline state and then during bilateral ansae
subclaviae stimulation at frequencies of 1, 2, and 4 Hz.
The order of stimulation frequencies was chosen randomly and given at 10-minute intervals. Ten minutes
after the final frequency-ERP response curve was obtained during the control state, a low-energy shock was
delivered. Fifteen minutes later, ERPs were determined,
and frequency-ERP response curves were again obtained. Then, 10 minutes later, a high-energy shock was
delivered, and frequency-ERP response relationships
were determined 15 minutes after the high-energy shock.
In 4 of 6 dogs, baseline ERP and ERP response to
norepinephrine infusion (0.5 ,ug * kg` * min-') were determined before low-energy shock (control state) and
after high-energy shock. ERPs were determined 5 minutes after initiation of norepinephrine infusion to allow
equilibration. Time interval between low- and highenergy
shocks was 60 to 70 minutes.
TABLE 2. Baseline Heart Rate and Mean Arterial Blood Pressure Before and After Shocks
Heart Rate, bpm
Mean Arterial Blood Pressure, mm Hg
Control
After Shock
Control
After Shock
Low energy
High energy
Low energy
High energy
114±2
117+1
Group 1 (N=6)
117±2
102±6
102±6
95±7
Sham (first)
Sham (second)
Sham (first)
Sham (second)
132±9
134±10
Group 2 (N=7)
135±8
112±5
109±4
106±3
Low energy
High energy
Low energy
High energy
117±2
122±2
Group 3 (N=6)
131±3
97±6
93±10
92±12
118±2
121±2
Group 6 (N=3)
96±11
95±15
130±8
Group 7 (N=3)
132±6
109±2
112±6
Low energy
Medium energy
Low energy
Medium energy
8
125±3
123±3
Group (N=6)
124±3
102±5
101±8
98±7
111±4
Group 9 (N=3)
113±7
104±3
107±4
116±3
Group 10 (N=3)
116±4
85±5
91±3
121±4
Group 11 (N=6)
118±2
108±4
111±4
Values are mean±SEM and were obtained during control period and 15 minutes after delivery of each shock. bpm indicates beats
per minute; and N, number of test dogs.
2664
Circulation Vol 88, No 6 December 1993
TABLE 3. Baseline Ventricular Effective Refractory Period Before and After Shocks
After Shock
Control
Ventricular Effective Refractory Period
High energy
Low energy
165±3
169±4
Basal sites (n=1 2)
169±4
Group 1 (N=6)
Group 2 (N=7)
Patch sites (n=12)
Apical sites (n=18)
169±3
Basal sites (n=14)
Patch sites (n=14)
Apical sites (n=20)
152±3
156±3
155±2
Basal sites (n=12)
Patch sites (n=12)
Apical sites (n=18)
Basal sites (n=6)
Patch sites (n=6)
Apical sites (n=12)
Basal sites (n=6)
Patch sites (n=6)
Apical sites (n=12)
154±2
159±2
159±1
159±2
161±2
160±1
162±4
161±2
162±2
171 ±2
171 +4
174+2
172±4
172±2
Sham (first)
Sham (second)
152±3
155±2
155±2
152±3
157±3
156+2
High energy
Low energy
Group 3 (N=6)
Group 6 (N=3)
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
Group 7 (N=3)
-
151±+2
157±2
158±+1
153±2
159+1
160+1
159±3
160±3
159±2
162±4
162±2
162±2
Low energy
Medium energy
160±1
158±1
155±1
Basal sites (n=12)
162±1
159±1
160±2
Patch sites (n=12)
160±1
158±2
Apical sites (n=18)
160±1
161±2
161±2
Basal sites (n=6)
Group 9 (N=3)
157±3
161±3
Patch sites (n=6)
158±2*
160±2
Apical sites (n=12)
156±6
153±5
Basal sites (n=6)
Group 10 (N=3)
156±5
156±6
Patch sites (n=6)
157±3
154±4
Apical sites (n=12)
160±1 *
157±1
Basal sites (n=12)
Group 11 (N=6)
164±2
160±2
Patch sites (n=12)
165±1*
160±1
Apical sites (n=18)
Values are mean±SEM and were obtained during control period and 15 minutes after each shock. N indicates
number of test dogs; and n, number of ventricular test sites.
*P<.05 vs control value.
Group 8 (N=6)
Group 2. Seven dogs just received patch implantation,
as in group 1 dogs, but no discharge of shocks. Ansae
subclaviae stimulation-ERP response curves were determined three times, using the same time intervals of
ERP determination as in group 1.
Group 3. The effects of low- and high-energy shocks
on myocardial response to norepinephrine infusion
were studied in 7 dogs. ERP was determined in the
baseline state and during intravenous infusion of
norepinephrine at doses of 0.1, 0.25, and 0.5
,ug kg`. min1. ERPs were determined 5 minutes
after initiation of each infusion. The order of doses
was chosen randomly and given at 10-minute intervals.
Ten minutes after determination of the last norepinephrine dose-ERP response curve during the control
period, a low-energy shock was discharged. Fifteen
minutes after the low-energy shock, norepinephrine
dose-ERP response curves were obtained. Then, 10
minutes later, a high-energy shock was delivered, and
norepinephrine dose-ERP response curves were determined 15 minutes later. Time interval between the
two shocks was 70 to 80 minutes.
Effects of Low- and High-Energy Shocks on
Refractory Period Response to Vagal Stimulation
Group 4. Effects of DC shocks on efferent vagal
responses were studied in 7 dogs. Baseline ERP and
ERP during bilateral vagal stimulation were determined
during control state, 15 minutes after a low-energy
shock, and 15 minutes after a high-energy shock. Time
interval between the two shocks was 30 to 40 minutes.
Ito et al DC Shocks and Autonomic Neural Function
A
I
-
0
(n=12)
(n=12)
2520-
15-
15-
10-
10-
10-
5
s-
CONTROL
LOW ENERGY
HIGH
ENERGY
-Y-
5-
0
0
[
B
4Hz
20-
P15
10-
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
CL
0.
-0
5-
W
2 HZ
20-
20-
15-
15-
10
10
5_
5
0
16 J. Bilateral
25-
25-
20-
20-
20
P 15.2
10-
15-
15
10-
10
5-
5
I
W
0
0.25
0.5
.
0.1
5
0.25
ansae
Effects of Leading-Edge Voltage and Current on
Refractory Period Response to Ansae Subclaviae
Stimulation for Medium-Energy Shocks
Groups 9 and 10. Effects of leading-edge voltage
0.5
or
current on efferent sympathetic responsiveness were
studied in 6 dogs receiving shocks of 16 J, which is an
just exceeding the threshold that attenuated
sympathetic responsiveness. Group 9 consisted of 3 dogs
that received a 16-J shock with a low leading-edge
voltage and current, while group 10 consisted of 3 dogs
that received a 16-J shock with a high leading-edge
voltage and current. Capacitance was 100 OtF in group 9
and 50 liF in group 10. Stimulus frequency of ansae
subclaviae stimulation-ERP response curves was determined before and 15 minutes after the shock.
energy
--{-
1
0.1
vs
subclaviae stimulation-ERP redetermined before and 15 minutes
after each shock. Methods and time intervals were the
same as in group 1.
CO
5-
4Hz
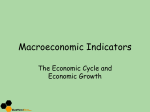
APICAL SITES
(n=18)
25-
0.
2Hz
response curves during control and 15 minutes after first
and second sham shocks from
7 dogs. High-energy shocks
shifted frequency-response
curves down and rightward.
Values are mean±SEM. n indicates number of test sites.
*P<.O01 control.
sponse curves were
PATCH SITES
(n=12)
(n=12)
1 Hz
re-
sponse curves at basal, patch,
and apical test sites. ERP
shortening (ordinate) in response to various stimulation
frequencies of bilateral ansae
subclaviae stimulation (abscissa) obtained during control, 15
minutes after low-energy
shock, and 15 minutes after
high-energy shock from 6
dogs (A). B, Similar frequency-
&
/
1 Hz
2Hz
4Hz
Frequenc,V of Ansae Subclaviae Stimuladiion
4 Hz
BASAL SITES
X
APICAL SITES
(n=20)
25
(n=14)
Time Effect of High-Energy Shocks on Refractory
Period Response to Ansae Subclaviae Stimulation
Group 5. The time course of alterations in sympathetic responsiveness after a shock was evaluated in 7
dogs. Baseline ERP and ERP during bilateral ansae
subclaviae stimulation were determined before and 15,
60, 120, and 180 minutes after a single high-energy
shock. The frequency of ansae subclaviae stimulation
was constant at 4 Hz. The ERP response to norepinephrine infusion (0.5 ,ug * kg1 min1) was obtained at the
end of the study in 6 dogs.
Effects of Shock Energy Level on Refractory Period
Response to Ansae Subclaviae Stimulation
Groups 6, 7, and 8. Twelve dogs in three groups were
studied to determine the threshold energy level that
attenuated sympathetic responsiveness. Group 6 consisted of 3 dogs receiving a single shock of 6 J; group 7
consisted of 3 dogs receiving a single shock of 10 J; and
group 8 consisted of 6 dogs receiving shocks of 0.5 and
g
.
.
0
4Hz
/s *
CONTROL
SHAM SHOCK 1
SHAM SHOCK 2
*
1 Hz
2Hz
PATCH SITES
25-
(n=14)
refractory period (ERP)
15
1 Hz
BASAL SITES
25-
(n18)
20-
0o
2Hz
1 Hz
FIG 2. Plots show ansae subclaviae stimulation-effective
APICAL SITES
25-
20
Co
0:
cc
PATCH SITES
BASAL SITES
25
2665
CONTROL
-0-
LOW ENERGY
*
HIGH ENERGY
0
0.1
Dose of Norepinephrine Infusion (,gg/kg/min)
0.25
0.5
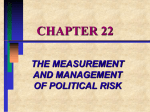
FIG 3. Plots of norepinephrine
dose-effective refractory period
(ERP) response curves. Shortening of ERP (ordinate) during intravenous infusion of norepinephrine
(abscissa) at basal, patch, and apical test sites obtained during control, 15 minutes after low-energy
shock, and 15 minutes after highenergy shock from 6 dogs. Values
are mean+SEM. n indicates number of test sites.
2666
Circulation Vol 88, No 6 December 1993
TABLE 4. Baseline Heart Rate, Mean Arterial Blood
Pressure, and Ventricular Refractory Periods During
Norepinephrine Infusion In Dogs That Received Shocks
and Vagal Stimulation In Group 4
After
After
LowHighControl
145±7
Energy
Shock
145±7
Energy
Shock
148±6
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
Heart rate, bpm (N=7)
Mean arterial blood pressure,
mm Hg (N=7)
154±5 154±8 153±6
Ventricular ERP, ma
Basal sites (n=14)
154±3 154±3 154±3
Patch sites (n=14)
154±3 156±3 157±3
Apical sites (n=21)
154±2 155±2 155±3
Values are mean±SEM and were obtained during intravenous
infusion of norepinephrine at a rate of 0.25 gg* kg-' * min1 to
achieve a constant background of sympathetic effect. ERP
indicates effective refractory period; N, number of test dogs; n,
number of ventricular test sites; and bpm, beats per minute.
Effects of High-Energy Shock Delivered Through the
Pericardium on Refractory Period Response to Ansae
Subclaviae Stimulation
Group 11. Effect of the patch electrodes positioned
outside the pericardium was tested in 7 dogs. Each dog
received a single high-energy shock over patches sutured to the outside of the pericardium. Ansae subclaviae stimulation-ERP response curves were determined
before and 15 minutes after high-energy shocks.
Analysis of Data
As reported in the previous studies,15,16 data from
ventricular test sites with less than 9-msec shortening of
the ERP elicited by bilateral ansae subclaviae stimulation at 4 Hz or less than 3-msec lengthening of ERP
induced by bilateral vagal stimulation during the first
control determination were excluded because of insufficient effects of neural stimulation at those particular
sites. Two dogs (one in group 1 and the other in group
11) were excluded from-the analysis because ventricular
fibrillation occurred after shocks.
Data were expressed as mean±SEM. Two-way repeated-measures ANOVA was used to compare the
ansae subclaviae stimulation frequency-ERP response
curves or norepinephrine dose-ERP response curves.
One-way repeated-measures ANOVA was used to compare effects of energy levels on vagal stimulationinduced ERP prolongation and time course of baseline
ERPs, hemodynamic data, or ansae subclaviae stimulation-induced ERP shortening after the shocks. A statistical significance was set at P<.05.
Results
Effects of Low- and High-Energy Shocks on Ansae
Subclaviae Frequency- and Norepinephrine
Dose-Refractory Period Response Relations
Calculated values for the various shock waveforms
are shown in Table 1. Blood pressure, heart rate, and
baseline ERP during control states and after shocks of
various energies are shown in Tables 2 and 3.
In group 1, low-energy shocks did not affect the ansae
subclaviae stimulation-ERP response curves at sites
basal to, beneath, or apical to the patches (Fig 2A).
However, high-energy shocks shifted the frequencyresponse curves downward and to the right at sites
apical to and beneath the patches but not at sites basal
to the patches (Fig 2A). Frequency-response curves
were unchanged in sham dogs (group 2, Fig 2B).
ERP shortening in response to norepinephrine infusion was 17.3±1.3 versus 16.8±1.3 msec at basal sites,
19.6±2.0 versus 19.1±1.8 msec at patch sites, and
20.3±1.6 versus 20.5±1.1 msec at apical sites during
control versus after high-energy shock (P>.5).
Norepinephrine dose-ERP response curves in group
3 are shown in Fig 3. Neither low- nor high-energy
shocks affected dose-ERP response curves at basal,
patch, and apical test sites.
Effects of Low- and High-Energy Shocks on
Refractory Period Response to Vagal Stimulation
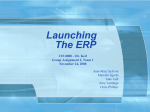
Table 4 shows the baseline ERP values of test sites
during norepinephrine infusion. Both low- and highenergy shocks did not affect the ERP prolongation
induced by bilateral vagal stimulation at sites basal to,
beneath, or apical to the patches in group 4 (Fig 4).
Time Effect of High-Energy Shocks on Refractory
Period Response to Ansae Subclaviae Stimulation
Heart rate, mean arterial pressure, and baseline
ERPs in group 5 are shown in Table 5. Baseline ERPs
at patch or apical test sites were unchanged (P>.1) over
time, while baseline ERPs at basal sites showed slight
prolongation (P<.01) after the shock. Fig 5 shows that
15 minutes after high-energy shocks, ERP shortening
induced by bilateral ansae subclaviae stimulation was
unchanged at sites basal to the patches but was attenuated at sites beneath and apical to the patches. ERP
shortening at patch and apical test sites in response to
ansae subclaviae stimulation was attenuated during a
3-hour period after delivery of the high-energy shock.
ERP shortening during norepinephrine infusion was
21.8±1.2 msec for basal sites, 21.5±0.8 msec for patch
sites, and 20.4±1.2 msec for apical sites (P>.7) 3 hours
after the shock.
We compared the time course of ERP response with
ansae subclaviae stimulation after a single high-energy
shock at individual test sites and dogs. After the shock,
no basal test sites showed ERP shortening in response
to ansae subclaviae stimulation that was <80% of
control values. ERP shortening at patch and apical sites
was attenuated 15 minutes after the shock in each dog
(Fig 6A), but the reduction of ERP shortening was
different among dogs (ERP shortening was 35±2% to
85±4% of control values 15 minutes after the shock).
ERP response returned to control value 180 minutes
after the shock in the dog that received a 33-J shock
(ERP shortening 15, 120, and 180 minutes after the
shock was 85±4%, 64±5%, and 104±7% of control
values, respectively; Fig 6A*). The dog that received a
38-J shock showed sustained attenuation of ERP response during a 3-hour period after the shock (ERP
shortening 15 and 180 minutes after the shock was
54±2% and 41±4% of control values, respectively; Fig
6At). In the other dogs, ERP response showed incomplete return to control values at 180 minutes (ERP
Ito et al DC Shocks and Autonomic Neural Function
APICAL SITES
(n=21)
BASAL SITES
C
Co
C
,E
0
-.
1..~
c
Low
High
c
Low
High
Delivered Ener
Level
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
shortening 15 and 180 minutes after the shock was
35±2% to 76±7% and 73±8% to 86+8% of control
values, respectively), but the restoration curves were
different among dogs.
Attenuation and restoration of ERP response after
the shock were different among test sites in each dog
(Figs 6B and 6C). In the dog that received a 33-J shock
(Fig 6B), ERP response in two patch sites and in two of
three apical sites was attenuated 15 minutes after the
shock but returned toward control values 30 minutes
after the shock (ERP shortening 15 and 30 minutes
after the shock was 29% to 41% and 71% to 75% of
control values, respectively). ERP response in one apical site showed delayed recovery (ERP shortening 15,
60, 120, and 180 minutes after the shock was 36%, 27%,
32%, and 50% of control value, respectively). In the dog
that received a 32-J shock (Fig 6C), ERP response in
one of two patch sites was almost unchanged (ERP
shortening
15 and 180 minutes after the shock
was
100%
and 94% of control values, respectively). ERP response
in the other patch site and in one of three apical sites
was attenuated 15 minutes after the shock but recovered
toward control values (ERP shortening 15 and 180
minutes after the shock was 74% to 83% and 83% to
84% of control values, respectively). ERP response in
two of three apical sites showed sustained attenuation
(ERP shortening 15 and 180 minutes after the shock
was 54% to 67% and 53% to 63% of control values).
C
Low
High
2667
FIG 4. Bar graphs showing effects of low- and high-energy
shocks on prolongation of effective refractory period (ERP) induced by bilateral vagal stimulation (ordinate) at basal (left),
patch (middle), and apical test
sites (right). ERP prolongation in
response to vagal stimulation
showed no change after low- or
high-energy shocks. C indicates
control; and n, number of test
sites.
Effects of Shock Energy Level on Refractory Period
Response to Ansae Subclaviae Stimulation
Medium-energy shocks of 16 J (group 8) shifted the
ansae subclaviae stimulation-ERP response curves at
patch (P<.022) and apical test sites (P=.003), while
shocks of 0.5 J (group 8), 6 J (group 6), or 10 J (group
7) did not (Fig 7). Ansae subclaviae stimulation-ERP
response curves were unchanged at basal test sites in
these three groups (not shown).
Fig 8 shows the relationship between energy level and
attenuation of ERP shortening in response to ansae
subclaviae stimulation after a single shock. Basal sites
showed no attenuation of ERP shortening at any energy
levels. ERP shortening in response to ansae subclaviae
stimulation was unchanged after single shocks of 0.5 to
10 J but was attenuated after single shocks of >10 J at
patch and apical test sites. Attenuation of ERP shortening after 16-J shock was similar to 35-J shock.
Effects of Leading-Edge Voltage and Current on
Refractory Period Response to Ansae Subclaviae
Stimulation for Medium-Energy Shocks
Parameters of shocks in groups 9 and 10 are shown in
Table 1. Delivered energy level was similar among
shocks that had low (group 9) and high (group 10)
leading edges of current (P>.05). Attenuation of sympathetically induced ERP shortening at patch and apical sites in response to ansae subclaviae stimulation was
TABLE 5. Time Course of Baseline Heart Rate, Mean Arterial Blood Pressure, and Ventricular
Effective Refractory Period Before and After DC Shock In Dogs That Received Single High-Energy
Shock In Group 5
After DC Shock, min
Control
15
60
120
180
119±4
Heart rate, bpm (N=7)
119±4
120±5
119±5
119±6
Mean arterial blood pressure,
mm Hg (N=7)
103±5
104±6
102±5
102±7
100±5
Ventricular ERP, ma
153±2
156±2*
157±2*
Basal sites (n=14)
157±2*
157±2*
157±1
159±1
157±1
Patch sites (n=14)
158±1
159±2
157±1
157±1
158±1
158±1
158±1
Apical sites (n=21)
N
indicates
number
Values are mean±SEM;
of test dogs; n, number of ventricular test sites; and bpm, beats per
minute.
*P<.01 vs control.
0.
c
(c
W
20
IC
15'
0)
10'
5
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
:~ ~
Circulation Vol 88, No 6 December 1993
2668
0
C
c.5
I=
20
15
15
60
120
BASAL SITES
(n=14)
PATCH SITES
(n=14)
Effects of DC Shocks on the Response to Efferent
Sympathetic and Vagal Stimulation
180 min
1~~~~~~~~
10
APICAL SITES
(n=21)
a
CL
5
0
C
15
60
1
180
delivered directly to the epicardial surface attenuate
ERP shortening in response to ansae subclaviae stimulation at sites beneath and apical to the patch electrodes
but not at sites basal to the patch electrodes; low- and
high-energy shocks do not shift norepinephrine doseERP response curves at basal, patch, and apical test
sites; low- and high-energy shocks do not attenuate the
ERP prolongation produced by efferent vagal stimulation; a single high-energy shock attenuates ERP shortening in response to ansae subclaviae stimulation at
patch and apical test sites for as long as 3 hours;
threshold energy level that attenuated ERP shortening
induced by ansae subclaviae stimulation is 10 to 16 J;
both high and low leading-edge current shocks of 16 J
attenuate the ERP shortening in response to ansae
subclaviae stimulation; and pericardial placement of
patch electrodes seemed to protect against shock-induced attenuation of ERP shortening in response to
ansae subclaviae stimulation.
min
Time After DC Shock
FIG 5. Bar graphs show time course of shortening of
effective refractory period (ERP) induced by bilateral
ansae subclaviae stimulation at basal (top), patch (middle), and apical test sites (bottom) after a single highenergy shock in 7 dogs. Patch and apical sites exhibited
attenuation of ERP response to ansae subclaviae stimulation after high-energy shocks, while ERP response at
basal sites was unchanged. Values are mean±SEM. C
indicates control; and n, number of test sites. *ANOVA
P<.001 vs control.
similar among low and high leading-edge current shocks
(Fig 9).
Effects of High-Energy Shock Delivered Through the
Pericardium on Refractory Period Response to Ansae
Subclaviae Stimulation
Delivered energy, leading-edge voltage, duration, and
tilt in group 11 were similar (P>.05) to the high-energy
shocks of group 1 dogs with patches sutured inside the
pericardium (Table 1). Leading-edge current was lower
and impedance was greater in group 11 than in group 1
(P<.05). High-energy shocks delivered over patches
sutured outside of the pericardium did not affect ERP
response to ansae subclaviae stimulation (Fig 10).
Discussion
Major Findings
The major findings from this study are that single
high-energy truncated monophasic exponential shocks
Effects of countershock on the myocardium have
been evaluated, using histology,4-6'8 ECG mapping,5
enzymatic analysis,17 and scintigraphic methods.18'19 In
the present study, we demonstrated for the first time
that defibrillating shocks delivered over implantable
patches impair the refractory period response to efferent sympathetic stimulation but not efferent vagal stimulation in dogs. Sympathetic responsiveness was attenuated at patch and apical test sites but not at basal test
sites. Norepinephrine dose-ERP response curves did
not shift after high-energy shocks at any sites, indicating
that the responsiveness of the myocardium was normal
and unchanged.
We have shown previously that efferent sympathetic
nerves are located in the superficial subepicardium.13 It
is likely that electrical shocks impaired efferent sympathetic nerves at the position of patch electrodes because
attenuation of sympathetic response occurred only at
sites beneath and apical to the patch electrodes. The
ERP response was not attenuated at sites basal to the
patch electrodes. In contrast, high-energy shocks did
not alter ERP prolongation produced by vagal stimulation because vagal fibers are concentrated in the subendocardium13.14 and thus removed from contact with the
patch. Morphological studies indicate that damage by
transthoracic or epicardial shocks tends to be concentrated in the epicardial and subepicardial regions at the
site of electrode application.6'20 If the upper edge of the
patch had reached the atrioventricular groove before
vagal fibers dive to the endocardium,14 it is possible that
the shock might have affected vagal nerves as well.
Patients with implantable cardioverter-defibrillators
show shock-related pathological changes in myocytes
subjacent to the patch electrode.9 Morphological alterations after shocks are different between subepicardium
and subendocardium.6,20 Electrical countershocks cause
contraction abnormalities in subepicardial zones when
shocks are given directly to the epicardium but not in
the subendocardial zone.21 In a scintigraphic study, the
major component of technetium-99m uptake occurs in
the epicardial layers when shocks <50 J are applied
directly to the heart. A single shock 250 J induces
technetium-99m uptake in the subendocardial layers.22
Ito et al DC Shocks and Autonomic Neural Function
A
%
a*
1oo-
10
80-
cc
C.
E0
0 0 60CD)0
c
CO
1t
t§00 40a.
[
8
* .:
ol
.
Ca
*
a
15
120
60
180 min
C
B
100 -
28 8
80 -
a
(3c,
40 -
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
00o 40
PATCH SITES
*
....---- APICAL SITES
L8 20
aLI
o L_
j
i'
15 60O
20 fl
120;0 min
.
-",I-
15
Thus, single shocks <50 J mainly damage the subepicardial myocardial tissue, which is consistent with our
observation that a single shock s35 J affected the
epicardial and/or subepicardial region and attenuated
the sympathetic response. Subendocardial layers were
not affected by this energy level, as judged by the
preserved vagal response. Higher-energy shocks applied to the heart are probably necessary to produce
transmural damage and attenuate the vagal response.
the DC shocks have no sustained effects on such neurotransmitter release.23 For DC shocks to exert sustained effects on sympathetic responsiveness, as in the
present study, several mechanisms, alone or in combination, can be postulated. Electric shocks can damage
the subepicardial myocardium and cause diffusion of
metabolites from the injured tissue to affect the autonomic function16; electric shocks can damage the blood
10J
6J
--CO
-0*-
0.5 J and 16 J
(n=1 8)
(n=9)
(n=9)
20-
6J
15-
-0- CONTROL
-0.>- CONTROL
CONTROL
20-
-_*-- 10J
0.5 J
A
A~~ ~*
._
en)
CL
10-
0-
10-
5.
50
1 Hz
2 Hz
4Hz
16J
15-
15-
C,)
p-
1
vessels supplying the nerve axons; or electric shocks can
directly injure the sympathetic nerve axons.
Although we did not perform a histological examination of the heart, multiple shocks from 1 to 24 J
delivered directly to the heart using implantable patches
show only minimal pathological changes in dogs.24 Single defibrillation shocks with a cardioverter/defibrillator
showed no pathological cardiac changes, and multiple
shocks exhibited only superficial myocardial injury under the patch electrodes in humans.9
Electrical shocks impair myocardial anaerobic metabolism25 and increase myocardial potassium efflux without reduction of myocardial blood flow.26,27 However,
such metabolic changes are short, lasting only several
minutes.2",29 It is not likely that accumulation of these
metabolites affected sympathetic response for longer
time periods. Further, it is unlikely that metabolites
diffusing from such a small area of injured myocardium
caused sympathetic attenuation at much larger areas
located apically and beneath the patch electrodes.
Myocardial blood flow or coronary blood flow is
unchanged after transthoracic (200 to 460 J) or epicar-
Mechanisms of Shock-Induced Attenuation of
Efferent Sympathetic Response
Although transthoracic defibrillator shocks induce
the local release of acetylcholine and catecholamines,23
20-
FIG 6. Graphs show time course
of sympathetic responsiveness at
patch and apical test sites after a
single high-energy shock. Ordinate: Relative effective refractory
period (ERP) shortening in response to ansae subclaviae stimulation compared with control values in percentage. A, Plots of
iin: minutes after
shock at arrow
averaged values of two patch and
three apical test sites in each dog.
* and t, see text; § and #, ERP
changes in individual test sites are
shown in panels B and C, respectively. B and C, Changes of ERP
X
shortening at individual patch and
apical test sites in the dogs receiving a 33-J (B) and a 32-J shock
(C). Time course of ERP response
-- PATCH SITES after single high-energy shocks
--- ... APICAL SITES
was different among dogs and
.
.
among test sites in each dog.
60 120 180 min
.....
60 -
Ad
2669
1 Hz
2 Hz
4 Hz
1
1H~z
Frequency of Ansae Subclaviae Stimulation
2H~z
4H4z
FIG 7. Plots show bilateral ansae
subclaviae stimulation-effective refractory period (ERP) response
curves at apical test sites during control and 15 minutes after DC shocks
in 3 dogs that received shocks of 6 J
(left), in 3 dogs that received shocks
of 10 J (middle), and in 6 dogs that
received shocks of 0.5 J and 16 J
(right). Shocks of 0.5, 6, and 10 J did
not shift the frequency-ERP response curves, while shocks of 16 J
shifted the curve downward and to
the right. *P=.003. Format and abbreviations are as in Fig 2.
Circulation Vol 88, No 6 December 1993
2670
E100
90
CD
80C
0
o~
7020
o
30
4
Basal Sites
*
Patch and Apical
Sites
FIG 8.
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
level
Plot shows relationship between shock energy
(abscissa)
effective refractory
and
period
(ERP)
shortening in response to ansae subclaviae stimulation at
4 Hz after a single shock compared
percentage (ordinate).
with
control values in
Data were obtained from control
values and after first shock in groups 1, 5, 6, 7, 8, 9, and
10.
ERP
data
this figure.
after
a
Shocks
second shock were
>10 J
attenuated
not included in
ERP
response,
while shocks s10 J showed no significant effects on ERP
response to ansae subclaviae stimulation.
dial
shocks.19'21'30 However, myocardial
after high-energy shocks because
shocks >30 J but not shocks .30 J applied directly to
the heart reduce both thallium-201 uptake and myocardial blood flow to shock sites.22 These regional blood
flow changes could modulate autonomic neural func(5 to 75 J) DC
ischemia
might occur
1C
_D
0:
02
0
0.
0
10
cnCD02
10
WJ E0:
q
0
-
n=6 n=6
Basal
n=6 n=6
n=9 n=9
Patch
Apical
Test Sites
Low Leading Edge
Current Shock
High Leading Edge
Current Shock
FIG 9. Bar graph shows effects of low and high leadingedge current shocks of 16 J on effective refractory period
(ERP) shortening elicited by ansae subclaviae stimulation
(4 Hz) compared with control values in percentage.
Attenuation of ERP response after shock was similar
among low and high leading-edge current shocks at
patch and apical test sites.
tion. Although we did not measure myocardial blood
flow, reduction of regional myocardial blood flow probably does not play a major role in shock-induced sympathetic attenuation because 16-J shocks also attenuated sympathetic responsiveness in our study but do not
reduce myocardial blood flow.22
Vascular disorders are observed in dogs receiving
electrical defibrillation.4 DC shocks might damage vessels supplying the nerves and alter sympathetic function. However, the arterial supply to the sympathetic
and vagal nerves of the heart is not well established, and
we cannot entirely exclude this as a possibility.
In our study, some test sites beneath or apical to the
shock area showed marked sympathetic attenuation 15
minutes after shock delivery but recovered toward
control values over time after a single high-energy
shock. These results indicate that shock-induced sympathetic attenuation can be a transient event, probably
functional in origin at some sites. Electrical shocks to
peripheral nerves cause functional changes in nerve
impulse conduction.11 Excessive amounts of electric
current injure the nerves and produce morphological
damage due to the high electric energy10 and may have
been the responsible mechanism in our study.
Sustained Sympathetic Attenuation After
High-Energy Shocks
Restoration of nerve action potential after DC shocks
depends on the shock voltage and capacity of the
condenser.11 Shocks <200 V produce transient disturbances of nerve action potential, while discharges of 1000
V cause total block of nerve conduction followed by
action potential abnormalities lasting >60 minutes.
High-voltage shocks from small-capacity condensers
create greater disturbances than low-voltage shocks
from larger capacitors. The restoration kinetics following the high-voltage pulses are slower than for the
low-voltage pulses of the same energy.
In the present study, restoration of sympathetic responsiveness after high-energy shocks was observed at
some test sites exhibiting marked sympathetic attenuation but not at others. Some patch and apical test sites
showed no recovery during a 3-hour period. These
results might reflect excessively high energy delivery to
some sympathetic nerves because of local "hot spots"
around the edges of the patches that can occur following
the shock. Conceivably, the lack of recovery could also
reflect progressive neural damage following the initial
shock.
The current density at the edges and corners of the
electrodes is more dense than that within the body of
the electrodes.31 This so-called edge effect creates zones
of high current density limited to the edges of the
patches31,32 and could injure sympathetic nerves that lie
in the superficial subepicardium (depth .0.5 mm) when
the patch electrodes are applied directly to the epicardium. Because local current density beneath the shock
electrode is uneven,31-33 it might cause attenuation of
sympathetic responses at some sites beneath and apical
to the patch electrode but not at others. The fact that
vagal nerves are concentrated in the subendocardium,
far from such high current density areas, might be a
that shocks did not affect efferent vagal function.
If the patches were placed over the vagal nerves prior to
reason
Ito et al DC Shocks and Autonomic Neural Function
PATCH SITES
(n=12)
BASAL SITES
(n=12)
APICAL SITES
(n=18)
25-
25-
,am
0)
20-
20-
CD
15-
15-
10-
10-
._
0
c0
cc)
5-
5
W~
O-A
1 Hz
4 Hz
2 Hz A
(7-0- CONTROL
-I
1 Hz
2 z
AFTER SHOCK
4 Hz
2671
FIG 10. Plots show stimulus frequencies of bilateral ansae subolaviae stimulation versus effective
refractory period (ERP) responses
at basal (left), patch (middle), and
apical test sites (right) during control and 15 minutes after high-energy shock in 6 dogs with patches
sutured outside of the pericardium. High-energy shocks did not
affect frequency-ERP response
curves. Format and abbreviations
are as in Fig 2.
Frequency of Ansae Subclaviae Stimulation
their intramural course,14 vagal dysfunction likely would
have resulted as well.
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
Patches Outside the Pericardium Protect Against DC
Shock-Induced Attenuation of Efferent
Sympathetic Response
High-energy shocks applied to patches outside the
pericardium did not attenuate the ERP response to
sympathetic stimulation. These shocks had higher impedance and lower leading-edge current than did highenergy shocks over patches inside the pericardium.
Such high impedance reflects the electrical character of
the pericardium, which contains collagenous and elastic
fibers. Although the high impedance provided by the
pericardium might slightly reduce the energy reaching
the epicardium,m the pericardium is too thin to affect
the total shock energy very much. However, pericardium interposed between the patch electrodes and
epicardium might blunt the high current density zones
at the edges of the electrodes31,32 and reduce damage to
sympathetic nerves.
Methodological Consideration
We used only the small patch electrodes to replicate
the approximate patch-myocardium relationship
found in human defibrillator implants. The surface
area of implantable patches used in humans is 10 to 27
cm2,35,36 while the surface area of the patch electrodes
in our experiment was 17 cm2. Larger electrodes
reduce both the defibrillation threshold and average
current density and could decrease the myocardial
injury22'37-39 and perhaps the attenuation of sympathetic responsiveness as well. Larger electrodes would
not necessarily eliminate edge effects, however. Regardless, given the size of the canine heart, it was very
difficult to obtain both even contact with epicardium
and sufficient distance between the borders of the two
patches when using the medium size patch. Delivered
energy level (0.5 to 35 J) in the present study was
comparable with that of implantable cardioverterdefibrillators in humans.
Modeling studies of current distributions of defibrillating shocks show uneven current density near the
defibrillation electrode.27'33 Electrode configuration also
affects such current distribution,31 40 and electrodes of
different contours might have modified our results.
We sutured the patch electrodes to the pericardium
to avoid injury to the epicardium. We tried to maintain
firm and even patch electrode contact with the ventricular epicardium, but we were not able to exclude
poor contact at some points of the patch electrode.
Elevated ventricular wall temperature and myocardial
burns can occur at such sites after defibrillator
shocks41 and could account for irreversible sympathetic nerve injury. Overall patch contact was good
since our results showed impedance values similar to
those reported using conventional patch electrodes
(58 to 64 Q1 for medium- and high-energy shocks over
patches inside the pericardium).38
Higher currents delivered by smaller capacitors at
identical energy levels are arrhythmogenic,42'43 since
peak current rather than energy level determines the
extent of myocardial damage.43'44 In our study, high or
low leading-edge voltage and current shocks showed
similar effects on sympathetic attenuation at the same
energy level of 16 J. Leading-edge voltages between 527
and 764 V and currents between 8.5 and 11.7 A had no
significantly different effects on neural function. However, we cannot exclude more sustained sympathetic
attenuation with high leading-edge voltage shock because we measured the ERP response to sympathetic
stimulation only once.
Shock waveforms affect both defibrillation energy
and myocardial damage.2'45-47 Forty-joule damped sine
wave shocks attenuated efferent sympathetic response,
but 1-J shocks did not (authors' unpublished data).
Effects of other waveforms on sympathetic neural function need to be tested in the future.
Study Implications
Although arrhythmia induction was not tested in the
present study, regional sympathetic attenuation after
DC shock creates uneven efferent sympathetic actions
on the heart that could produce ventricular tachyarrhythmias.48 One of the causes of postoperative inhospital death after cardioverter-defibrillator implant
is incessant ventricular tachycardia/fibrillation.49 The
mechanism of this exacerbation of ventricular arrhythmia, so-called "VT storm," is unknown but could be
related to shock-induced heterogeneous sympathetic
attenuation. Furthermore, hemodynamic depression,
another known complication following cardioverterdefibrillator implantation, could be related to sympathetic neural depression. It is important to stress that
our data showed sympathetic neural attenuation after
only one high-energy shock. Initial energy levels to
2672
Circulation Vol 88, No 6 December 1993
cardiovert-defibrillate the heart sometimes exceed 15 J
in humans.2'50,51 Generally, a minimum of three such
shocks is necessary during cardioverter-defibrillator
implantation. The incidence of high defibrillation
thresholds is low, but such patients may need multiple
high-energy shocks.52 It is possible that nonthoracotomy cardioverter-defibrillator implantation may protect against shock-induced sympathetic attenuation
and may reduce arrhythmia and hemodynamic problems after cardioverter-defibrillator implant.
It is tempting to recommend that patches should be
implanted in patients on the outside of the pericardium,
based on the results from this study. However, as
always, caution must be exercised in applying observations from animals to patients. Placement of a patch
electrode outside the pericardium may result in phrenic
nerve damage and may increase the defibrillation energy.34 Also, it is possible that repeated shocks, even with
the pericardium interposed, might still attenuate sympathetic neural function.
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
Acknowledgments
Supported in part by the Herman C. Krannert Fund; by
grants HL-42370 and HL-07182 from the National Heart,
Lung, and Blood Institute of the National Institutes of Health;
US Public Health Service; and the American Heart Association, Indiana Affiliate, Inc. We thank Naomi S. Fineberg, PhD,
for statistical analysis and Jacob Rohleder, BS, for technical
assistance.
References
1. Mirowski M. The automatic implantable cardioverter-defibrillator:
an overview. J Am Coil Cardiol. 1985;6:461-466.
2. Winkle RA. The implantable defibrillator: progression from firstto third-generation devices. In: Zipes DP, Jalife J, eds. Cardiac
Electrophysiology: From Cell to Bedside. Philadelphia, Pa: WB
Saunders Co; 1990:963-969.
3. Klein LS, Miles WM, Zipes DP. Antitachycardia devices: realities
and promises. JAm Coll Cardiol. 1991;18:1349-1362.
4. Tedeschi CG, White CW. A morphologic study of canine hearts
subjected to fibrillation, electrical defibrillation and manual compression. Circulation. 1954;9:916-921.
5. Dahl CD, Ewy GA, Warner ED, Thomas ED. Myocardial necrosis
from direct current countershock. Circulation. 1974;50:956-961.
6. Warner ED, Dahl C, Ewy GA. Myocardial injury from transthoracic defibrillator countershock. Arch Pathol. 1975;99:55-59.
7. Babbs CF, Tacker WA, VanVleet JF, Bourland JD, Geddes LA.
Therapeutic indices for transchest defibrillator shock: effective,
damaging, and lethal electrical doses. Am Heart J. 1980;99:
734-737.
8. Patton JN, Allen JD, Pantridge JF. The effects of shock energy,
propranolol, and verapamil on cardiac damage caused by transthoracic countershock. Circulation. 1984;69:357-368.
9. Singer I, Hutchins BM, Mirowski M, Mower MM, Veltri EP,
Guarnieri T, Griffith LSC, Watkins L, Juanteguy J, Fisher S, Reid
PR, Weisfeldt ML. Pathologic findings related to the lead system
and repeated defibrillations in patients with the automatic
implantable cardioverter-defibrillator. JAm Coil Cardiol. 1987;10:
382-388.
10. Panse F. Electrical lesions of the nervous system. In: Vinken PJ,
Bruyn GW, eds. Handbook of Clinical Neurology. Amsterdam:
North-Holland Publishing Co; 1970:344-387.
11. Eickhorn R, Haverkampf K, Antoni H. Disturbances of neural
conduction in isolated frog nerves following exposure to strong
electric fields. Muscle Nerve. 1986;9:313-318.
12. Petty PG, Parkin G. Electrical injury to the central nervous system.
Neurosurgery. 1986;19:282-284.
13. Martins JB, Zipes DP. Epicardial phenol interrupts refractory
period responses to sympathetic but not vagal stimulation in canine
left ventricular epicardium and endocardium. Circ Res. 1980;47:
33-40.
14. Takahashi N, Barber MJ, Zipes DP. Efferent vagal innervation of
canine ventricle. Am J Physiol. 1985;248:H89-H97.
15. Inoue H, Zipes DP. Time course of denervation of efferent sympathetic and vagal nerves after occlusion of the coronary artery in
the canine heart. Circ Res. 1988;62:1111-1120.
16. Miyazaki T, Zipes DP. Presynaptic modulation of efferent sympathetic and vagal neurotransmission in the canine heart by hypoxia,
high K', low pH, and adenosine. Circ Res. 1990;66:289-301.
17. Ehsani A, Ewy GA, Sobel BE. Effects of electrical countershock
on serum creatinine phosphokinase (CPK) isoenzyme activity. Am
J Cardiol. 1976;37:12-18.
18. Pugh BR, Buja LM, Parkey RW, Poliner LR, Stokely EM, Bonte
FJ, Willerson JT. Cardioversion and 'false positive' technetium-99m stannous pyrophosphate myocardial scintigrams. Circulation. 1976;54:399-403.
19. DiCola VC, Freedman GS, Downing SE, Zaret BL. Myocardial
uptake of technetium-99m stannous pyrophosphate following
direct current transthoracic countershock. Circulation. 1976;54:
980-986.
20. Knox MA, Hughes HC, Tyers GFO, Seidl D, Demes LM. The
induction of myocardial damage by open-chest low-energy countershock. Med Instru. 1980;14:63-66.
21. Kerber RE, Martins JB, Gascho JA, Marcus ML, Grayzel J. Effect
of direct-current countershocks on regional myocardial contractility and perfusion. Circulation. 1981;63:323-332.
22. Doherty PW, McLaughlin PR, Billingham M, Kernoff R, Goris
ML, Harrison DC. Cardiac damage produced by direct current
countershock applied to the heart. Am J Cardiol. 1979;43:
225-232.
23. Cobb FR, Wallace AG, Wagner GS. Cardiac inotropic and
coronary vascular responses to countershock. Circ Res. 1968;23:
731-742.
24. Fain ES, Billingham M, Winkle RA. Internal cardiac defibrillation:
histopathology and temporal stability of defibrillation energy
requirements. JAm Coil Cardiol. 1987;9:631-638.
25. Gaba DM, Waxwell MS, Merlone S, Smith C. Internal countershock produces myocardial damage and lactate production
without myocardial ischemia in anesthetized dogs. Anesthesiology.
1987;66:477-482.
26. Arnsdorf MF, Rothbaum DA, Childers RW. Effect of direct
current countershock on atrial and ventricular electrophysiological
properties and myocardial potassium efflux in the thoracotomised
dogs. Cardiovasc Res. 1977;11:324-333.
27. Koning G, Veefkind AH, Schneider H. Cardiac damage caused by
direct application of defibrillator shocks to isolated Langendorffperfused rabbit heart. Am Heart J. 1980;100:473-482.
28. Anderson GJ, Reiser J. Electrophysiologic changes induced by
external transthoracic countershock. J Electrocardiol. 1983;16:
191-198.
29. Niebauer MJ, Geddes LA, Babbs CF. Potassium efflux from myocardial cells induced by defibrillator shock. Med Instru. 1986;20:
135-137.
30. Lucy SD, Jones DL, Klein GJ. Effects of defibrillation shocks
delivered directly over a major coronary artery. PACE Pacing Clin
Electrophysiol. 1992;15(part I):1711-1719.
31. Koning G, Schneider H, Reneman RS, Hoelen AJ. An electrode
system with rounded edges for direct ventricular defibrillation. Med
Biol Eng. 1972;10:201-206.
32. Kim Y, Fahy B, Tupper BJ. Optimal electrode designs for electrosurgery, defibrillation, and external cardiac pacing. IEEE Trans
Biomed Eng. 1986;33:845-853.
33. Yabe S, Smith WM, Daubert JP, Wolf PD, Rollins DL, Ideker RE.
Conduction disturbance caused by high current density electric
fields. Circ Res. 1990;66:1190-1203.
34. Rubin L, Hudson P. Epicardial versus parietal pericardial defibrillation. Am J Emerg Med. 1985;3:160-164.
35. Winkle RA, Stinson EB, Echt DS, Mead RH, Schmidt P. Practical
aspects of automatic cardioverter/defibrillator implantation. Am
Heart J. 1984;108:1335-1346.
36. Bach SM, Shapland JE. Engineering aspects of implantable
defibrillators. In: Saksena S, Goldshlager N, eds. Electrical Therapy
for CardiacArrhythmias. Philadelphia, Pa: WB Saunders Co; 1990:
371-383.
37. McLean LD, van Tyn RA. Ventricular defibrillation. JAMA. 1961;
175:471-474.
38. Dixon EG, Tang ASL, Wolf PD, Meador JT, Fine MJ, Calfee RV,
Ideker RE. Improved defibrillation thresholds with large contoured epicardial electrodes and biphasic waveforms. Circulation.
1987;76:1176-1184.
39. Ideker RE, Wolf PD, Alferness C, Krassowska W, Smith WM.
Current concepts for selecting the location, size and shape of defibrillation electrodes. PACE Pacing Chn ElectrophysioL 1991;14:227-240.
Ito et al DC Shocks and Autonomic Neural Function
40. Alt E, Theres H, Heinz M, Albrecht K, Georg H, Bloemer H. A
new approach towards defibrillation electrodes: highly conductive
isotropic carbon fibers. PACE Pacing Clin Electrophysiol. 1991;14:
1923-1928.
41. Rivkin LM. The defibrillator and cardiac burns. J Thoracic Car,
diovasc Surg. 1963;46:755-764.
42. Peleska B. Cardiac arrhythmias following condenser discharges
and their dependence upon strength of current and phase of
cardiac cycle. Circ Res. 1963;13:21-32.
43. Peleska B. Cardiac arrhythmias following condenser discharges led
through an inductance: comparison with effects of pure condenser
discharges. Circ Res. 1965;16:11-18.
44. Stoeckle H, Nellis SH, Schuder JC. Incidence of arrhythmias in the
dog following transthoracic ventricular defibrillation with unidirectional rectangular stimuli. Circ Res. 1968;23:343-348.
45. Anderson HN, Reichenbach D, Steinmets GP Jr, Merendino KA. An
evaluation and comparison of effects of alternating and direct current
electrical discharges on canine hearts. Ann Surg. 1964;160:251-262.
46. Lumb G, Anderson GJ, Kase ML, Woo DV. Damage in canine
hearts following defibrillator shocks. Ann Clin Lab Sci. 1986;16:
171-179.
2673
47. Jones JL, Jones RE. Decreased defibrillator-induced dysfunction
with biphasic rectangular wave forms. Am J Physiol. 1984;247:
H792-H796.
48. Inoue H, Zipes DP. Result of sympathetic denervation in the
canine heart: supersensitivity that may be arrhythmogenic. Circulation. 1987;75:877-887.
49. Furman S, Kim SG. The present status of implantable cardiovascular defibrillation therapy. J Cardiovasc Electrophysiol. 1992;3:
602-625.
50. McVeigh K, Mower MM, Nisam S, Voshage L. Clinical efficiency
of low energy cardioversion in automatic implantable cardioverter
defibrillator patients. PACE Pacing Clin Electrophysiol. 1991;14:
1846-1849.
51. Winkle RA, Bach SMJ, Mead RH, Gaudiani VA, Stinson EB, Fain
ES, Schmidt P. Comparison of defibrillation efficiency in humans
using a new catheter and superior vena cava spring-left ventricular
patch electrodes. JAm Coil Cardiol. 1988;11:365-370.
52. Singer I, Lang D. Defibrillation threshold: clinical utility and therapeutic implications. PACE Pacing Clin Electrophysiol. 1992;15:
932-949.
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
Defibrillating shocks delivered to the heart impair efferent sympathetic responsiveness.
M Ito, H P Pride and D P Zipes
Circulation. 1993;88:2661-2673
doi: 10.1161/01.CIR.88.6.2661
Downloaded from http://circ.ahajournals.org/ by guest on April 30, 2017
Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231
Copyright © 1993 American Heart Association, Inc. All rights reserved.
Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on the
World Wide Web at:
http://circ.ahajournals.org/content/88/6/2661
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in
Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.
Once the online version of the published article for which permission is being requested is located, click Request
Permissions in the middle column of the Web page under Services. Further information about this process is
available in the Permissions and Rights Question and Answer document.
Reprints: Information about reprints can be found online at:
http://www.lww.com/reprints
Subscriptions: Information about subscribing to Circulation is online at:
http://circ.ahajournals.org//subscriptions/