Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
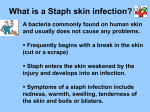
Staphylococcal and streptococcal infections Staphylococcal infections More than 30 staphylococcal species exist All are part of normal skin and mucous membrane flora They are either coagulase-positive or negative The most important coagulase-positive species is Staph. aureus Staph aureus 30% adults carry Staph. aureus in their anterior nares Carriers transfer the organism to skin allowing a portal of entry The organism has several putative determinant of pathogenicity including: Cell wall constituents Cell surface proteins Toxins (e.g. haemolysins and leukocidins) Enzymes (e.g. coagulase, protease, hyaluronidase) The organism is both aerobic and anaerobic on blood agar Microscopically it is gram-positive Forms clusters on solid media There is increasing spread of clones resistant to beta-lactam antibiotics (e.g. MRSA) Clinically it produces skin and soft tissue infections including Impetigo Folliculitis Cellulitis Deeper infections may occur after trauma or surgery Metastatic infection may result in Endocarditis Pericarditis Osteomyelitis Lung abscesses Treatment is with antistaphylococcal antibiotics (e.g. flucloxacillin) In MRSA Vancomycin is the treatment of choice Coagulase-negative staphylococci Staph. epidermidis and Staph. saprophyticus are the commonest human pathogens Staph. epidermidis is a common cause of nosocomial bacteraemia Often associated with indwelling catheters and prosthetic materials Is a common cause of prosthetic valve endocarditis Its is often multiply antibiotic resistant Treatment may require removal of line or prosthesis Streptococcal infections Streptococci are gram-positive cocci More than 30 species have been identified On solid media they grow in pairs or chains They are catalase negative Beta-haemolytic streptococci are classified according to their Lancefield group The following are human pathogens Strep. pyogenes (group A Streptococcus) Group C and G streptococci Strep. pneumoniae (pneumococcus) Group B Streptococcus viridans group streptococci Enterococcus Strep. pyogenes Important human pathogen Causes various cutaneous and systemic infections including Streptococcal pharyngitis Scarlet fever Rheumatic fever Post-streptococcal glomerulonephritis The bacteria is sensitive to penicillin Strep. pneumoniae Common bacterial pathogen Found in the nasopharynx of 20% of adults On a Gram-stain it appears as a diplococcus It is alpha-haemolytic on blood agar Common cause of localised and systemic infections including Otitis media Sinusitis Meningitis Pneumonia Endocarditis Osteomyelitis Infection can be prevented by the pneumococcal vaccine Resistance to penicillin is increasing worldwide Viridans group streptococci The viridans group of streptococci are a diverse group of organisms They are respiratory, gastrointestinal and oral cavity commensals Infection usually occurs in immunocompromised hosts Principal virulence trait is to adhere to cardiac valves and cause endocarditis Account for 30 - 40% of cases of endocarditis Most occur in patients with valvular heart disease Other risk factors include: Prosthetic heart valves Intravenous drug abuse Most are viridans streptococcal species are sensitive to penicillin Enterococcus spp. Enterococci are facultative anaerobes They are common commensal of the gastrointestinal tract They are significant cause of nosocomial infection including Urinary tract infections Endocarditis Intra-abdominal infection Risk factors for infection include Severe underlying disease Previous surgery Previous antibiotic therapy Renal failure The presence of vascular or urinary catheters Mortality from enterococcal infection is high Intrinsically resistant to beta-lactams and aminoglycosides They can also acquire resistance to Vancomycin Management of Vancomycin-resistant enterococcus (VRE) is difficult Bibliography Herwaldt L A. Staphylococcus aureus nasal carriage and surgical site infections. Surgery 2003; 134 (Suppl 5): S2-S9. Lowy F D. Staphylococcus aureus infections. N Engl J Med 1998; 339: 520-552.