Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Polysubstance dependence wikipedia , lookup
Plateau principle wikipedia , lookup
Orphan drug wikipedia , lookup
Compounding wikipedia , lookup
Psychopharmacology wikipedia , lookup
Theralizumab wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmacognosy wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Drug discovery wikipedia , lookup
Neuropsychopharmacology wikipedia , lookup
Prescription costs wikipedia , lookup
Drug design wikipedia , lookup
Neuropharmacology wikipedia , lookup
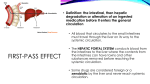
ION TRAPPING and absorption of drugs • Ion trapping example • Aspirin is an acidic drug. When aspirin is in the acidic environment of the stomach (pH 23), it exists predominantly in the nonionized/lipophilic form. Aspirin will easily enter the cells of the stomach. The inside of these cells have a pH of 7.4. Most of the drug molecules will shift to the ionized/hydrophilic form in this pH, which will “trap” those molecules inside the cells. • There will always be some nonionized/lipophilic molecules inside the stomach cells. As a nonionized/lipophilic molecule leaves the stomach cell and enters the circulatory system, an ionized/hydrophilic molecule is converted to the nonionized/lipophilic form to preserve the ratio. This action continues until all aspirin molecules have exited the stomach cells and entered the circulation. Effect of dissolution and GI motility on absorption of orally administered drugs • Oral medication must be in the lipophilic form to be absorbed into the cells of the GI tract. The medication must also be small enough to enter the cells. • ___________________ is the dissolving of a drug. • _____________ medications (solutions, elixirs) do not have to go through a dissolution process. • _____________ medications (tablets, granules, powders) must go through dissolution and be broken apart to be absorbed. • Because liquids do not have to go through dissolution, they are usually absorbed more rapidly than solid forms of medication and may have a quicker onset of action. Effect of dissolution and gi motility on absorption of orally administered drugs • _________________________ tablets dissolve slowly over minutes to hours, releasing small amounts of medication for absorption and sustaining a consistent level of medication in the blood. • Because the medication is released slowly, there will be a __________ peak in blood concentration of the medication than if it were given in a regular-release form. • The higher the peak in blood concentration, larger the concentration gradient between the blood and tissues. • The larger the concentration gradient, the quicker the diffusion will happen into the tissues. Effect of dissolution and gi motility on absorption of orally administered drugs • Most absorption for PO drugs occurs in the _________________, so dissolution needs to occur __________ the meds get there. • Alteration of the GI tract’s motility can effect how much time a medication has to dissolve and be absorbed. • Spasming of the pylorus will also cause gastric emptying to be delayed. • Increased gastric motility may cause drugs to get to the intestines and be absorbed sooner than desired. • Diarrhea (increased intestinal motility) may move the medication past the small intestines before it is dissolved. • Decreased intestinal motility can cause more of the drug to be absorbed than was intended. First-pass effect • Definition: the _____________, then _____________ degradation or alteration of an ingested medication before it enters the general circulation • All blood that circulates to the small intestines must travel through the liver on its way to the systemic circulation. • The HEPATIC PORTAL SYSTEM conducts blood from the intestines to the liver where the contents from the intestines can have toxins and other substances removed before reaching the systemic circulation. • Some drugs are considered foreign by the liver and never reach systemic circulation. Effect of perfusion on absorption of parenterally administered drugs • PERFUSION: • Tissues that are ______________ with blood absorb injected drugs much ___________ than tissues that are poorly perfused. • Injecting a drug in an area that is far away from the blood stream, or an area that has very few vessels will slow absorption as the drug will have to diffuse over a long distance. • Muscle is well perfused compared to fat so IM medications should be absorbed faster than SQ. • An inactive muscle is less perfused than an active muscle. • Cold temps cause vasoconstriction in SQ capillaries, decreasing the rate of absorption. Warm temps have the opposite effect. • DISTRIBUTION: the movement of a drug from the systemic circulation into tissues • Drugs enter and exit the circulation at the capillaries • Capillaries have ________________ that allow fluid and molecules to enter and exit the circulation. • Both hydrophilic and lipophilic molecules can fit through fenestrations. • In the brain, capillary anatomy is different. ________ _______________________________________________ _______________________________________________ The only type of drugs that can pass through the BBB are lipophilic molecules who pass through the cell membranes. • Other areas of the body that have similar capillary anatomy are the globe of the eye and the prostate. Barriers to drug distribution • Capillaries of the placenta have fenestrations, so one should assume that drugs administered to a pregnant female may have an effect on the fetus. Effect of tissue perfusion on drug distribution • Drugs are distributed faster and in larger amounts to tissues that are well-perfused (active skeletal muscle, liver, kidneys). • Drug delivery is delayed to poorly perfused areas of the body such as fat and inactive skeletal muscle. • _____________________ occurs after the drug molecules have been distributed to the tissues. Drug molecules move back and forth between the blood and tissues due to diffusion and the presence of a concentration gradient. • Redistribution continues until there is equilibrium between the blood and tissues. • Plasma is filled with proteins that are too large to leave the circulation. • Many drugs are made so that a percentage of their molecules bind to proteins. ____________________________________________ ______________________________________________________ ______________________________________________________ • Only the “________________” of the drug is small enough to leave the capillaries and have an effect on the tissues. • There is a balance between the bound drug molecules and free drug molecules. When a free molecule leaves circulation, a protein releases its bound molecule to replace the one that left. • Drugs that are highly protein-bound must be used with caution in animals with _______________________ (GI, liver, renal issues) as more drug will be active in those animals than in healthy ones. Drug dose should be lowered. Effect of plasma protein binding on drug distribution Volume of distribution • Vd: a value that indicates the extent to which a drug is distributed throughout the body. • It assumes that the drug is equally distributed throughout each compartment of the body and that the concentration on the blood is in equilibrium with the concentration in the rest of the body. • _________________________________________________________________________________ _________________________________________________________________________________ • Drug is diluted by the fluid of the body compartments • Vd are different between animals of the same size but different percentages of body fat. • Animals with large amounts of fat will have higher blood levels than lean animals as it will take longer for the drug to distribute to the fat than it will to distribute to the active skeletal muscle of the lean animal. • Drug dose will need to be adjusted. • Actual Vd is not known. Apparent Vd is an estimate. • Apparent Vd can be determined by knowing the dose of administered drug and the blood concentration of the drug. • Even if a drug is distributed throughout the body, it won’t have an effect on all the tissues that it is distributed to. • In order for a drug molecule to have an effect on a cell, the cell must have a receptor on its membrane that is a fit for the drug. •The drug molecule and receptor fit together like a lock and key. Once the connection is made, the cell is altered in some way. •Every cell does not have a receptor to fit every drug molecule. •Drug molecule A that is specific for making uterine muscles contract will not make muscles of the stomach contract. The stomach muscles will lack receptors for drug molecule A. •A cell will be very sensitive to the effects of a drug if it possesses a large number of receptors that the drug can bind to. •Cells can increase or decrease there number of receptors. •Cells have many different receptors that produce many different effects. Pharmacodynamics: the way drugs exert their effects • Neurotransmitters and hormones have receptors on the surface of cells. When they bind with the receptor, they stimulate that receptor to produce or to inhibit a specific action in the cell. Drugs are made to bind with these same receptors. • Some drugs act as _______________, stimulating the receptor in the same way that the body’s neurotransmitters and hormones do. Other drugs act as _______________, blocking the action of the natural substance on the receptor. • When a drug molecule combines with a receptor, it has a specific effect on a cell. The specific effect is the drug’s ______________________. Antagonists and agonists Antagonists and agonists • Drugs can antagonize each other. • ______________________ ANTAGONISM exists when two different drugs fit in the same receptor site and their intrinsic activities are opposite of one another. The effect that is seen depends on which drug is present in greater quantities. This exists with drugs that reverse one another. • _________________________ ANTAGONISM exists when one drug either combines better with the shared receptor or one drug alters the shape of the other drug’s receptor. The latter would prevent the noncompetitive antagonist from binding. Antagonists and agonists • If Drug X increases the heart rate by 50% and Drug Y also increases the heart rate, but only by 25%, Drug Y is a PARTIAL AGONIST to Drug X. These drugs attach to the same receptor, but cause different levels of intrinsic activity. • If Drug X increases the heart rate by 50% and Drug Z decreases the heart rate by 25%, Drug Z is a PARTIAL ANTAGONIST to Drug X. It is not a reversal agent, but can reduce the effects of another drug. Non-receptor-mediated reactions • Some drugs produce their effects without binding to a receptor. • Example 1: The drug Mannitol has the effect of being a diuretic. The molecules of Mannitol are excreted into the urine where they cause additional water to be excreted in the urine via osmosis. • Example 2: Chelators combine with ions or other compounds to produce their effects. EDTA is anticoagulant chelator found in purple top blood tubes. It combines with calcium in the blood sample to prevent clotting. • Example 3: Some antacid medications work by binding to HCl in the stomach to weaken the acid and reduce stomach irritation. Biotransformation and metabolism • BIOTRANSFORMATION: Drugs being metabolized by enzymes into a form that can be eliminated by the body. • Altered drug is known as a METABOLITE. It is usually hydrophilic and eliminated by the kidneys or liver. • THE MAJORITY OF BIOTRANSFORMATION OCCURS IN THE ___________ by cytochrome P450 enzymes (aka the mixed function oxidase system). • Phase 1 of Biotransformation: • Original drug molecule is chemically transformed by adding or removing electrons or by hydrolysis. • The metabolite is now more water soluble. • Phase 2 of Biotransformation: • The metabolite is conjugated, or joined with another molecule to make it more hydrophilic and able to be excreted in the urine. Drug Interactions Affecting Biotransformation • Multiple drugs in the body at the same time can effect each other’s biotransformation. • They may compete for the same enzymes, slowing the metabolism of each. • Toxic concentrations of one drug may result. • The number of enzymes in this system can increase with repeated exposure to the drug. These drugs end up being metabolized at an increased rate. This is referred to as ________ ________________. • Shortens the amount of time that the drug can be effective in the body (also known as ______________). • Explains tolerance that is seen with alcohol consumption. Species and age differences in drug biotransformation • Just because a drug is safe to use in one species, does not mean it is safe to use in all species. • The liver needs time after birth to finish developing (approx. ____ _________). • Since the liver is a major route of biotransformation, caution should be used when administering any drug to neonates that requires the liver to metabolize it. • Older animals may have a decline in liver and/or kidney function. Dosages should be adjusted or alternative medications used if these organs biotransform the medications. Drug elimination • ELIMINATION: also known as excretion, the movement of drug molecules out of the body • Routes of elimination: feces, urine, sweat, exhalation, milk, saliva, keratin • *Major routes of elimination are into the urine (__________), and the feces (bile from the ______________). • Drugs eliminated via the milk should not be used in nursing animals or lactating dairy cows • Changes in elimination can occur with dehydration, degeneration of kidneys or liver with age, or diseases that affect those organs. • Dosages must be adjusted to avoid toxicity • Two ways that drugs are eliminated via the kidney: filtration at the glomerulus and active secretion in the tubules Renal elimination (FILTRATION) • Filtration occurs as blood flows through the glomerulus into Bowman’s Capsule. • Proteins are too large to be filtered. Drugs that are protein bound will remain in the bloodstream at this point. • In cases of hypoproteinemia, drugs that should be protein-bound can be lost in the urine. • Decreased renal blood flow will cause lower numbers of drug molecules to be filtered at the glomerulus. • This would happen with hypotension, dehydration, blood loss, shock, or fight/flight response. • Increased renal blood flow will cause drug molecules to be removed from the body more rapidly. • This would happen with administration of IV fluids, drugs that increase renal perfusion, or hypertension. • Two ways that drugs are eliminated via the kidney: filtration at the glomerulus and secretion into the tubules. • Secretion occurs as early as the proximal convoluted tubule. It involves drug molecules being actively transported from the peritubular capillaries into the urine. No concentration gradient is necessary. Renal elimination • If a protein-bound drug detaches from its protein (in the blood) and (SECRETION) binds to a transport molecule on the cell membrane of the tubule, the drug can be transported into the urine to be excreted. • If the drug is lipophilic, it can be reabsorbed back into the bloodstream as it travels to the Loop of Henle. • After the Loop of Henle, drug concentrations in the urine seldom change. • Blood from the GI tract flows through the liver before entering the systemic circulation. • Drugs excreted by the liver diffuse into hepatocytes and then enter the bile. • Bile is collected in the gallbladder and then dumped into the duodenum. • _______________ drug molecules have the opportunity to be reabsorbed in the small intestines and make a second trip to the liver and repeat the cycle. This is known as ENTEROHEPATIC CIRCULATION. These drugs can effect the body for a longer duration of time than those that don‘t reenter the circulation. • Like the kidneys, drug dosages must be reduced when giving drugs eliminated via billiary excretion to patients with liver insufficiency. Hepatic elimination Half-life and clearance • HALF-LIFE OF ELIMINATION/CLEARANCE: the rate at which drugs leave the body. • Measure of how fast a volume of blood is cleared of the drug, expressed as a volume of blood cleared over time • Time value that describes how long the drug concentration takes to decrease by ______% • May dictate how frequently the drug must be given to maintain concentrations in therapeutic range • May reflect how well the organs that eliminate the drug are functioning • Half life will increase if the organ that eliminates a drug is compromised Relation of Half-life to Steady-state concentrations • STEADY-STATE: point at which drug levels plateau and all peak concentrations are the same and all trough concentrations are the same • Happens when a drug is given repeatedly • The amount of drug being administered equals the amount of drug being eliminated • After the time of one half life has passed, the peak and trough concentrations are approx. 50% of what they will be when they achieve steady-state • The time from beginning of therapy to steady state is approximately ___ times the half life • Example: a drug with a half life of 6 hours will take 30 hours to reach steady state Drug withdrawal times • WITHDRAWAL TIME: the time (in days) after a drug is administered during which the animal cannot be sent to slaughter and the eggs/milk must be discarded • Drug residues in food are a growing concern for people • All drugs approved for use in food animals have a withdrawal time • Drug must not only be out of the bloodstream, but also all of the tissues (no residues) • Waiting period can result in loss of money to the food animal producer, but there are severe fines/penalties for not following withdrawal times. • The FARAD (Food Animal Residue Avoidance Databank) produces a compendium of drugs with their withdrawal times.