Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
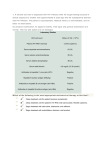
HUMAN IMMUNODEFICIENCY VIRUS (HIV) Introduction Acquired immune deficiency syndrome (AIDS) is a severe, life-threatening disease that represents the late clinical stage of infection with human immunodeficiency virus (HIV). Human immunodeficiency virus (HIV) medicine is a very specialized field and expert advice should ways be sought regarding the management of HIV/ AIDS patients. These guidelines describe general principles only. The Origin of HIV Clinically apparent human immunodeficiency virus (HIV) infection first was recognized in 1981 in homosexual men in New York City who presented with evidence of a profound acquired immune deficiency syndrome (AIDS). For many years scientists theorized as to the origins of HIV and how it appeared in the human population, most believing that HIV originated in other primates. Then in 1999, an international team of researchers reported that they had discovered the origins of HIV-1, the predominant strain of HIV in the developed world. A subspecies of chimpanzees native to west equatorial Africa had been identified as the original source of the virus. The researchers believe that HIV-1 was introduced into the human population when hunters became exposed to infected blood. 3 Epidemiology ● Occurrence is worldwide. There were 40 million people living with HIV/AIDS by the end of 2001 and in 2000 three million people died from HIV-related illnesses. The vast majority of HIV infections occur in developing countries. ● For the period 1983 to 2003 there was a cumulative total of 4680 HIV diagnoses in Victoria. This represents about 21% of Australia’s total. Males accounted for 94% of the diagnoses. Pathophysiology Organism ● Human immunodeficiency virus (HIV) types 1 and 2 are a member of family retroviridae. Immunopathology HIV results in chronic infection of immune cells that express the antigen CD4+, to which the virus attaches and gains entry to the cell. A DNA copy of the viral RNA genome is then produced by the viral enzyme reverse transcriptase, (retroviruses are distinguished by this ability). This DNA “pro-virus” then integrates into the host’s DNA where it codes for continuing viral production. Ongoing replication of the virus eventually leads to the death of the cell. Cells expressing the CD4+ antigen include: ● Monocytes/ macrophages ● Helper lymphocytes. Infection of the helper lymphocytes leads to a relentless depletion of these cells, which play a major role in the body’s cell mediated immunity. Immune dysfunction is typically not clinically apparent some years following initial infection because CD4+ lymphocytes are usually present initially in numbers that greatly exceed requirements. As numbers of these cells reduce with time to critical levels, malignancies and opportunistic infections begin to occur. Transmission HIV can be transmitted from an infected person by: 1. Sexual exposure: ● 2. Sexual exposure to infected semen, vaginal fluids and other infected body fluids during unprotected sexual intercourse with an infected person. This includes oral sex. Inoculation from biological tissues, icluding: ● Inoculation with infected blood transfusions. ● Blood products transfusions. ● Transplantation of infected organs such as bone grafts or other tissues, ● Artificial insemination with infected semen. 3. 4. Vertical: ● Mother to fetus via placental transfer ● Interventions that decrease the risk of vertical transmission from an infected woman to her child include antiretroviral therapy during pregnancy and caesarean section. With these interventions the risk of mother to child transmission is less than 5%. If there is no intervention, the risk of mother to child HIV transmission has been estimated to be 20– 45%. Breastfeeding: ● 5. Breastfeeding of an uninfected infant by an HIV positive mother. Sharps injuries: ● Sharps injuries including needle stick injuries or other exposure to blood and body fluids. ● The overall rate of seroconversion following a needle stick injury involving HIV infected blood is said to be less than 0.5%, however this is dependent on the type of needle stick injury (deep versus shallow) and the viral load of the infected person. Incubation Period ● The period from infection to the primary seroconversion illness is three to eight weeks. ● The period from infection to development of anti-HIV antibodies is three weeks to three months. ● The interval from HIV infection to the diagnosis of AIDS ranges from about nine months to 20 years or longer, with a median of 12 years. ● There is a group of people with a more rapid onset of disease who develop AIDS within three to five years of infection. ● Treatment with antiretroviral drugs and disease specific prophylaxis has resulted in an 80% reduction in AIDS-associated illnesses. Reservoir ● Humans. Period of Communicability ● All antibody positive persons carry the HIV virus. ● Infectivity is presumed to be life long. ● Successful therapy with antiretroviral drugs can lower the viral load in blood and semen to undetectable levels and reduce infectivity. Susceptibility and Resistance ● Everyone is susceptible to infection. ● The presence of other sexually transmitted infections, especially those with skin or mucosal ulceration, may increase susceptibility. Clinical Features The 1993 CDC Classification for HIV/ AIDS: CLINICAL CATEGORY CD4 Cell Count A B C ≥ 500/ mm 3 A1 B1 C1 200-499/ mm 3 A2 B2 C2 < 200/ mm 3 A3 B3 C3 Patients who have clinical category C conditions or who have a CD4 count that is less than 200 are classified as having AIDS. See appendix 1 below for a table that demonstrates the relationship of the CD4 count to the development of clinical disease. Therefore AIDS patients will be classified as C1, 2, 3 or A3, and B3. Clinical Category A This group includes: 1. Acute primary (seroconversion) HIV illness 2. Asymptomatic (latent) HIV infection. 3. Persistent generalized lymphadenopathy. Acute primary (seroconversion) HIV illness 1. 2. Acute seroconversion: ● This generally occurs within 2-4 weeks of primary contact with the HIV virus. ● Many cases will be very mild or asymptomatic. ● The illness itself is non-specific with constitutional symptoms which may include, fever, myalgias, arthralgias, anorexia, malaise and lethargy. Lymphadenopathy and mild splenomegaly may occur. A non-specific rash may also occur. It is often described as an infectious mononucleosis type illness. ● The illness may last 2-3 weeks. Occasionally a neurological syndrome may present: 4 ● Meningo-encephalitis. ● Neuropathies. ● Guillain Barre syndrome. Asymptomatic (latent) HIV infection. ● Infected persons may then be free of clinical signs or symptoms for months to 10 years or sometimes even longer than this. ● During this period there is usually a progressive decline in the CD4 count. Persistent generalized lymphadenopathy. ● Some patients who are otherwise asymptomatic may develop persistent generalized lymphadenopathy (PGL). ● Some definitions have described PGL as two or more nodes of greater than one centimetre persisting for greater than 3 months. Clinical Category B These patients have symptoms but they are not those which would be classified as group A or group C clinical disease. The predominant clinical features in this group include: 1. 2. Persistent non-specific constitutional symptoms: ● Lasting for greater than one month. ● Fever (>38 5 ) ● Diarrhoea ● Weight loss, (> 10% body weight). A range of muco-cutaneous conditions, including: ● Oropharyngeal candidiasis, (excluding esophageal involvement) ● Oral leukoplakia ● Vulvovaginal candidiasis (persistent, recurrent or refractory) ● Cervical dysplasia (moderate or severe)/cervical carcinoma in situ ● Vasculitis. ● Herpes zoster (shingles), involving ≥2 episodes or ≥1 dermatome ● Atypically severe and generalized skin disorders of xeroderma, molluscum contagiosum or seborrheic dermatitis 3. Idiopathic thrombocytopenic purpura. 4. Peripheral neuropathies. Clinical Category C There is a large range of AIDS-defining illnesses. These include: Neurological ● Progressive HIV encephalopathy. Infective 1. 2. 3. 4. Bacterial ● Recurrent bacterial pneumonia, (≥2 episodes in 12 months) ● Tuberculosis or other mycobacterium Viral ● Chronic herpes simplex infection ● Cytomegalovirus infection, this causes eye disease in particular Fungal ● Candidiasis of the bronchi, trachea, or lungs ● Esophageal candidiasis. ● Cryptococcus neoformans, which may result in meningitis. Protozoal ● Toxoplasmosis of the brain. ● Pneumocystis carinii pneumonia (PCP), this is one of the most common opportunistic infections in HIV patients. ● Cryptosporidiosis Malignancies 1. Kaposi’s sarcoma 2. Lymphomas. HIV wasting Syndrome Wasting syndrome due to HIV is defined as ● Weight loss >10% of baseline body weight Associated with either: ● Chronic diarrhea (≥2 loose stools per day ≥1 month) ● Chronic weakness ● Documented fever ≥1 month Investigations Diagnostic tests 1. 2. 3. FBE: ● Look for lymphopenia. ● Reduction in the lymphocyte CD4 count Serology: ● Detection of HIV antibody by the ELISA screening test. IgM is produced as well as IgG however IgG is more reliable in the screening for HIV and this is the one that is used. Neither the IgG nor IgM are protective. ● IgG in most cases becomes detectable within 3 months. ● If IgG is detected the result is usually then confirmed by Western blot analysis which involves the detection of antibodies direction toward specific HIV viral antigens. The most commonly detected antibody being that which is directed against the p24 antigen. Viral antigen: ● Detection of the viral p24 antigen in serum is done by an EIA (enzyme immuno-assay) test. ● The level of viral load provides an indication of the infectivity of the patient. (From Australian Family Physician vol 20 no 6 June 1991) 4. PCR: ● 5. PCR tests can be done to detect pro-viral DNA sequences, but these are not routinely done nor are they routinely necessary. Viral cultures: ● This is only necessary in certain special clinical situations. The above graph shows the natural history of untreated cases of HIV infection. There is a relentless attrition of CD4 cells with a corresponding increase in viral load. Explanation, counselling and consent: ● Note that when testing any patient for HIV it is very important to include a discussion on the risk profile the patient has (by which many could be reassured) and the meaning of what a positive or negative result would mean. ● It is important also to get specific consent for HIV testing. Further tests CXR ● In particular, to look for evidence of infection or malignancy CT Scan ● This will be indicated in patients being investigated for progressive HIV encephalopathy. ● Metastatic disease or other malignancy such as lymphoma. ● The ring enhancing lesion characteristic if toxoplasmosis. Esophagoscopy/ Bronchoscopy ● This may be done to define the extent of an oropharyngeal candidiasis. Esophageal involvement or tracheal or bronchial involvement are AIDS defining conditions. Management Management issues include: ● Acute seroconversion illness. ● Anti-retroviral treatment ● Treatment of specific AIDS illnesses ● HIV and pregnancy ● Post exposure prophylaxis. ● Education ● Counseling and support Acute seroconversion illness: ● In acute HIV infection, treatment is appropriate on theoretical grounds but is of unproven clinical benefit based on current published evidence. ● The decision to treat at this stage will be made by a specialist in HIV medicine. 2 Anti-retroviral treatment: The following is provided for general information only. Antiretroviral therapy continues to evolve. It should only be prescribed by specialists in HIV medicine. Initiation of treatment will depend on a wide range of factors including: ● The presence or absence of symptoms ● The CD4 count ● The viral load ● Patient profile factors/ co-morbidities. The recommendations for initiation of antiretroviral therapy are summarised in the table below from the Therapeutic guidelines 2006. In general the following principles apply: ● Symptomatic HIV infection (including HIV-associated opportunistic infections, malignancies, central nervous system disease, thrombocytopenia) - all patients should be treated. ● Asymptomatic HIV infection - all patients with a CD4 cell count less than 200 per microlitre should be treated. ● Treatment is usually deferred if the CD4 cell count is greater than 350 per microlitre. ● Patients with a CD4 cell count between 200 and 350 per microlitre should also be treated, although the exact time to initiate antiretroviral therapy in the latter group will be influenced by factors such as short-term risk of disease progression, tolerability and long-term toxicity of the antiretroviral regimen, and the patient’s willingness to maintain a high level of adherence to lifelong therapy. Clinical condition CD4 cell count HIV viral load Recommendation Symptomatic Any value Any value Treat Asymptomatic <200/microlitre Any value Treat Asymptomatic >200/microlitre but Any value Offer therapy ≤350/microlitre Asymptomatic >350/microlitre ≥100 000 copies/mL Discuss with patient, may defer therapy Asymptomatic >350/microlitre <100 000 copies/mL Defer therapy NB: Although antiretroviral drugs are available on the Pharmaceutical Benefits Scheme for patients with CD4 cell counts <500/microlitre, or viral load >10 000 copies/mL, guidelines generally recommend waiting until CD4 cell counts are <350/microlitre. Treatment of specific AIDS illnesses: ● Again this is a very specialized area and patients should be referred to their specialist in HIV medicine. ● A good overview of the prophylaxis and treatment of opportunistic infections in HIV-infected adults is given in the latest edition of the Antibiotic Therapeutic guidelines. HIV infection in pregnancy: 2 ● Antepartum and intrapartum combination antiretroviral treatment of an HIV-infected mother and postpartum treatment of the infant reduces the risk of HIV transmission to the infant to less than 2%. ● This is a highly specialised area and management involving close collaboration between an HIV specialist, an obstetrician and a paediatrician is essential. General principles include: ● The Royal Australian and New Zealand College of Obstetricians and Gynaecologists recommends that all pregnant women should be offered HIV counselling and testing at the first antenatal visit. ● The decision to initiate antiretroviral therapy in an HIV-infected woman should be based on a detailed discussion between the woman and her treating doctors about the pros, cons and uncertainties of treatment. ● All HIV-infected pregnant women should be offered antiretroviral therapy regardless of CD4 cell count and HIV viral load. ● Breastfeeding should be avoided. Post exposure prophylaxis: This is an important area of concern for the public but is especially relevant for health workers. There are specific protocols for staff to follow in these circumstances, (see separate guidelines, Exposure to Blood borne pathogens) In general terms: See the Exposure to Blood Borne Pathogens Package for full details, but in general terms: 1. These cases must be prioritized as category 2. 2. All cases involving a staff member are to be referred to the Infectious Control Nurse Co-coordinator, immediately both in hours and out of hours. 3. First aid: ● 4. 5. Risk assessment: ● There should be an urgent risk assessment done to determine the likeyhood of exposure to HIV. Risk may be doubtful, possible, definite and massive, (see appendix 2 below). ● Identify the source (patient) whenever possible. Testing the source where possible: ● 6. 7. Immediately wash affected area with soap and water - apply Betadine. Do not squeeze the wound. If eyes are contaminated, remove contact lenses and rinse gently with water or normal saline while eyes are open. If blood gets into the mouth, spit it out, then rinse with water several times. 5 Arrange with attending MO to obtain consent for venipuncture from the source (patient) for Hepatitis B surface antigen, Hepatitis C and HIV antibody as soon as possible after the incident. Ensure consent is documented in patients’ history. Infectious Diseases Specialist Advice: ● If the source (patient) is HIV antibody positive the attending MO in emergency should Contact an Infectious Diseases Physician immediately for advice, and referral for further management of the staff member (see attached list). Refer to checklist prior to Infectious Diseases Consultation located in the blood exposure resource folder. ● If there is any uncertainty regarding a case again contact the Infectious Diseases Physician to discuss the case and for advice. Anti-retroviral therapy: ● Consultation with an Infectious Diseases Physician is to be sought before the commencement of any drug regimen. ● As recommended by the US Centres for Disease Control 6 drugs for postexposure prophylaxis after occupational HIV exposure are available in the Emergency Department. ● Combivir, a combination of two antiretroviral agents AZT & 3TC and Nelfinavir (a protease inhibitor). These drugs can reduce the chance of seroconversion by 79%, but the patient must be committed to taking them properly. ● For maximum benefit these drugs should be initiated promptly, preferably within 1 - 2 hours post exposure if possible. 8. ● The drugs should be explained to the patient, but the patient needs to be involved in making the final decision about whether to take them. The recipient needs to make a decision on the day of the exposure and start the antiretroviral drugs as soon as possible. It is best if they take the first dose in the presence of the medical staff and this is documented in the history. ● Antiretrovirals have significant side effects. ID Physicians usually only strongly advise them if the injury is high risk (eg from a known HIV positive source, or during an assault from an unknown source etc). Otherwise the chance of serious side effects may out weigh the benefit of the drugs. In addition the long-term risks of these drugs which we are giving to healthy people is unknown, so they are not prescribed lightly. ● The recipient will usually take 3 drugs, two or three times per day for 4 weeks. ● A patient education handout is available for these drugs. ● Again for full details see the Exposure to Blood Borne Pathogens Package. Follow-up: ● It is essential that all patients are fully aware of their follow-up instructions. ● Staff members are followed up by the Infection Control Nurse and the Northern’s ID physicians. ● Low risk public patients may be followed up by their GP. Information sheets for the GP are available in the Exposure to Blood Borne Pathogens Package Education This is a vital aspect in all cases. Useful information is contained in the Hospital’s blood borne pathogens package. Further Sources of Information The Australasian Society for HIV Medicine: http://www.ashm.org.au Melbourne Sexual Health http://www.mshc.org.au USA Department of Heath and Human Services: http://aidsinfo.nih.gov Appendix 1 Correlation of CD4 counts with clinical illness: 4 Appendix 2 Risk Stratification following possible HIV exposure: 5 Doubtful ● Intradermal injury with needle considered not to be contaminated with blood or body fluid ● Superficial wound not associated with visible bleeding produced by instrument contaminated with blood or body fluid. ● Prior wound or skin lesion contaminated with body fluid other than blood and with no trace of blood ● Mucous membrane surface contact with body fluid other than blood. ● Intact skin visibly contaminated with blood or body fluid Possible (demands appropriate care and follow-up) ● Intradermal injury with a needle contaminated with blood or body fluid ● Wound not associated with visible bleeding produced by an instrument contaminated with blood or body fluid ● Prior wound/skin lesion contaminated with blood or body fluid ● Mucous membrane surface contact with blood Definite (demands appropriate care and follow-up) ● Any direct inoculation such as an intramuscular penetrating injury with a blood or body fluid contaminated needle ● Injection of blood/body fluid ● Laceration that causes bleeding and is produced by an instrument that is visibly contaminated with blood Massive Exposure (demands appropriate care and follow-up) ● Transfusion of blood ● Injection of large volume of blood or body fluids (> 1 ml) ● Parenteral exposure to laboratory specimens containing high titre of virus. References 1. The Bluebook Website. 2. Therapeutic Antibiotic Guidelines 13th ed June 2006 3. CDC Website 4. Could it be HIV? Edited by Graeme Stewart 2nd ed 1994 MJA The Australasian Society for HIV Medicine 5. The Northern Hospital Exposure to Blood Borne Pathogens Package. 6. MMWR 1998; 47(RR-7).