Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
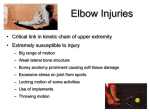
Elbow/ Forearm Anatomy • Bones – – – – Humerus Ulna Radius Bony Alignment • Arthrology and Movements – Humeroulnar Humeroradial – Proximal & Distal Radioulnar Elbow/Forearm Anatomy • Ligaments and Capsule – Joint Capsule – Ulnar Collateral (UCL) • 3 bundles – – – – Lateral Ulnar Collateral (LUCL) Radial Collateral (RCL) Annular Interosseus Membrane Anterior, Transverse, and Posterior Bundles Elbow Movements • Which muscles accomplish these? – Flexion – Extension – Supination – Pronation Elbow/Forearm Anatomy • Musculature – Elbow Flexor/Pronator Group • • • • Biceps brachii Brachialis Brachioradialis Pronator Teres/Quadratus • Forearm Flexors - Common Flexor Tendon » Medial epicondyle – Flexor carpi radialis – Flexor carpi ulnaris – Flexor Digitorum – Palmaris Longus Elbow/Forearm Anatomy • Musculature – Extensor/Supinator Group • • • • Triceps Brachii Anconeus Supinator Extensor carpi radialis longus • Forearm Extensors - Common » Lateral epicondyle – – – – Extensor carpi radialis brevis Extensor carpi ulnaris Extensor digitorum Extensor digiti minimi Extensor Tendon Elbow/Forearm Anatomy • Bursae – Bicipital – Olecranon • Subcutaneous and Subtendinous • Blood supply – Brachial, Radial, and Ulnar arteries • Nerve – Radial, Ulnar, and Median Nerves Elbow Observation • Anatomical – Carrying Angle – Cubitum Varum – Cubitum Valgum – Cubitum Recurvatum Common Mechanisms of Injury Indirect Direct Bursitis – Etiology • Superficial location makes it extremely susceptible to injury (acute or chronic) --direct blow – Signs and Symptoms • Pain, swelling, and point tenderness • Swelling will appear almost spontaneously and w/out usual pain and heat – Management • In acute conditions, compression for at least 1 hour • Chronic cases require superficial therapy primarily involving compression • If swelling fails to resolve, aspiration may be necessary – Tends to fill up again • Can be padded in order to return to competition Elbow Injuries • Bursitis Elbow Injuries • Muscle Strains – Etiology • MOI is excessive resistive motion (FOOSH), repeated microtears • Hyperextension – torn anterior capsule • Rupture of distal biceps is most common muscle rupture of the upper extremity – Signs and Symptoms • Active or resistive motion produces pain; point tenderness in muscle, tendon, or lower part of muscle belly – Management • • • • RICE and sling in severe cases Follow-up w/ cryotherapy, ultrasound and exercise Tape for athletic competition If severe loss of function encountered - should be referred for Xray (rule out avulsion or epiphyseal fx • Forearm Compartment Syndrome – Impaired circulation and neural function Elbow/Forearm Injuries Musculature/Tendinitis • Medial Epicondylitis - chronic “Pitcher’s, Golf, Javelin Elbow” – MOI: repeated flexion (common flexor tendon), valgus stresses, faulty biomechanics – Special Tests: Epicondylitis tests (Flexor/Pronator) • Tx: RICE (emphasize rest), NSAIDs, strengthening Elbow/Forearm Injuries • Lateral Epicondylitis - chronic “Tennis Elbow” – MOI: overuse of extensor/supinator muscles, faulty biomechanics (common extensor tendon) • faulty backhand, too much topspin, too small or large grip – Special Tests: Epicondylitis tests (extensors) – Tx: RICE (emphasize rest), NSAIDs, strengthening, biomechanics correction Elbow Injuries • Bony/Articular – Osteochondrosis/Osteochondritis • Loose bodies (joint mice) – locking and clicking – Little League Elbow (valgus overload or overstress injury to the medial elbow ) • Apophysitis, stress fractures, avulsions usually at medial epicondyle • Onset is slow, very progressive pain – Throwing distance is affected • Tx: RICE (emphasize rest), NSAIDs Nerve Injuries • Ulnar nerve trauma – The “funny bone” – Tinel’s sign • Radial tunnel syndrome – Resembles lateral epicondylitis – Long finger test • Pronator Teres Syndrome – Median Nerve – Pinch test Elbow/Forearm Injuries • Fractures - Humerus, Radius, Ulna • MOI: – Direct contact – FOOSH • Tx: – Immobilize – Referral – Monitor pulse and circulation Elbow Injuries • Dislocations – S/S:deformity, pain, limited ROM, swelling. – Management • Immobilize in position found • Do Not Reduce • Monitor distal pulse and neurological signs Elbow Injuries • Volkmann’s Contracture – result of serious elbow/forearm injury – S/S: 4 P’s 1. 2. 3. 4. loss of pulse pallor paralysis pain w/ passive finger extension Elbow Injuries • Ligament Sprains – Lateral Collateral Ligament (Radial) • Not as common as MCL sprain. • Special tests: – Varus Test – Annular Ligament • Special Test: – Radioulnar test – Lateral ulnar collateral ligament • Posterior instability test – Management • Conservative treatment begins w/ RICE and NSAID’s LUCL What about the ulnar collateral ligament? • The Throwing or Overhead motion Throwing Motion • Early cocking – Abduction/ER - Supraspinatus very active • Late Cocking – Anterior shld. Stretched/medial elbow valgus – Scapula must be stable – Valgus stress on elbow • Acceleration – Stable scapula/Large muscle groups to IR – Valgus stress on elbow • Deceleration - ECCENTRIC – Teres Minor/Infraspinatus espec. active to slow down – Biceps Brachii to slow elbow extension • Follow-Through – Scapula protracts(abducts) - Serratus anterior – LHB tendon stabilizes Tensile stress Acceleration: Extension occurs at a rate of up to 2500º per second and continues to 20º of flexion. Forearm lags behind the upper arm and generates valgus stress (> 60 Nm), The valgus force can overcome the tensile strength of the UCL and cause either chronic microscopic tears or acute rupture. Ulnar (Medial) Collateral • At 90º of flexion, it provides 55% of the resistance to valgus stress at the elbow. – UCL is composed of 3 bands: anterior, posterior, and transverse • Etiology – Injured as the result of a valgus force from repetitive trauma – Can also result in ulnar nerve inflammation, or wrist flexor tendinitis; overuse flexor/pronator strain, ligamentous sprains; elbow flexion contractures or increased instability Ulnar (Medial) Collateral • Signs and Symptoms – – – – Pain along medial aspect of elbow; tenderness over MCL Associated paresthesia, positive Tinel’s sign Limited extension and supinatioin Pain w/ valgus stress test at 20 degrees; possible end-point laxity – X-ray may show marginal osteophytes; calcification w/in MCL; loose bodies in posterior compartment • Management • Conservative treatment begins w/ RICE and NSAID’s OR • Surgical intervention may be necessary (Tommy John procedure) Elbow Injuries • Ruptured Medial Collateral Ligament – “Tommy John” Surgery – Use palmaris longus to replace the ligament – valgus stress avoided for 4-6 months – 1 to 1 ½ years to recover Posterolateral rotatory instability • Tear in Lateral Ulnar Collateral Ligament – Humeroradial joint in instable – Radius and ulna “rock away” from humerus with extension – Special Test: • Posterolateral rotatory instability test • May occur alone or along with ulnar collateral tears Prevention of Elbow Injuries • Protective Equipment – Pads, counterforce braces • Physical Conditioning – Don’t forget the muscles • To support MCL and flexor carpi ulnaris and flexor digitorum superficialis – Fist pumps and Rice bucket • Proper Skill and Technique Elbow Problem Solving Putting it together with Case studies Recognition and Management of Injuries to the Elbow • Subject to injury due to broad range of motion, weak lateral bone structure, and relative exposure to soft tissue damage • Many sports place excessive stress on joint • Locking motion of some activities, use of implements, and involvement in throwing motion make elbow extremely susceptible History – – – – – – – – – What is the cause of pain? Mechanism of injury? Previous history? Location, duration and intensity of pain? Creptitus, numbness, distortion in temperature? Sounds or sensations? Technique changes? Weakness or fatigue? What provides relief? Observation – Deformities and swelling? – Carrying angle • Cubitus valgus versus cubitus varus – Flexion and extension • Cubitus recurvatum – Elbow at 45 degrees • Isosceles triangle (olecranon and epicondyles) – Elbow at 0 degrees • Straight line (olecranon and epicondyles) Palpation - bony • • • • • • Humerus Medial and lateral epicondyles Olecranon process Radial head Radius Ulna Palpation – soft tissue • Ulnar (medial), Radial and Lateral Ulnar collateral ligaments • Annular ligament • Biceps brachii • Brachialis • Brachioradialis • Pronator teres • Triceps • Anconeus • Supinator • Wrist flexors and extensors ROM and Muscle Testing – Active and Passive Range of Motion • Flexion and Extension • Supination and Pronation – Muscle Testing • Muscles of the elbow and those that serve as wrist flexors, extensors, supinators, and pronators Circulatory and Neurological Function – Circulatory • Pulse should be taken at brachial artery and radial artery • Skin sensation should be checked - determine presence of nerve root compression or irritation in cervical or shoulder region – Neurology • • • • Tinel’s sign Elbow Flexion Test Pronator Teres Syndrome Test Pinch Test Joint Stability • • • • Valgus Stress Test Varus Stress Test Radioulnar Joint Test Posterolateral Rotatory Instability Test Epicondylitis Tests • • • • • Resisted Wrist Extension Test Resisted Long Finger Extension Test Wrist Flexion-Pronation Stretch Test Resisted Wrist Flexion Test Wrist Extension-Supination Stretch Test Case Study #1 • A 24 year old woman comes to you complaining of pain in her right elbow on the medial side. The pain sometimes extends into the forearm and is often accompanied by tingling in to the little finger and half of the ring finger. The pain and paresthesia are particularly bothersome when she plays recreational volleyball. Describe your assessment plan. Case Study #2 • A 14 year old female gymnast comes to you complaining of elbow pain. She explains she was doing a vault and bent her elbow backward (hyperextension) when she heard a snap. The injury occurred 1 hour ago and there is swelling. She is cradling her elbow in slight flexion against her body and she does not want to move the elbow. She has normal sensation and vascularity in her hand. Describe your assessment plan. Case Study #3 • A 22 year old wrestler comes to you complaining of posterior elbow pain. He says that 10 days ago he banged his elbow in practice and then later on his car door. He has had posterior swelling since then and increasing pain and dysfunction. Describe your assessment plan. Case Study #4 • A 46 year old man comes to you complaining of diffuse left elbow pain. He notes that when he picks items up with his left hand to carry, the pain increases dramatically. For example, when he carries a briefcase for several minutes, his elbow becomes stiff and sore. He reports general physical activity including gardening and work around the home. He has a workshop and does some woodwork and other crafts. Describe your assessment plan.