Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
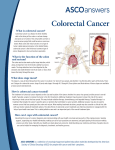
Focus on Colorectal Cancer in Ontario Driving quality, accountability and innovation throughout Ontario’s cancer system TABLE OF CONTENTS Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 Anatomy of the Colon and Rectum . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Risk Factors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 Incidence of Colorectal Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 Mortality from Colorectal Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 Colorectal Cancer Survival . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4 Colorectal Cancer Screening . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5 Assessing Consistency of Practice Against Evidence-Based Recommendations . . . . . . . . . . 7 Practice Guidelines and the Treatment of Colorectal Cancer . . . . . . . . . . . . . . . . . . . . . . . . . 7 Surgical Treatment of Colorectal Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7 Adjuvant Therapy of Early Stage Colorectal Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 Management of Metastatic Colorectal Cancer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9 Observations on the Treatment of Colorectal Cancers at the Regional Cancer Centres . . . . 10 Role of Palliative Care . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 Access to Cancer Treatment – Wait Times . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24 Glossary of Terms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26 Practice Guideline Publications of the Gastrointestinal Disease Site Group . . . . . . . . . . . . . 27 FOCUS ON COLORECTAL CANCER IN ONTARIO Prepared by: Dr. Jean Maroun Chair, Gastrointestinal Disease Site Group Dr. W.K. (Bill) Evans Chief Medical Officer and Provincial Vice-President With the Assistance of: Saira Bahl Dr. Bernard Cummings Mark Gregus Dr. Eric Holowaty Dr. Loraine D. Marrett Dr. Tom McGowan Diane Nishri Sherman Quan Dr. Linda Rabeneck Dr. Marko Simunovic Dr. Andy Smith Dr. Hartley Stern Dr. Terrence Sullivan Beth Theis Dr. Anthony Whitton Dr. Brent Zanke September 2004 FOCUS ON COLORECTAL CANCER IN ONTARIO Introduction Colorectal cancer is the most common form of gastrointestinal cancer and includes cancers of both the colon and the rectum. Colorectal is the fourth most common form of cancer in Canada, after breast, lung and prostate cancer. This monograph on colorectal cancer has been prepared to provide information on patterns of practice to those directly involved in the provision of care to these patients throughout Ontario, as well as to those who are responsible for managing components of the health care system. The practice patterns are shown against the backdrop of the evidence-based guidelines developed by the Gastrointestinal Disease Site Group of Cancer Care Ontario’s Program in Evidence-based Care. In addition to information on patterns of practice, this monograph provides information on the timeliness of access to care, the risk factors associated with colorectal cancer, and an overview of the incidence and mortality of colorectal cancer. In brief, it provides a synoptic assessment of the current quality of care for colorectal cancer patients in the province of Ontario. It is hoped that this monograph will assist those responsible for care delivery to achieve the best possible results for patients with a diagnosis of colorectal cancer. The information in this monograph has been collected from a variety of Cancer Care Ontario (CCO) sources. Data on incidence, mortality, and survival were extracted from data held by the Ontario Cancer Registry (OCR). The Oncology Patient Information System (OPIS) was the source of data on wait times and treatment practices. The information found in the sections on incidence, mortality, and survival was largely extracted from “Insight on Cancer. News and Information on Colorectal Cancer,” produced by Cancer Care Ontario and the Canadian Cancer Society, Ontario Division. 1 Anatomy of the Colon and Rectum The colon and rectum make up the large intestine, which removes nutrients from food and stores waste until it passes out of the body as fecal material. As shown in Figure 1, the colon starts in the right lower quadrant of the abdomen where the contents of the small intestine enter the cecum. The appendix is attached to the lower part of the cecum. The ascending colon is that part of the colon that runs from the cecum to the hepatic flexure situated in the right upper abdominal quadrant. The transverse colon crosses the abdomen to the splenic flexure lying in the left upper abdominal quadrant. The descending colon extends from the splenic flexure to the left lower abdominal quadrant where it makes an S-shaped loop, which is called the sigmoid colon. The sigmoid colon then connects to the rectum and the junction between the sigmoid colon and the rectum is called the rectosigmoid junction. The rectum extends from the rectosigmoid junction to the anal canal, which ends at the anus. Cancer located anywhere in the colon, including the sigmoid colon, is classified as colon cancer. Cancer found within the rectum, including the rectosigmoid junction, is classified as rectal cancer. As cancers of the colon and rectum have many features in common, they are commonly classified as colorectal. 2 Figure 1 LEFT RIGHT transverse colon splenic flexure hepatic flexure ascending colon descending colon small intestine cecum sigmoid colon appendix rectum anus rectosigmoid junction Risk Factors Colorectal cancer is associated with several risk factors. These include age, diet, family history, and social habits. • Age: As people become older, the likelihood of developing colorectal cancer increases, which explains why most of those diagnosed with colorectal cancer are 50 years of age or older. • Diet: Obesity and centralbody fat result from a poor diet. When coupled with low physical activity, the risk of developing colorectal cancer increases. • Family History: A family history of colorectal or some other cancers is a marker of increased risk, which may be due to heritable factors, similar unhealthy lifestyle, or a combination of these factors. • Personal Medical History: A diagnosis of ulcerative colitis or Crohn’s disease increases the risk of developing colorectal cancer. • Social Habits: Long-term heavy smoking, and excess alcohol consumption, also appear to increase the risk of colorectal cancer. Studies indicate that smokers are 30 to 40 percent more likely than non-smokers to die of colorectal cancer because of a higher incidence of polyps in smokers. FOCUS ON COLORECTAL CANCER IN ONTARIO Incidence of Colorectal Cancer Figure 2 In 2003, it is estimated that there will be 18,000 new cases and 8,300 deaths from colorectal cancer in Canada. In Ontario, it is estimated that there will be 6,800 new cases and 3,000 deaths from colorectal cancer in 2003. Although the age-standardized incidence rates are still lower than those of 1985, the growth and aging of the population has caused the number of new cases to rise steadily and significantly in recent years among both men and women. Figure 3 shows the Key map of Ontario regions E Thunder Bay Sudbury 70 Age-standardized rate per 100,000 (3-year moving averages) 60 50 40 30 20 10 0 1986 1981 1996 1991 2001 Year of diagnosis Female incidence Male incidence Source: Cancer Care Ontario (Ontario Cancer Registry, 2003) Figure 3 Colorectal Cancer Incidence Rates* by Region, 1997–2001 70 Age-standardized rate per 100,000 The incidence of colorectal cancer has fluctuated over the past 20 years but is now slightly higher in males and lower in females than in 1981 (Figure 2). Since 1997, the incidence in men has risen about 2% per year. Female incidence rates have also risen somewhat since 1997 after a steady fall from the early 1980s. The reasons for these trends are not well understood, although changes in diet and social habits likely contributed to the decline in the 1980s. There is no obvious explanation for the recent rise, although the greater use of colonoscopy for screening and /or diagnosis may be a contributing factor. Colorectal Cancer Incidence Rates by Sex in Ontario, 1981–2001 60 50 40 30 20 10 Ottawa CE 0 Kingston SE Hamilton NW NE S SW CW CE SE Region London CW Windsor SW S An enlarged version of this map can be seen in Appendix A * points = incidence estimates; I = 95% confidence intervals – the horizontal line represents the incidence rate for Ontario as a whole Source: Cancer Care Ontario (Ontario Cancer Registry, 2003) 3 E Figure 4 shows the agestandardized mortality rates (death rate per 100,000 population) from colorectal cancer for both men and women over the past two decades. Colorectal cancer mortality fell for both sexes between 1981 and 2001, with a decline of 20% for males and 27% for females. These falls in mortality may reflect the decline in incidence in the 1980s and early 1990s and possibly earlier diagnosis and improvements in treatment. Age-standardized mortality rates by region are displayed in Figure 5. Mortality rates do not vary much by region, but the Northeast and Southwest regions are higher, whereas the Central East region is lower. The horizontal line represents the average mortality rate for all of Ontario. Colorectal Cancer Survival In general, there has been a steady increase in survival for both men and women over the past several decades. This is likely due to improvements in treatment techniques, as well as Colorectal Cancer Age-Standardized Mortality Rates by Sex in Ontario, 1981-2001 40 35 Age-standardized rate per 100,000 (3-year moving averages) Mortality from Colorectal Cancer Figure 4 30 25 20 15 10 5 0 1981 1986 1991 1996 Male mortality Female mortality Source: Cancer Care Ontario (Ontario Cancer Registry, 2003) Figure 5 Colorectal Cancer Age-Standardized Mortality Rates* by Region, 1997–2001 70 60 50 40 30 20 10 0 NW NE S SW CW CE SE Region * points = incidence estimates; I = 95% confidence intervals – the horizontal line represents the average mortality rate for Ontario as a whole 4 2001 Year of death Age-standardized rate per 100,000 geographic distribution of incidence rates in the different regions of Ontario. The Northeast region appears to have the highest incidence rate, whereas the Central East region appears to have the lowest. The Northeast, Northwest, and Southwest regions all have an incidence rate above the provincial average of 51.4 per 100,000. The horizontal line represents the average incidence rate for all of Ontario. Source: Cancer Care Ontario (Ontario Cancer Registry, 2003) E FOCUS ON COLORECTAL CANCER IN ONTARIO Figure 6 Colorectal Cancer Estimated* Five-year Relative Survival † by Region, Age-adjusted, 1996-2000 100 90 80 Relative survival (%) the diagnosis of colorectal cancer at earlier stages, when treatment is more effective. Figure 6 shows the five-year relative survival for Ontario by region, for cases under follow-up during 1996 to 2000. These survival estimates were generated using the Brenner period method of estimating survival, which looks at cases followed within a recent period, 1996 to 2000 in this case. There are not significant differences between regions, except for the Northwest which has a significantly lower relative survival. The horizontal line represents the average relative survival for all of Ontario. 70 60 50 40 30 20 10 0 NW NE S SW Colorectal Cancer Screening CW CE SE E Region Definition of Effective Screening The goals of screening are to decrease the incidence of and mortality from cancer. Effective screening should detect: (1) cancers at an earlier stage with a better prognosis than those detected because of symptoms; and (2) premalignant lesions, which when removed, lead to a decrease in incidence of the disease. Why Colorectal Cancer Screening Meets the Criteria for Effective Screening Colorectal cancer (CRC) may bleed in amounts that are grossly undetectable, but detectable by a fecal occult blood test (FOBT), which, if followed up by colonoscopy, leads to the diagnosis of CRC. Survival with CRC is markedly improved with detection at an early stage. CRC is preceded by the development * Using Brenner’s period method, which estimates survival of all cases under follow-up during 1996-2000, adjusted for age † Bars = survival estimates, I = 95% confidence intervals – the horizontal line represents the average five-year relative survival in the province. Source: Cancer Care Ontario (Ontario Cancer Registry, 2003) of adenomatous polyps, which although rarely detectable by FOBT are detectable and resectable at colonoscopy. Case-control studies of flexible sigmoidoscopy (FS) have demonstrated a reduction in CRC mortality. No previous studies have evaluated the relationship between screening colonoscopy and CRC mortality. However, the National Polyp Study, a cohort study, evaluated CRC incidence following screening colonoscopy. The National Polyp Study consisted of 1418 individuals who had a complete colonoscopy during which one or more adenomas were removed. The subjects subsequently underwent periodic colonoscopy during an average follow-up of 5.9 years, and the incidence of CRC was ascertained. The incidence was compared with that in three reference groups, including two cohorts in which colonic polyps were not removed and one population-based cancer registry (the Surveillance, Epidemiology and End-Results [SEER] cancer registry). A substantial reduction (76-90%) in CRC incidence was observed in the National Polyp Study cohort compared to the expected incidence estimated in the three reference groups (1). 5 Review of Screening Methods and Outcomes FOBT: FOBT is the only modality with randomized controlled trial (RCT) evidence of mortality reduction (2,3). RCTs of periodic (annual or biennial) FOBT show reduction in mortality from CRC from 13%-33% with up to 50% compliance with periodic FOBT. FOBT has both false negative rates and false positive rates for detecting CRC. Individuals with a positive FOBT must be followed up by colonoscopy. Flexible Sigmoidoscopy: FS examines the distal colon and rectum. Lesions observed in this area can be removed or biopsied. Retrospective case-control studies have shown a reduction in mortality from rectosigmoid cancer of 60% to 80% with screening FS, with a protective effect lasting up to 10 years (2,3). Colonoscopy: Colonoscopy detects asymptomatic cancers and precancerous lesions that can be removed. There have been no RCTs comparing screening colonoscopy to other CRC screening methods. In a crosssectional study of screening colonoscopy, 3,121 asymptomatic individuals aged 50 to 75 were recruited from U.S. Veterans Administration hospitals (4). The subjects had no large bowel evaluation within the previous 10 years, and no recent bowel symptoms. Men comprised 96.8%, and 13.9% had a family history of CRC (one or more first-degree relatives). CRC was detected in 1% and non-invasive “neoplasms” (adenomas ≥ 1 cm, villous adenomas, and carcinoma in situ) were detected in 10%. 6 Extrapolating from the National Polyp Study, it is reasonable to assume that screening colonoscopy is a preventive, as well as a screening, intervention. There is no direct information on the optimal frequency of screening colonoscopy for average-risk individuals. For average-risk persons without colonoscopic abnormality, the polyp-cancer hypothesis suggests an interval of 10 years before the next screen. Colorectal Cancer Guidelines and Recommendations in Canada Approximately 75% of CRCs arise in average-risk individuals (defined as 50 years or older with no family history of CRC). CRC screening is effective in reducing both CRC incidence and mortality, as summarized above. After reviewing the scientific evidence for CRC screening, the Canadian Task Force on Preventive Health Care published its recommendations in 2001 (5). For average-risk individuals 50 years or older, annual or biennial fecal occult blood test (FOBT) or FS every five years were recommended as the initial CRC screening tests. The Task Force determined that the evidence was insufficient to recommend for or advise against colonoscopy as the initial CRC screening test. Despite strong evidence demonstrating the effectiveness of CRC screening, there are no population-based CRC screening programs in Canada. In 1999, Cancer Care Ontario (CCO) convened an expert panel to develop recommendations for a CRC screening program in Ontario. The panel recommended the creation of an FOBT-based CRC screening program for average risk individuals between the ages of 50 and 75 (Ontario Expert Panel, 1999). This was echoed in 2002 at the national level by a committee convened by Health Canada (National Committee on Colorectal Cancer Screening, 2002). CCO and its partners are now evaluating two implementation models for FOBT aimed at Ontarians aged 50-75 who are at average risk of colorectal cancer. It is anticipated that the information from this evaluation will assist in planning a population-based CRC screening program in Ontario. Colorectal Cancer Screening in Ontario There is increasing demand for colonoscopic screening from asymptomatic average-risk individuals and their physicians. The volume of colonoscopies in Ontario increased from 62,039 in 1992 to 172,204 in 2001 but it is not known how much of this increase is due to screening versus diagnostic procedures (6). Recently, an Ontario study of nearly one million men and women age 50-59 years with no prior history of CRC or large bowel evaluation revealed that less than 21.5% had any type of large bowel test. This is an upper bound of the extent of screening, since it includes all tests done, whether for screening or for diagnostic work-up (7). There is a great need for educational programs to raise awareness among the public and physicians about the importance of CRC screening. FOCUS ON COLORECTAL CANCER IN ONTARIO Assessing Consistency of Practice against Evidencebased Recommendations The recent development of a software for CCO called DS-Web has made it possible to rapidly interrogate a number of administrative databases, including the Ontario Cancer Registry, the Oncology Patient Information System (OPIS) and the New Drug Funding Program (NDFP) database. Among other things, it can rapidly determine the volume of clinical activity in any cancer centre across the province and analyze radiotherapy and systemic therapy clinical practice patterns. Where stage information is available, it is now possible to describe the stage-specific treatment practices. In the future it should be possible to assess stage-specific survival. In the paragraphs that follow, the recommendations for treatment by type and stage of colorectal cancer are described and then the actual clinical practices are displayed for each of the regional cancer centres. For more information on DS-Web, send inquiries to <[email protected]>. Practice Guidelines and the Treatment of Colorectal Cancer The Gastrointestinal Disease Site Group (DSG) is one of 14 DSGs that develop evidencebased practice guidelines and evidence summaries as part of Cancer Care Ontario’s Program in Evidence-based Care. The Gastrointestinal DSG has 18 members from across the province representing the disciplines of surgical oncology, radiation oncology, medical oncology, anatomical pathology and gastroenterology, in addition to patient representatives and oncology fellows in training. The DSG has completed 14 guidelines and published 12 of them on various aspects of the treatment for different stages of colorectal cancer, as well as other gastrointestinal malignancies. These guidelines can be found on Cancer Care Ontario’s web site, <http://www.cancercare.on.ca/ access_PEBC.htm>. The recommendations found in these guidelines, as well as other sources, are briefly summarized below. Surgical Treatment of Colorectal Cancer For patients presenting with early stage colon and rectal cancer (Stages 0-III), the usual initial treatment is surgical removal (resection) of the tumour, assuming the patient can tolerate the appropriate operation. For those patients who undergo a complete surgical resection, roughly half survive five years. The survival rate depends on the stage of the tumour at the time of surgery. The tumour stage is determined by factors such as the degree of penetration of the tumour into the bowel wall and the extent of lymph node involvement by cancer. The stage of the tumour determines the risk of recurrence and, in higher risk cases, signals the need for further therapy (adjuvant therapy) to reduce the likelihood of recurrence and death from cancer. Colon Cancer When the cancer is detected at an early stage (Stage 0 and some Stage I) and is limited to a polyp, the standard practice is to perform a polypectomy (removal of the polyp). This procedure avoids having to cut into the abdomen by using a colonoscope that is inserted through the rectum. A local excision removes superficial cancers and a small amount of nearby tissue from the inner layers of the colon. If the tumour invades the bowel wall or surrounding tissues, the usual operation is a segmental resection of the colon, where the tumour and a length of normal colon on either side of the tumour is removed. Local lymph nodes are also removed to appropriately stage the patient (10). Accurately staging the patient is important because this signifies whether or not they are eligible for adjuvant chemotherapy, a well-established treatment option for patients with Stage III CRC. Unfortunately, provincewide research confirms that Ontario surgeons and pathologists currently fail to routinely stage CRC and identify those who would benefit from this treatment, even though this can be achieved through a relatively simple change in lymph node retrieval and examination. An initiative to improve colorectal cancer staging in Ontario, led by Dr. Andy Smith from the Toronto Sunnybrook Regional Cancer Centre, is currently underway. Usually, about one-third of the colon is removed, but more or less tissue may be removed depending on the exact size and location of the tumour. After the tumor is removed, the two ends 7 of the remaining colon are reconnected, allowing normal bowel function. In some situations, it may not be possible to reconnect the colon, and a colostomy (an opening in the abdominal wall to allow passage of stool) is needed (10). Rectal Cancer For early stage disease, a polypectomy and local excision can be used to remove superficial cancers or polyps. Local transanal resection involves cutting through all layers of the rectum to remove invasive cancers as well as some surrounding normal rectal tissue. This procedure can be used to remove some Stage I rectal cancers that are relatively small and not too far from the anus. Polypectomy, local excision, and local transanal resection are done with instruments inserted through the anus, without making a surgical opening in the skin of the abdomen (10). Some Stage I rectal cancers and most Stage II or III rectal cancers are removed by either low anterior (LA) resection or abdominoperineal (AP) resection. LA resection is used for cancers near the upper part of the rectum, close to where it connects with the colon. Low anterior resection is like most abdominal operations where an incision is made only in the abdomen. The tumour, along with a margin of normal tissue on either side of it, is then removed. In addition to removing the tumour, lymph nodes and a large amount of fatty tissue around the rectum is removed. The colon is then reattached to the rectum that is remaining so 8 that a permanent colostomy is not necessary. Sometimes, when special techniques are necessary to prevent a permanent colostomy, it is necessary to have a temporary colostomy opening for about eight weeks while the surgical site heals. A second operation is then performed to close the temporary opening (10). An abdominoperineal (AP) resection is performed when the cancer is in the farthest end of the rectum near the anus and involves the sphincter muscle (the muscle that keeps the anus closed and prevents stool leakage). With this procedure, an incision must be made in the abdomen and the perineum, which is the area around the anus. The anus and tissues surrounding it, including the sphincter muscle, are then removed. Having this procedure means a permanent colostomy is necessary to eliminate stool. Recent Advances in Colorectal Cancer Surgery Laparoscopic surgery is a minimally invasive alternative to open abdominal surgery that involves one or more small incisions in the abdomen. The abdomen is insufflated with carbon dioxide gas, which pushes the abdominal wall away from the intestine. Three to five small incisions are made in the abdomen to create ports for inserting a laparoscope, a pencilthin instrument with its own lighting system and miniature video camera, and special surgical instruments. The surgeon performs the entire operation by observing the image projected by the camera on a monitor. The resected portion of the colon or rectum is then removed by enlarging one of the ports and pulling it through (12). Laparoscopic surgery provides the benefits of less postoperative pain, a shorter hospital stay and a shorter recuperation period (11). Total mesorectal excision (TME) has been shown to reduce the local recurrence of rectal cancer compared with non-TME resection and is considered the optimal surgical intervention (13). The mesorectum is the fatty tissue surrounding the rectum under the peritoneum and limited by the fascia recti. It contains vessels and nodes and is separated from the pelvic wall by an avascular plane. A sharp dissection allows the resection of the mesorectum along this avascular plane. The mesorectum is surrounded by a fascia which should be kept intact and removed with the specimen. Nodules of cancer can be found in the mesorectum as far as 5 cm below the lower tip of a tumour. Therefore, if the tumour is located in the upper part of the rectum, the mesorectal excision should be made up to 5 cm below the lower edge of the tumour. For mid or low rectal cancers, a total mesorectal excision should be performed (14). TME is a specialized resection technique that requires some training, so an extensive effort to mentor surgeons in the technique of TME is underway provincially. This initiative is being led by Dr. Marko Simunovic from the Juravinski Cancer Centre in Hamilton. FOCUS ON COLORECTAL CANCER IN ONTARIO Adjuvant Therapy of Early Stage Colorectal Cancer In Stage I colon and rectal cancers where the tumour is superficial and does not penetrate deeply into the bowel wall, the survival at five years following surgical resection is > 90%. These patients do not require any adjuvant treatment. The treatment of Stages II and III differs for colon and rectal cancers. In Stage II colon cancer, where the tumour has a deeper penetration into the bowel wall, or penetrates through the wall, but without involvement of the lymph nodes, routine adjuvant chemotherapy is not recommended, as no effective adjuvant therapy for this group has yet been identified. In Stage III colon cancer where the lymph nodes are involved by cancer, the risk of recurrence is high, ranging from 50 – 70%. For these patients, six months of adjuvant chemotherapy with 5-FU and leucovorin (LV) is recommended with an estimated absolute improvement in five-year survival of 15%. Rectal cancer differs from colon cancer by the need to treat both Stages II and III. In these patients, postoperative radiotherapy is added to chemotherapy in view of the risk for local recurrence of tumour in the pelvis. Treatment consists of six months of 5-FU based chemotherapy combined usually in the third post-operative month with five weeks of radiation. The administration of a continuous intravenous infusion of 5-FU concurrent with the radiation therapy appears to achieve the best results. Though postoperative radiotherapy in combination with chemotherapy is the recommended standard of care in North America, there are emerging data from Europe indicating that preoperative radiotherapy is also effective. Ongoing clinical trials to compare these approaches to the timing of radiation therapy relative to surgery, as well as the role of chemotherapy, are being conducted. Management of Metastatic Colorectal Cancer (CRC) The management of metastatic colon and rectal cancers is the same and guidelines developed by the DSG are common to both sites. In the last two decades, there have been significant advances in the treatment of metastatic CRC. New drugs have become available and more effective chemotherapy drug combinations have been developed. Three groups of drugs are presently available for the systemic treatment of metastatic CRC: The fluoropyrimidines, irinotecan and oxaliplatin. 5-Fluorouracil (5-FU) is a fluoropyrimidine and for over 30 years it has been the principal drug for treating colorectal cancer. It is a thymidylate synthase (TS) inhibitor- an important enzyme in DNA synthesis. Its initial use as a single agent was associated with minimal benefit. The addition of leucovorin (LV), also known as folinic acid (FA), led to improved anticancer effects and the combination of 5-FU/LV (5-FUFA) became standard therapy for several years. Subsequently, other TS inhibitors such as raltitrexed (tomudex) and capecitabine (xeloda) were developed and these had an easier administration schedule with a better toxicity profile. The DSG guidelines recommend their use as alternative options for patients selected for monotherapy when an easier and better tolerated schedule is desired. Capecitabine’s use as first line monotherapy is increasing in view of its ease of oral administration, as well as its better toxicity profile when compared to 5-FU/LV. When compared to 5-FU/LV in randomized studies, patients treated with capecitabine have shown similar survival outcomes but with higher response rates. The second compound that has had a significant impact on CRC outcomes is irinotecan, a topo-isomerase I inhibitor that interferes with DNA replication. Irinotecan has demonstrated significant survival benefit when compared to best supportive care in patients who have failed first line therapy with 5-FU/LV. Guidelines developed by the DSG recommend the use of this drug as a second line therapy. Monotherapy is associated with a median survival of about 12 months in patients with metastatic colorectal cancer, a modest improvement from the six months median survival observed in untreated patients. The use of irinotecan in combination with 5-FU/LV as first line therapy has demonstrated a 9 significant improvement in response rate, time to progression, and overall survival when compared to standard 5-FU/LV. It has become the recommended standard combination for the first line therapy of metastatic CRC in medically appropriate patients. Oxaliplatin, a third generation platinum compound not yet available on the Canadian market, has demonstrated success in the treatment of CRC. Randomized trials have demonstrated its efficacy in first and second line therapy in metastatic CRC. Oxaliplatin is synergistic with 5-FU and should be used in combination with 5-FU/LV even in patients who have had disease progression on 5-FU/LV therapy. Recent studies have confirmed that the use of short infusion schedules of 5-FU/LV in combination with either irinotecan (FOLFIRI regimen) or oxaliplatin (FOLFOX regimen) is associated with higher efficacy and less toxicity. Infusional therapy has emerged as the new standard of care in combination chemotherapy for CRC. Of interest is the fact that capecitabine administered orally for two weeks out of every three weeks can emulate the results of a 5-FU infusion and ongoing combination trials are evaluating its use as an alternative to intravenous 5-FU infusions. Combination chemotherapies in the first line therapy of metastatic CRC have led to an increase in the median 10 survival of patients to about 16 months and data on the use of sequential combinations are demonstrating a further increase to a median survival of 20-22 months. The decision to use sequential monotherapy or combination chemotherapy depends on several clinical factors that include patient age, performance status, comorbidities, and the willingness of the patient to accept treatment with its trade-offs of drug-induced toxicities against the prospect of modest survival and quality of life gains. Observations on the Treatment of Colorectal Cancers at the Regional Cancer Centres The data displayed in figures 7-15 were extracted from two of Cancer Care Ontario’s administrative databases, the Oncology Patient Information System (OPIS) and the New Drug Funding Program’s database, using DS-Web. In order to evaluate practice relative to evidence-based recommendations, it was necessary to select only those cases for whom stage information was recorded in the chart electronically. The capture of stage information has improved at all cancer centres but is still incomplete, which may account for the modest number of cases seen in some analyses. In 2002, 86% of patients diagnosed with colorectal cancer at the regional cancer centres were staged. However, at the provincial level in 2001, the last year for which data from the Ontario Cancer Registry are available, only 19.5% of patients diagnosed with colorectal cancer had information on stage assignment available. Radiation Therapy Radiation is used as part of the treatment for patients with Stage II and III rectal cancer and for palliation of symptoms in patients with advanced unresectable or recurrent rectal cancer. When adjuvant treatment is offered, it can be given pre- or post-operatively (before or after surgery). If delivered preoperatively for tumours that appear resectable, it may be administered in a few fractions, usually as a total dose of 25Gy in five fractions in one week, or as multiple fractions (for example, 45 Gy in 20 to 25 fractions over four to five weeks). The relative merits of these two schedules are being examined in ongoing trials. The longer schedule is generally preferred when the primary tumour is of borderline resectability, and surgery is usually performed about four to eight weeks after radiation, to allow time for downsizing of the cancer. If radiotherapy is administered post-operatively, a dose of 45Gy in 25 fractions in five weeks is considered standard, and may be supplemented by boost therapy to the tumour bed of 5.4 to 9Gy in 3 to 5 fractions, if it is judged that the boost can be given safely. FOCUS ON COLORECTAL CANCER IN ONTARIO Figure 7 provides an analysis of the treatment administered in the regional cancer centres and it shows that the majority of cases are being treated with 25-30 fractions, which is considered acceptable. Those patients being Figure 7 treated for curative intent with less than 25 fractions are likely to be pre-operative radiotherapy cases and the variability seen here is likely due to local management preferences. For the small number of cases treated with > 30 fractions, there may be tumour related factors that required treatment with higher doses. Higher doses are almost invariably given to incompletely resected cancers. Percentage of Stage II and III Rectal Cases Treated with Curative Intent Grouped by Number of Radiotherapy Fractions Given, Jan – Dec 2002 100% Number of Treated Cases 80% 60% A. >30 B. 25-30 C. <25 40% 20% 0% No. of Cases: HAM 78 KNG 21 LND 65 NEO 32 NWO 8 OTT 43 TSB 89 WND 20 ALL RCC 356 Regional Cancer Centre Source: Cancer Care Ontario (Oncology Patient Information System, 2003) Legend: HAM = Hamilton Regional Cancer Centre OTT = Ottawa Regional Cancer Centre KNG = Kingston Regional Cancer Centre TSB = Toronto Sunnybrook Regional Cancer Centre LND = London Regional Cancer Centre WND = Windsor Regional Cancer Centre NEO = Northeastern Ontario Regional Cancer Centre RCC = Regional Cancer Centre NWO = Northwestern Ontario Regional Cancer Centre 11 Advanced rectal cancer is usually treated for palliation by a few fractions (10 or less), although in some cases a more Figure 8 prolonged course can be indicated. Figure 8 shows that the majority of patients being treated with palliative intent in the regional cancer centres are in fact given 10 or fewer fractions. Percentage of Rectal Cases (all stages) Treated with Palliative Radiotherapy, Grouped by Number of Fractions Given, Jan – Dec 2002 100% Number of Treated Cases 80% 60% A. >10 B. 0-10 40% 20% 0% No. of Cases: HAM 11 KNG 14 LND 20 NEO 10 NWO 4 OTT 20 Regional Cancer Centre Source: Cancer Care Ontario (Oncology Patient Information System, 2003) 12 TSB 40 WND 1 ALL RCC 120 FOCUS ON COLORECTAL CANCER IN ONTARIO Systemic Therapy of Rectal Cancers Stage II and III rectal cancers, when offered adjuvant systemic therapy are treated with 5-FU/FA, 5-FU with radiation therapy (RT), 5-FU for four or five days, or 5-FU by continuous intravenous infusion (CIV) and concurrent radiotherapy. All of these regimens are considered appropriate and as Figure 9 indicates, these are the regimens predominantly used at the regional cancer centres. Figure 9 Capecitabine (CAPEC) and Raltitrexed are not standard therapies, although in some cases, these TS inhibitors can be substituted for 5-Fluorouracil when ease of administration is preferred or when severe toxicity results from the administration of 5-Fluorouracil. The presence of 5-FU-mitomycin (5-FU-MITO) is appropriate for treatment of squamous cell cancer involving the anal canal rather than the treatment of adenocarcinomas of the rectum. Etoposide-carboplatin (ETOPCARBO) is also appropri- ate for squamous cell cancer but would not be used with adenocarcinoma of the rectum. Irinotecan in combination with 5-Fluorouracil and leucovorin (IFL) is a regimen used in metastatic or Stage IV colorectal cancer and would not be expected to be used in the adjuvant setting. The inclusion of a small number of these cases in the data may either represent inappropriate use of the regimen, or an error in the recording of stage information in the health record. Percentage of Stage II and III Carcinomas of the Rectum and Rectosigmoid Treated with Adjuvant Chemotherapy Grouped by Regimen Given, Jan – Dec 2002 100% RALTITREXED 80% Number of treated Case OTHER REG 5-FU-MITO 60% IFL 5-FUFA 5-FU CIV + RT 40% 5-FU- 4 OR 5 DAYS ETOPCARBO 20% CAPEC 0% No. of Cases: HAM 96 KNG 60 LND 89 NEO 68 NWO 38 OTT 94 TSB 59 WND 72 ALL RCC 576 Regional Cancer Centre Source: Cancer Care Ontario (Oncology Patient Information System, 2003) 13 Figure 10 demonstrates that the vast majority of patients seen in regional cancer centres with Stage II and III rectal or rectosigmoid carcinoma are treated appropriately with adjuvant therapy. The presence of IFL in the data set may Figure 10 represent a data entry error at the centre, while the presence of etoposide-carboplatin may be due to the inclusion of patients with anal cancer. In unusual circumstances where 5-Fluorouracil could not be delivered or had previously caused severe toxicity, the use of Capecitabine or Raltitrexed as a substitute would be appropriate adjuvant therapy. Percentage of Stage II and III Cancers of the Rectum and Rectosigmoid Treated by Adjuvant Systemic Therapy Grouped as Consistent or Inconsistent with Practice Guidelines, Jan – Dec 2002 100% 90% Number of Treated Cases 80% 70% OTHER REG 60% IFL ETOPCARBO 50% 5-FU-MITO 40% CAPEC 30% CONSISTENT 20% Acceptable Regimens: 10% 0% No. of Cases: HAM 65 KNG 29 LND 58 NEO 36 NWO 8 OTT 62 Regional Cancer Centre Source: Cancer Care Ontario (Oncology Patient Information System, 2003) 14 TSB 28 WND 41 ALL RCC 327 • 5-FUFA • 5-FU CIV+RT • 5-FU-4 or 5 Days FOCUS ON COLORECTAL CANCER IN ONTARIO Systemic Therapy of Colon Cancers The GI Disease Site Group does not recommend the routine use of adjuvant chemotherapy in Stage II colon cancer. As can be seen in Figure 11, the number of Figure 11 patients who actually received adjuvant 5-FUFA treatment is relatively small. When it is used, it is for those patients considered to be at higher risk of recurrence due to poor prognostic factors. The fact that a small number of colon cancer cases are coded as having received anastrozole or paclitaxel and carboplatin suggests that these patients have, in addition to Stage II colon cancer, other malignancies, possibly breast and/or lung cancer. Percentage of Stage II Colon Cancers Treated with Adjuvant Systemic Therapy Grouped According to Treatment Regimen Used, Jan – Dec 2002 100% ANASTRO Number of Treated Cases 80% PACLICARBO IFL 60% 5-FU CIV + RT 5-FU- 4 OR 5 DAYS 5-FU (IV/CIV)+RT 40% CAPEC OTHER REG 20% 5-FUFA 0% No. of Cases: HAM 20 KNG 6 LND 9 NEO 6 NWO 4 OTT 20 TSB 4 WND 9 ALL RCC 78 Regional Cancer Centre Source: Cancer Care Ontario (Oncology Patient Information System, 2003) 15 The standard of care for patients with Stage III colon cancer is adjuvant 5-FU with folinic acid (5-FUFA). As can be seen in Figure 12, this is the dominant treatment offered in regional cancer centres. Capecitabine (which is metabolized to 5-Fluorouracil within the body) is easier to administer and would be an appropriate alternative in Figure 12 circumstances where intravenously administered chemotherapy is difficult or impossible. The inclusion of cases in this data set of 5-FU in combination with radiation therapy (5-FU + RT and 5-FU CIV + RT) is inappropriate for the adjuvant management of colon cancer and these cases are likely rectal cancers inappropriately coded as colon cancer. Irinotecan- 5-FU-leucovorin (IFL) is inappropriate for the adjuvant therapy of colon cancer and may represent a data entry error as this treatment would only be used for Stage IV cancer. Anastrozole is used in the management of breast cancer and its inclusion in the data set likely represents treatment for a second cancer. Percentage of Stage III Colon Cancer Treated with Adjuvant Systemic Therapy According to Chemotherapy Regimen Used, Jan – Dec 2002 100% ANASTRO 80% Number of Treated Cases IRINOTECAN IFL 5-FU-LEV 60% 5-FU- 4 OR 5 DAYS 5-FU (IV/CIV)+RT CYCLO-PO 40% CAPEC OTHER REG 20% 5-FUFA 0% No. of Cases: HAM 65 KNG 18 LND 45 NEO 33 NWO 15 OTT 57 Regional Cancer Centre Source: Cancer Care Ontario (Oncology Patient Information System, 2003) 16 TSB 22 WND 23 ALL RCC 278 FOCUS ON COLORECTAL CANCER IN ONTARIO Figure 13 demonstrates that the adjuvant systemic therapy used in the treatment of patients with Stage III colon cancer is very consistent with the guideline Figure 13 recommendations of the GI Disease Site Group. Only a relatively few cases would be considered unacceptable and these, in fact, may represent coding errors, data entry errors or patients who have other malignant diseases in addition to colon cancer. Percentage of Stage III Colon Cancer Treated with Adjuvant Systemic Therapy Grouped as Consistent or Inconsistent with Practice Guidelines Recommendations, Jan– Dec 2002 100% Number of Treated Cases 80% ANASTRO CYCLO-PO 60% IRINOTECAN CAPEC OTHER REG 40% CONSISTENT 20% Acceptable Regimens: 0% No. of Cases: HAM 65 KNG 18 LND 45 NEO 33 NWO 15 OTT 57 TSB 22 WND 23 ALL RCC 278 • 5-FUFA • 5-FU CIV+RT • 5-FU-4 or 5 Days • 5-FU-LEV • IFL Regional Cancer Centre Source: Cancer Care Ontario (Oncology Patient Information System, 2003) In the management of Stage IV (metastatic) colon cancer, a number of different chemotherapy regimens are acceptable according to the Disease Site Group guidelines. The approaches include monochemotherapy with Capecitabine and Raltitrexed and combination chemotherapy regimens based on 5-Fluorouracil, usually in combination with folinic acid and Irinotecan. Figure 14 shows Capecitabine, Irinotecan with 5-Fluorouracil and Leucovorin (IFL), and 5-Fluorouracil with folinic acid (FUFA) as the dominant regimens used at the cancer centres. 17 Figure 14 Percentage of Stage IV Colon Cancer Treated with Systemic Chemotherapy According to Chemotherapy Regimen First Used, Jan – Dec 2002 100% RALTITREXED MITOMYCIN 80% Number of Treated Cases IRINOTECAN 5-FU CIV + RT 60% 5-FU (IV/CIV)+RT ETOP-PO CISPETOP -3 DAYS 40% CAPEC IFL OTHER REG 20% 5-FUFA 0% No. of Cases: HAM 22 KNG 6 LND 11 NEO 22 NWO 10 OTT 34 TSB 10 WND 16 ALL RCC 131 Regional Cancer Centre Source: Cancer Care Ontario (Oncology Patient Information System, 2003) When these regimens are grouped together as acceptable, as seen in Figure 15, only a few residual cases are identified as receiving “inappropriate” therapy. The use of cisplatin-etoposide may indicate the co-existence of another cancer or of a small cell tumour rising in the gastrointestinal tract. Overall, these data show that the practitioners in the regional cancer centres treating metastatic colon cancer use treatment regimens that are judged to be appropriate according to the guidelines of the provincial Disease Site Group. 18 Role of Palliative Care Palliative care plays a very important role in the management of colorectal cancer patients because, as noted in the section on colorectal cancer survival, the five-year survival of colorectal cancer patients remains less than 60%. Many patients with metastatic disease would benefit from the expertise of a palliative care team to assist in symptom management, psychosocial support, and attention to spiritual needs. Unfortunately, there is little information about the proportion of colorectal cancer patients who actually have access to such important supportive care and palliative care assistance. In some cancer treatment facilities, palliative care clinics have been established to support the needs of cancer patients generally, and particularly those with symptoms that are proving difficult to manage with conventional medical interventions. Future initiatives should optimize the integration of supportive care and palliative care services into the management of the patient with colorectal cancer particularly if they have metastatic disease. And there is a need for more data on the proportion of patients who are provided such care and the degree to which their symptoms are palliated. FOCUS ON COLORECTAL CANCER IN ONTARIO Figure 15 Percentage of Stage IV Colon Cancer Patients Treated with First-Line Systemic Therapy Grouped as Consistent or Inconsistent with Practice Guidelines, Jan – Dec 2002 Number of Treated Cases 100% 80% MITOMYCIN 60% ETOP-PO CISPETOP - 3 DAYS OTHER REG 40% CONSISTENT Acceptable Regimens: 20% 0% No. of Cases: HAM 22 KNG 6 LND 11 NEO 22 NWO 10 OTT 34 TSB 10 WND 16 ALL RCC 131 • RALTITREXED • IRINOTECAN • 5-FU CIV+RT • 5-FU(IV/CIV)+RT • CAPEC • IFL • 5-FUFA Regional Cancer Centre Source: Cancer Care Ontario (Oncology Patient Information System, 2003) Access to Cancer Treatment – Wait Times It is not known at what point waiting for cancer treatment can lead to physical harm. Intuitively, it makes sense to begin treatment as promptly as possible after the diagnosis of cancer. On the other hand, cancer takes many years to reach a size that is clinically detectable, so several weeks or months of waiting may actually have little or no impact on the ultimate outcome. There are data to show that anxiety levels are high for people awaiting a diagnosis, and again from diagnosis to the actual start of treatment. In this context, the Canadian Association of Radiation Oncologists recommends that the time interval from referral to the start of treatment should be no longer than four weeks. There are, however, no standards for wait times for surgery or the administration of chemotherapy. From a study of surgical wait times at hospitals associated with cancer centres in Ontario and published in the CMAJ in August of 2001, the average wait time from referral to colorectal surgery was 36 days (8). Wait time data during 2003 from the Princess Margaret Hospital, University Health Network, suggested an even more serious waiting time problem, as the time from the decision to operate and the date of the operation was 37 days for gastrointestinal cancers. The rate limiting steps appear to be access to operating rooms and the availability of specialized personnel, including anaesthetists. Surgical data in Ontario are incomplete so wait times are difficult to estimate. CCO has taken action and is conducting a Cancer Surgery Wait Times Pilot Project at the request of the Ministry of Health and Long-Term Care. CCO is collecting cancer surgery wait times data and plans to merge this data with 19 from referral to consultation and consultation to treatment. When compared to Figures 18a and 18b, which show the average systemic therapy wait times for colorectal cancer for the same period, there is a noticeable difference in how long patients wait from consultation to treatment. This difference can be attributed to the fact that chemotherapy treatment does not have the same resource constraints as radiation therapy, that already collected by the University Health Network. At the same time, CCO is developing plans for the implementation of a province-wide database so that data collection will eventually be automated. Radiation Therapy Figures 16a and 16b show the average radiation therapy wait times (50th percentile and 90th percentile) for colorectal cancer or surgery for that matter. Therefore, waiting times for chemotherapy are generally shorter. Where wait times exceed two weeks from either referral to consultation or consultation to treatment, the underlying cause is usually either a shortage of medical oncology consultants or poor access to imaging studies (CT or MRI scan), which are necessary to assess the disease extent prior to the start of treatment. Figure 16a Radiation Therapy Wait Times for Colorectal Cancer (colon, rectum, rectosigmoid) 2000 Q1 to 2003 Q1 Weeks Wait 20 Referral to Consultation 15 10 5 8.4 8.3 6.7 6.6 3.0 2.7 3.0 3.3 7.0 6.2 6.0 3.2 3.1 5.6 2.8 2.5 6.7 6.4 6.0 4.8 2.9 2.6 1.7 1.1 4.3 1.4 0 Valid No. of Cases 2000 Q1 2000 Q2 2000 Q3 2000 Q4 2001 Q1 2001 Q2 2001 Q3 2001 Q4 2002 Q1 2002 Q2 2002 Q3 2002 Q4 2003 Q1 90 78 67 77 90 76 96 76 97 102 102 100 96 Figure 16b 20 Consultation to Treatment Weeks Wait 15 10.0 10 5 7.7 3.6 8.1 7.0 7.0 2.9 9.6 3.1 3.7 3.5 7.9 3.1 9.0 9.9 9.1 10.3 11.0 7.6 2.8 3.1 3.1 3.3 3.1 4.0 3.1 0 Valid No. of Cases 2000 Q1 2000 Q2 2000 Q3 2000 Q4 2001 Q1 2001 Q2 2001 Q3 2001 Q4 2002 Q1 2002 Q2 2002 Q3 2002 Q4 2003 Q1 93 81 69 83 86 80 100 75 98 112 103 106 95 50th Percentile Note: Excludes all patients whose wait times exceed 20 weeks. Source: Cancer Care Ontario (Oncology Patient Information System, 2003) 20 90th Percentile FOCUS ON COLORECTAL CANCER IN ONTARIO Figures 17a and 17b would lead one to believe that the average wait times for colon cancer radiation treatment are quite good and conform to the Canadian Association of Radiation Oncologists’ recommendations for a time interval of four weeks or less from referral to treatment. This may be misleading because most of the treatment for colon cancer is palliative, where patients only receive one to two fractions of radiation. This is in contrast to the situation for patients who receive treatment with curative intent, which requires a much larger number of fractions. From a resource scheduling perspective, it is much easier to book one to two palliative appointments, as opposed to 10-20 appointments for curative intent. Figure 17a Radiation Therapy Wait Times for Colon Cancer 2000 Q1 to 2003 Q1 20 Referral to Consultation Weeks Wait 16.4 15 12.4 9.9 10 9.6 3.2 2.7 1.9 2.6 5.0 2.3 2.4 7.9 7.0 5.0 5 8.9 8.1 7.4 4.4 2.7 1.9 4.7 3.6 3.0 1.9 1.4 1.4 0 Valid No. of Cases 2000 Q1 2000 Q2 2000 Q3 2000 Q4 2001 Q1 2001 Q2 2001 Q3 2001 Q4 2002 Q1 2002 Q2 2002 Q3 2002 Q4 2003 Q1 21 20 12 11 22 11 19 19 17 25 27 27 27 Figure 17b 20 Consultation to Treatment Weeks Wait 15 13.3 10.9 10 8.9 7.7 6.0 5 1.8 3.9 1.1 1.1 8.6 7.0 5.9 3.4 1.8 9.4 8.0 7.0 2.0 1.4 2.7 3.3 0.9 1.9 1.7 2.0 1.0 0 Valid No. of Cases 2000 Q1 2000 Q2 2000 Q3 2000 Q4 2001 Q1 2001 Q2 2001 Q3 2001 Q4 2002 Q1 2002 Q2 2002 Q3 2002 Q4 2003 Q1 26 24 14 15 23 13 21 19 19 29 29 31 32 50th Percentile 90th Percentile Note: Excludes all patients whose wait times exceed 20 weeks. Source: Cancer Care Ontario (Oncology Patient Information System, 2003) 21 interval of two weeks, mainly due to the lack of availability of specialists to see the patients. The wait times from consultation to treatment are well below the recommended two week time interval. This results from the Systemic Therapy Figures 18a and 18b show the average wait times for colorectal cancer systemic therapy. The wait from referral to consultation exceeds the recommended time fact that there are fewer inherent resource constraints for the treatment of patients with systemic therapy. Figure 18a Systemic Therapy Wait Times for Colorectal Cancer (colon, rectum, rectosigmoid) 2000 Q1 to 2003 Q1 20 Referral to Consultation Weeks Wait 15 10 7.9 2.9 2.4 3.1 3.0 2.9 5.9 5.7 5.7 5.3 5.4 5 7.3 6.3 3.1 3.1 3.3 7.0 3.0 3.1 9.0 7.7 7.0 2.9 7.4 2.6 3.0 0 Valid No. of Cases 2000 Q1 2000 Q2 2000 Q3 2000 Q4 2001 Q1 2001 Q2 2001 Q3 2001 Q4 2002 Q1 2002 Q2 2002 Q3 2002 Q4 2003 Q1 243 205 212 244 247 219 198 207 202 207 188 181 172 5.7 5.6 Figure 18b 20 Consultation to Treatment Weeks Wait 15 10 6.6 5.0 4.7 5 1.6 1.6 4.9 1.4 6.6 1.6 1.5 1.7 1.1 6.7 6.0 5.0 4.6 4.6 3.9 1.0 1.1 1.6 1.6 1.0 1.6 0 Valid No. of Cases 2000 Q1 2000 Q2 2000 Q3 2000 Q4 2001 Q1 2001 Q2 2001 Q3 2001 Q4 2002 Q1 2002 Q2 2002 Q3 2002 Q4 2003 Q1 229 198 205 232 238 217 198 199 192 197 180 177 169 50th Percentile Note: Excludes all patients whose wait times exceed 20 weeks. Source: Cancer Care Ontario (Oncology Patient Information System, 2003) 22 90th Percentile FOCUS ON COLORECTAL CANCER IN ONTARIO Cancer Care Ontario posts wait time information on its web site <http://www.cancercare.on.ca/ access_waitTimes.htm>. These wait times represent the median (average) wait times from referral to treatment for the preceding three months and are updated monthly from the regional cancer centres and Princess Margaret Hospital. For the three-month period June to August 2003, the median wait time from referral to start of radiation treatment for colorectal cancer by centre is shown below. Although the data shows gastro-intestinal cancer wait times, colorectal makes up such a large proportion of the cases (approximately 90%) that the numbers fairly represent the wait times for colorectal cancer. Gastro-Intestinal [GI] Radiation Therapy Wait Time Information for a Three-month Period, June – August 2003 Centre Weeks Hamilton Regional Cancer Centre 4.5 Kingston Regional Cancer Centre 2.3 London Regional Cancer Centre 4.2 Northeastern Regional Cancer Centre 5.7 Northwestern Regional Cancer Centre 7.1 Ottawa Regional Cancer Centre 6.6 Princess Margaret Hospital 3.1 Toronto-Sunnybrook Regional Cancer Centre 5.6 Windsor Regional Cancer Centre 7.1 The benchmark time interval from referral to treatment for colorectal cancer is four weeks and, as can be seen, not all radiotherapy treatment centres achieve this standard. 23 Conclusions Colorectal cancer is one of the most common malignancies in Ontario and one of the leading causes of cancer deaths. CRC is commonly cured by surgery alone when diagnosed early. For colon cancer patients with a high risk of recurrence (i.e. Stage III and a subset of Stage II), adjuvant chemotherapy is recommended. Combination chemotherapy with radiation therapy is recommended for patients with Stage II and III rectal cancer. Cancer Care Ontario guideline recommendations appear to have been 24 adopted in regional cancer centres. The available data do not allow us to determine if all patients who could potentially benefit from those therapies actually receive them. After many years in which minimal benefit was achieved with chemotherapy in Stage IV disease, improvements have been seen in survival times in clinical trials. Improvements are anticipated in the general cancer population from the application of the treatment regimens that are recommended by the DSG practice guidelines. A variety of fluoropyrimidine- based therapies either alone or in combination with irinotecan or oxaliplatin can be used to palliate symptoms and prolong survival. Practices in regional cancer centres appear to be generally consistent with evidence-based practice guidelines. However, there are no data to inform us as to whether all candidates who could benefit from these therapies actually receive them. FOCUS ON COLORECTAL CANCER IN ONTARIO Glossary of Terms Adenocarcinoma Cancer that begins in cells that line certain internal organs and that have glandular (secretory) properties. Adenomatous Polyp A non-cancerous growth that protrudes from the bowel wall. Adjuvant chemotherapy The use of anti-cancer drugs after surgery to decrease the chance of the cancer coming back. Adjuvant therapy A treatment method used in addition to the primary therapy; used to increase the effectiveness of treatment. Age-standardized rate The number of new cases of cancer or cancer deaths per 100,000 that a population would have if it had a standard age structure. Standardization is necessary when comparing several populations that differ with respect to age because age has such a powerful influence on mortality and morbidity. Age-specific rate The number of new cases of cancer or cancer deaths during the year, expressed as a rate per 100,000 persons in a given age group. Chemotherapy Treatment using a drug or combination of drugs to kill cancer cells. Combined modality (or multimodality) therapy Two or more types of treatment are given either at the same time or in sequence; may include combinations of radiation, chemotherapy, surgery, or others. Five-year relative survival A measure of the reduction in life expectancy due to a diagnosis of cancer. Relative survival is estimated from life tables as the ratio of the observed survival of cancer cases five years after diagnosis to the expected survival of individuals of the same age in the general population. First-line therapy The first type of therapy given for a condition or disease. Fraction Dose of radiation for a single treatment. Incidence A rate showing how many new cases of a disease occurred in a population during a specified interval of time (usually expressed as number of new cases per unit time per fixed number of people; e.g., number of new cases of cancer per 100,000 persons in one year). Locally advanced cancer Cancer that has spread only to nearby tissues or lymph nodes. Lymph node Small bean-shaped organ that acts as a filter to collect bacteria and other foreign substances from the lymphatic system to be processed by the immune system. Metastasis The spread of cancer cells from the original site to other parts of the body. Modality A type or kind of treatment (surgery, chemotherapy, radiotherapy). Neoadjuvant therapy Therapy given before the primary treatment to treat a cancer to improve the effectiveness of the primary treatment; neoadjuvant therapy can be chemotherapy or radiation therapy. New Drug Funding Program A program to provide equal access to new effective agents for eligible patients throughout the province. As a result, access to expensive drugs is not limited by place of residence or a health care facility’s drug budget. New treatments are introduced in a standard manner on a provincial basis. Ontario Cancer Registry The population-based database that includes information on all diagnoses of cancer reported in Ontario since 1964. It includes limited data about diagnosis (date, type of cancer), death (date, cause), treatment, and the individual (date of birth, sex, census division of residence at diagnosis/ death) for all cancer patients. It does not include data on risk factors, stage, grade, or non-melanoma skin cancers. Palliative treatment Treatment given to relieve the symptoms and reduce the suffering caused by cancer and other lifethreatening diseases. Palliative cancer therapies are given together with other cancer treatments, from the time of diagnosis, through treatment, survivorship, recurrence or advanced disease, and at the end of life. Prevalence The total number of active cancer cases in the population at the current moment in time. Radiation treatment The use of high-energy radiation from x-rays, gamma rays, neutrons, and other sources to kill cancer cells and shrink tumors. Radical treatment Treatment given with the intent of curing the disease. Regimen The plan that outlines the dosage, schedule and duration of treatment. Regional involvement The spread of cancer from its original site to nearby surrounding areas. Risk factors Anything that may increase a person’s chance of developing cancer. It may be an activity, such as smoking, diet, family history, environmental agents or many other things. Second-line therapy Treatment that is given when initial treatment (first-line therapy) doesn’t work, or stops working. Side effect An effect on the body caused by cancer treatment other than the effect on the cancer; also called an adverse reaction. Squamous cell cancer Cancer that begins in squamous cells, which are thin, flat cells that look like fish scales. Squamous cells are found in the tissue that forms the surface of the skin, the lining of the hollow organs of the body, and the passages of the respiratory and digestive tracts. Also called epidermoid carcinoma. Staging A method to describe the extent of a cancer inside the body. If the cancer has spread, the stage describes how far it has spread from the original site to other parts of the body. Standard treatment Treatment that has been proven effective and is commonly used. Surgical resection Removing tissue from the body through a surgical procedure. Systemic disease Disease that affects the whole body rather than only an organ. Systemic treatment Treatment that reaches cells all over the body by travelling through the bloodstream. Three-year moving average Rate calculated using the sum of the new cases of cancer or cancer deaths for a three-year period and the population estimates for those same years. Three-year moving average rates are shown on all graphs describing trends in order to smooth out annual fluctuation. Tumour histology The type of cancer as classified by its appearance under the microscope. Many of the terms here were defined with the assistance of the National Cancer Institute’s cancer dictionary, accessible at http://www.nci.nih.gov/dictionary. 25 References 1. Winawer SJ, Zauber AG, Ho MN, O’Brien MJ, Gottlieb LS, Sternberg SS, Waye JD, Schapiro M, Bond JH, Panish JF, Ackroyd F, Shike M, Kurtz RC, Hornsby-Lewis L, Gerdes H, Stewart ET. Prevention of colorectal cancer by colonoscopic polypectomy. N Engl J Med 1993;329:1977-81. 2. Winawer SJ, Fletcher RH, Miller L. Godlee F, Stolar M, Mulrow C, Woolf SH, Glick S, Ganiats TG, Bond JH, Rosen L, Zapka JG, Olsen SJ, Giardello FM, Sisk JE, Van Antwerp R, Bown-Davis C, Marciniak DA, Mayer RJ. Colorectal cancer screening: Clinical guidelines and rationale. Gastroenterology 1997;112:594-642. 3. Winawer S, Fletcher R, Rex D, Bond J, Burt R, Ferrucci J, Ganiats T, Levin T, Woolf S, Johnson D, Kirk L, Litin S, Simmang C. Colorectal cancer screening and surveillance: Clinical guidelines and rationaleUpdate based on new evidence. Gastroenterology 2003;124:544-560. 4. Lieberman DA, Weiss DG, Bond JH, Ahnen DJ, Garewal H, Chejfec G. Use of colonoscopy to screen asymptomatic adults for colorectal cancer. Veterans Affairs Cooperative Study Group 380. N Engl J Med 2000;343:162-68. 5. Colorectal Cancer Screening: Recommendation statement from the Canadian Task Force on Preventive Health Care. CMAJ 2001;165:206-8. 6. Vinden C, Schultz S, Rabeneck L. Patterns of Colonic Evaluation Procedure Utilization in Ontario, 1996-2001: An ICES Research Atlas; in press. 7. Rabeneck L, Paszat LF. Population-based estimate of the extent of colorectal cancer screening in Ontario. Am J Gastroenterol; in press. 8. Simunovic M, Gagliardi A, McCready D, Coates A, Levine M, DePetrillo D. A snapshot of waiting times for cancer surgery provided by surgeons affiliated with regional cancer centres in Ontario. Can. Med. Assoc. J., Aug 2001; 165: 421 – 425. 9. Goldinger M. Colorectal Cancer – An Overview. Available: http://home.swipnet.se/~w-15548/crc.htm (Accessed 2004 Jan 19). 10. American Cancer Society. Available: http://www.cancer.org (Accessed 2004 Feb 15). 11. National Cancer Institute. Available: http://www.nci.nih.gov (Accessed 2004 Feb 15). 12. Colorectal Cancer Network. Available: http://www.colorectal-cancer.net (Accessed 2004 Feb 15). 13. BC Cancer Agency. Available: http://www.bccancer.bc.ca (Accessed 2004 Feb 15). 14. Mitry E, Barthod F, Penna C, Nordlinger B. Surgery for Colon and Rectal Cancer. Best Practice & Research Clinical Gastroenterology, Volume 16, Issue 2, April 2002, Pages 253-265. 26 FOCUS ON COLORECTAL CANCER IN ONTARIO Practice Guideline Publications of the Gastrointestinal Disease Site Group 1. Figueredo A, Germond C, Maroun J, Browman G, Walker-Dilks C, Wong S and the Gastrointestinal Cancer Disease Site Group. Adjuvant Therapy for Stage II Colon Cancer Following Complete Resection. Cancer Prevention and Control, 1997; 1(5): 379-92. 2. Figueredo A, Fine S, Maroun J, Walker-Dilks C, Wong S and the Gastrointestinal Cancer Disease Site Group. Adjuvant Therapy for Stage III Colon Cancer Following Complete Resection. Cancer Prevention and Control, 1997; 1(4): 304-19. 3. Figueredo A, Germond C, Taylor B, Maroun J, Agboola O, Wong R et al and the Gastrointestinal Cancer Disease Site Group. Post-operative adjuvant radiotherapy or chemotherapy for resected stage II or III rectal cancer. Current Oncology 2000;7(1):37-51. 4. Figueredo A, Rumble RB, Maroun J, Earle CC, Cummings B, McLeod R, Zuraw L, Zwaal C, and the members of Cancer Care Ontario’s Program in Evidence-based Care’s Gastrointestinal Cancer Disease Site Group. Follow-up of patients with curatively resected colorectal cancer: a practice guideline. Cancer. 2003, 3:26 (6 October 2003). 5. Figueredo A, Zuraw L, Wong RKS, Agboola O, Rumble RB, Tandan V, the members of Cancer Care Ontario’s Program in Evidence-based Care’s Gastrointestinal Cancer Disease Site Group. The use of preoperative radiotherapy in the management of patients with clinically resectable rectal cancer: a practice guideline. Medicine 2003, 1:1 (24 November 2003). 6. Figueredo A, Moore M, Germond C, Kocha W, Maroun J, Zwaal C, and the Gastrointestinal Cancer Disease Site Group. Use of irinotecan in second-line treatment of metastatic colorectal carcinoma. Current Oncology 2000;7(1):29-36. 7. Jonker D, Earle C, Kocha W, Moore M, Maroun J, Zuraw L, and the Gastrointestinal Cancer Disease Site Group. Use of irinotecan combined with 5-fluorouracil and leucovorin as first-line therapy for metastatic colorectal cancer. Curr Oncol 2001;8:60-8. 8. Germond C, Maroun J, Zwaal C, Wong S, and the Gastro-intestinal Disease Site Group. Use of raltitrexed in the management of metastatic colorectal cancer. Curr Oncol 1999;6(4):217-23. 9. Figueredo A, Zuraw L, Wong RKS, Agboola O, Rumble RB, Tandan V, and the members of the Gastrointestinal Cancer Disease Site Group. The Use of Preoperative Radiotherapy in the Management of Patients with Clinically Resectable Rectal Cancer: A Practice Guideline. BMC Medicine 2003;1:1. 27 Appendix A Key Map of Ontario Regions E Thunder Bay Sudbury Ottawa CE Kingston SE Hamilton London CW Windsor SW S 28 This document is intended for use by persons involved in the provision of care to colorectal cancer patients and for persons responsible for managing aspects of the cancer system relative to colorectal cancer patients in Ontario. Care has been taken in the preparation of the information contained in this document. Nonetheless, any person seeking to apply or consult the information herein is expected to use independent medical judgement in the context of individual clinical circumstances. Cancer Cancer Ontario makes no representation or warranties of any kind whatsoever regarding this information or use and disclaims any responsibility for their use in any way. Cancer Cancer Ontario retains all copyright in this material, including all text and graphic images. No portion of this material may be used or reproduced, other than for personal use, or distributed, transmitted or “mirrored” in any form, or by any means, without the prior written permission of Cancer Care Ontario. Cancer Care Ontario 620 University Avenue Toronto, ON M5G 2L7 www.cancercare.on.ca Phone: 416-971-9800 E-mail: [email protected]