Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
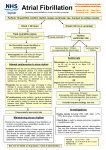
Acute Management of Atrial Fibrillation Dalia Hawwass PGY2 June 2015 Objectives • To review the initial management of atrial fibrillation with RVR in acute setting • Assessment for hemodynamic instability • Indications for urgent cardioversion • Different Rate Control agents Case Vignette • A 75 year old woman with PMHx of HTN, HLD and DM, CKD presents to ED for new onset dizziness, shortness of breath and palpitations that began 3 hours ago while patient was gardening in her lawn. She denies any associated chest pain and no actual loss of consciousness. • Vital Signs: T: 37.5 C, BP 90s/60s (Baseline BP 115/80s), HR 140s-160s bpm and RR 24. A&O x3 with some facial grimmace. Cardiac exam is irregulary irregular without murmurs. Lungs CTAB. Remainder of exam unremarkable. • She received a 2L bolus in the ED without increase in blood pressure EKG What is the next appropriate management for this patient? • A) IV diltiazem • B) Intubation • C) Urgent Cardioversion • D) IV pain control • E) CT pulmonary angiogram Indications for Urgent Direct Cardioversion • Hemodynamic Instability: • Patient with decompensated heart failure • Active ischemia: if symptomatic with angina or evidence of ischemia/infarction on EKG • Evidence of organ hypoperfusion (altered mental status, cold clammy skin, acute kidney injury) Urgent Cardioversion • Electrical Cardioversion: sedate patient and place setting on direct synchronization then shock • Initial shock setting of 100J 200J 300J 360J until sinus rhythm returns • Make sure you perform direct cardioversion with R wave synchronization to prevent an “R on T” phenomenon which can lead to V fib • Restoration of normal sinus rhythm takes precedence over need for protection from thromboembolic risk • Would recommend cardiology consult at this time If Patient is Hemodynamically Stable • Goal is ventricular rate control (<100 bpm) and anticoagulation • Resting HR goal should be 60-85 bpm in symptomatic patient • Roughly 50% of patients with new onset AF will spontaneously convert to NSR spontaneously within 48 hours of onset • Rate control or Rhythm control? • AFFIRM trial and RACE trial • No survival advantage in terms of stroke prevention rhythm control over rate control rate control • Rate control agents • • • • Calcium Channel Blockers Beta blockers (caution in patients with reactive airway disease) Digoxin Amiodarone (for patients intolerant or unresponsive to other agents) Rate Control Agents Drug Classes Drug Loading Dose Maintenance Dose Calcium Channel Blockers (nondihydropyridine)initial DOC Diltiazem 10 mg IV over 2 minutes Can repeat up to 20 mg IV 30 mg PO q6 hrs (can transition to long acting) Can use 10 mg IV q6 hrs prn Beta Blockersinitial DOC Metoprolol 5 mg IVP q5min x3 doses 25 mg PO BID, can uptitrate to 100mg PO BID Digoxin 0.5 mg IV loading dose0.25mg IV in 6 hrs0.25mg IV 6 hrs after 0.125 mg PO QD Amiodarone 150 mg IV/10 min 1mg/minx 6 hrs 0.5 mg/min x 18hrs 100-200 mg PO QD Other Other Rate Control Agents Calcium Channel blockers-non-dihydropyridine agents • IV diltiazem-initial dose 10 mg IV over 2 minutes • Can increase dose to 20mg IV if needed • Maintenance diltiazem 30mg PO q6hrs (short acting) or can transition to total long acting diltiazem • Can also use 10mg IVP q6 hrs prn • Start PO dose at same time as IV dosing, so PO can kick in by time IV dosing wears off Rate Control Agents Beta blockers • Metoprolol- Initial dose: 5mg IVP q5 minutes x3 doses and q6hrs prn • Maintenance Dose: 25 mg PO BID, can uptitrate to 100mg PO BID max • Start PO at same time as IV medication • Esmolol –Initial dose: 500mcg/kg IV over 1 min, can repeat in 5 minutes • Maintenance drip: 50-300 mcg/kg per min IV continuous infusion • Used only in ICU: • Advantage: short duration of action, easy to titrate to heart rate goal Rate Control Agents Digoxin can be used in acute setting but rarely as monotherapy • Initial loading dose: 0.5mg IVthen 0.25mg IV in 6 hrs0.25 mg IV 6 hours after • Maintenance dose: 0.125mg daily PO • Caution in elderly patients and those with renal failure (need to renally dose) • TREAT-AF study-increased risk in mortality in elderly patients by >20% on digoxin • Indicated in patients with LVEF<30% (inotropic agent) Rate Control Agents Amiodarone- both a rate control and rhythm control agent • Initial loading dose: 150 mg IV over 10 minutes, then 1 mg/min x 6 hrs, then 0.5mg/min x18 hrs • Maintenance dose: can change to oral 100mg200mg daily • Can promote cardioversion-so need to be on anticoagulation • Preferred agent in WPW to prevent AF impulses down accessory pathway leading to promotion of VF Case Revisited What is the next appropriate management for this patient? A) B) C) D) E) IV diltiazem Intubation Urgent Cardioversion IV pain control CT pulmonary angiogram Summary • If patient is hemodynamically unstable in setting of atrial fibrillation (with hypotension, angina, decompensated heart failure, AMS) then proceed with direct synchronized cardioversion • Rate control is goal for Afib with RVR for symptomatic management • Initial rate control agents are diltiazem or metoprolol References • Uptodate.com: Topics: Acute Management of Atrial Fibrillation • Uptodate.com: Topics: Rhythm Control vs Rate Control in Atrial Fibrillation • January, Craig T. et al. “2014 AHA/ACC/HRS Guideline for Management of Patient with Atrial Fibrillation: Executive Summary." Journal of American College of Cardiology (2014): n. pag. American College Cardiology Foundation. Web. 29 Sept. 2014. http://content.onlinejacc.org/article.aspx?articleid • wmshp.org/sg_userfiles/Sarigianis_CE_10172013_handout.pptx • King, D, Dickerson, Sack J. Acute Management of Atrial Fibrillation: Part I. Rate and Rhythm Control. Am Fam Physician. 2002 Jul; 66(2): 249-257.