Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
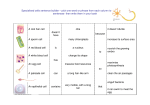
Introduction to tromatodes Phylum Platyhelminthes Class Trematoda Order Digenea Morphology • Adult worm – – – – Flattened (flatworm) and leaf like Sucker: oral & ventral (fluke) Body wall: musculo-tegumental sac Parenchyma (structure between body wall and internal organs): connective tissue fibers, cells and space between them – Digestive tract: not intact i.e. no anal opening, caecum – Reproductive system: hermaphrodite (monoecious) exception of schistosome – Muscular system – Nervous system – Excretory system • Egg – Size divergent – Ovoid – Operculum (exception of that of schistosome) – Content: ovum , vitelline cells, or miracidium Egg of Clonorchis sinensis Egg of Paragonimus westermani Egg of Fasciolopsis buski S. japonicum S. Mansoni S. haematobium Schistosome egg Features Reflecting Adaptation to Parasitism • Organs of attachment highly developed • Retardation of digestive system • Highly developed reproductive system Life Cycle • Complex • Alteration of generation sexual generation and asexual generation alter in the life cycle of parasite • Asexual multiplication in larval stage in snail host • Multiple hosts transfer and having reservoir hosts in majority • Water environment is essential Important Species • Liver fluke: Clonorchis sinensis • Intestinal fluke: Fasciolopsis buski • Lung fluke: Paragonimous westermani P. skrjabini • Blood fluke: Schistosoma spp. The Liver Fluke 肝吸虫 Clonorchis sinensis 中华支睾吸虫 Introduction • Parasite of biliary passage • Cause “clonorchiasis” • A common trematode in Far East • First report 1874 oversea Chinese in India Morphology • Adult worm – Size & Shape like the seed of sunflower – Sucker: oral = ventral – 2 dendritic testes lie in tandem to each other in the posterior region (clonorchis) Adults of Clonorchis sinensis Cross section of Clonorchis sinensis adult in the hepatic bile duct • Egg – Size: smallest – Shape: just like sesame – Color: yellowish brown – Operculum distinct: shoulder, knob – Content: miracidium Clonorchis sinensis egg. These are small operculated eggs. Size 27 to 35 µm by 11 to 20 µm. The operculum, at the smaller end of the egg, is convex and rests on a visible "shoulder". At the opposite (larger, abopercular) end, a small knob or hooklike protrusion is often visible (as is the case here). The miracidium is visible inside the egg. Egg of Clonorchis sinensis Life cycle of Clonorchis sinensis Life Cycle • A model pattern of trematode • Main points – Definitive host: human being – Reservoir host: dog, cat, etc. – Residing: hepatic bile duct – Discharge of eggs with feces – Hatching in the host small intestine – 2 intermediate host I: snails, such as Bithynia,Parafossarulus II: freshwater fishes, such as Cyprinus – 2 generation of asexual proliferation – Infective stage: metacercaria in fish – Infective route: oral consumption Pathogenesis • Due to adult worm • Mechanism – Mechanical: sucker – Chemical: excretions, secretions, metabolite – Biological: nutrition deprivation • Pathological process – Inflammation Proliferation ThickeningOcclusion – Extensive involvementFibrosis of the liver Clinical Manifestations • Acute stage: allergic reaction • Chronic stage: functional impairment of liver (Cholangitis, Cholecystitis, Bile stone, Jaundice, etc) • Advanced stage: portal cirrhosis & malignancy Laboratory Diagnosis • Etiological – Examination of egg in feces by sedimentation method – Duodenal aspiration • Immunological – ELISA to detect antiboby or antigen Epidemiology • Distribution – Far East (China, South Korea, Japan, etc.) – 24 provinces in China (Guangdon: 5 million infected etc.) Endemic Factors • Source of infection: mainly wild carnivores • I,II intermediate host in the same waterfield • Mode of fish breeding • Dinning habit & Customs Principle of Control • • • • • Cure patients & carrier praziquantel:25mg/kg, tid, 2 days Control reservoir host Carry out scientific fish-breeding Hygienic education not eating raw or undercooked fishes Paragonimus westermani 卫氏并殖吸虫 Paragonimus skrjabini (Paragonimus szechuanensis) 斯氏狸殖吸虫 The Lung Fluke • • • • Genus paragonimus Zoonotic parasite (cause zoonosis) Animal infection> human infection 2 major species in China Introduction • Pathogen of lung disease • Endemic hemoptysis • Favorite lodging site: lung • Ectopic site: brain, abdomen, muscle, etc. Morphology • • • • • Adult worm Body thick (a half piece of a bean grain) Tegument: spinous Sucker: oral = ventral Parallel arrangement of reproductive organ lobular testes (posterior) lobular ovary & uterus (anterior) Cross section of lung containing adult Paragonimus westermani. • Egg – Median size, ovoid (water pot) – Golden yellow – Distinctive & wide operculum – Contain 1 germ cell & several yolk cells Egg of Paragonimus westermani. Crab or crayfish Life cycle of Paragonimus westermani. Life cycle • • • • Definitive host: human being Reservoir host: carnivorous animals Habitation: lung & ectopic site Intermediate host: I: Melania snails II: stream crabs, crayfish • Infective stage: metacercaria • Infective mode: oral route, may via paratenic host (swine) • Migration & Preadult wondering • Ectopic parasitism: cerebral, abdominal,etc. • Eggs discharged with sputum & feces • 3 generation of asexual multiplication Pathogenesis • Stage take responsibility: adult & preadult • Pathological processes – Abscess stage(脓肿期) – Cystic stage(囊肿期) – Scar formation stage(纤维疤痕期) • 4 clinical types – Thoracic (pulmonary type):chest pain, coughing, blood-tinged sputum(hemoptysis) – Abdominal (hepatic type):hepatomegaly – Cranial type: dizzy, headache, epilepsy – Musculocutaneous type: migratable subskin nodule Laboratory diagnosis • Disease history + physical examination • Etiological diagnosis eggs in sputum or feces by sedimentation • Immunological diagnosis for ectopic infections Epidemiology • Global main continent except Europe • China 23 provinces Paragonimus westermani infection occurs in Asia (especially in China (Taiwan), Corea, India, Japan, Laos, Philippines, Sri Lanka, Thailand, Viet-Nam), Central-West Africa, South America (Ecuador, Peru Venezuela). Principle of control • Treat patient: praziquantel • Hygienic education • Social construction, economic refinement The Ginger Fluke 姜片虫 Fasciolopsis buski 布氏姜片吸虫 Intestinal fluke 肠道吸虫 Morphology • Adult worm – Like a ginger piece – Big muscular trematode – Have strong suckers,ventral >> oral Adult fluke of Fasciolopsis buski The adult flukes range in size: 20 to 75 mm by 8 to 20 mm Fasciolopsis buskii adult worm • Egg – Biggest – Ovoid – Minute operculum – Yellowish – Germ cell inclusions F.buski eggs are released in feces unembryonated. The operculated eggs are oval, brown and measure 130-150 by 78-100 um Life cycle of Fascilopsis buski Life Cycle • • • • Definitive host: human being Reservoir host: swine, etc. Intermediate host: Planorbis snails Aquatic plant vectors: caltrops, water chestnut, etc. • Habitation: small intestine • • • • Infective stage: metacercaria Infective route: oral Developmental stages: as Paragonimus 3 generation of asexual proliferation Pathogenesis Factors • Traumatic (suckers) • Obstructive (due large size) • Toxic (excretion, secretion, metabolite) Clinical Manifestation • Abdominal pain • Acute intestinal obstruction • Anemia • Generalized edema Laboratory Diagnosis • Examination of egg in feces by sedimentation method Epidemiology • Aquatic plant raising districts Fasciolopsis buski: is endemic in China (Taiwan), South-East Asia, Malaysia and India. Principle of Control • Drug for treatment: praziquantel • Water & nightsoil control; Scientific swine raising • Hygienic education Introduction • 6 species of human schistosomes – – – – – – Schistosoma japonicum S. mansoni S. haematobium S. intercalatum S. mekongi S. malayi Schistosoma japonicum 日本血吸虫 Distribution and Epidemic Situation • Worldwide – 200 million of population infected in 74 countries (S.m. 55; S.h. 55; S.j. 4; S.i. 10; S.me. 2; S.ma. 1) • China 50 years – 11 million in 12 provinces 0.7 million in 8 provinces Before control After control (1996) Regional distribution of S. japonicum infection in China Morphology • Difference from other trematodes – Dioecious adults – Non-opeculate egg – Bifurcated (forked) cercaria invades the final host by skin – Adults parasitize blood vessels • Adult – Male (15 mm length) < female (22 mm) – Oral sucker < ventral sucker – 2 paralleled guts form a blind caecum in the posterior ends – 7 testes in male and single ovary with a tubule uterus in female – Gynecophoric canal (male) in which female repose • Egg – Ovoid and non-opeculate – 74~106 m × 55~80 m – Contains one miracidium – Bear a minute lateral knob. • Miracidium • Cercaria S. japonicum S. Mansoni S. haematobium Schistosome egg Schistosome miracidium Schistosome cercaria Life Cycle Eggs discharged fresh water (hatch) miracidia penetrate oncomelania(I.H.)mother sporocysts (multiplication) daughter sporocysts (multiplication) cercariae (infective form) skin penetration of D.H. schistosomulum right heart lungs left heart systemic circulation portal system pairing and sexual maturation mesenteric veins lay eggs eggs develop and live in tissue for 21 days( 23% in liver tissue, 60% in intestinal tissue, 17% discharged) Cercarial dermatisis due to avian schistosome Main Points of Life Cycle • • • • • • Residing site: mesenteric vein I.H.(Only one): Oncomelania hupensis No metacercaria and redia stage Two generation of sporocyst Infective stage: cercaria Route of infection: skin penetration Adult of Schistosome in mesenteric veins of hamster Onchomelania hupensis Skin penetration of cercaria first appearance of eggs: 30~35 days Life spans in human: 4~5 years, longest: 35 years • Tissue egg – The egg which can develop and live in tissue • Significance of tissue egg – Major pathogenic stage, inflammation and granuloma around the egg – Diagnosis and evaluation of therapeutic efficacy Immunity • Concomitant immunity – Host carrying an initial infection of adult schistosomes shows the protection to a cercarial challenge infection (攻击性感染)and this protective immunity will disappear with eradication of schistosomes in the host • Immuno-evasion: It’s an ability by which the schistosome adult can evade the host immune response. The possible mechanism of evasion. – Acquire host antigen on it surface – Host-like antigen produced by parasite – Changing of tegument very quickly – Parasite may inactivate or down-regulate immune effectors Pathogenesis Schistosomiasis at each stage of the life cycle in human body • Cercaria (skin-penetration) – Dermatitis • Schistosomula (migration) – Larva migrans • Adult: (immunocomplex) – Immuno-nephropathy • Tissue egg: principal pathogenic stage Miracidium within eggSEASensitization of T Cell Th1IL-2, INF-, TNF activate macrophage, induce cell-mediated immunity Th2IL-4, IL-5 stimulate IgE production or eosinophilia inflammation and granuloma fibrosis portal hypertension intestinal polyp Clinical Form • Acute schistosomiasis – Fever, diarrhea, abdominal pain, enlargement of liver or spleen • Chronic schistosomiasis – asymptomatic or diarrhea, abdominal pain, enlargement of liver or spleen • Advanced schistosomiasis – Ascites; splenomegaly;collateral circulation; dwarfism; – Ectopic lesion: encephalitis; focal epilepsy Advanced schistosomiasis patient with portal hypertension and ascites A patient with S. j has marked ascites, splenomegaly, umbilical hernia and distended superficial abdominal veins. Diagnosis • Parasitological diagnosis (etiological, definitive diagnosis) – Demonstrating eggs by stool examination – Stool examination after concentration (sedimentation) – *Miracidium-hatching from eggs – Rectal biopsy — eggs-demonstration Miracidium-hatching from eggs Necessity: tissue ova; low egg burden due to mass treatment Possibility: • Hatch quickly (T:25; limpid water; free of Cl2;light; pH=6.8-7.8) • Three tropism:limpidity, phototrophic, ascendancy • Swimming in a zigzag way • Immunodiagnosis (indirect diagnosis) – Detection of antibodies in serum, urine, saliva by ELISA, but is impossible to distinguish current infection from past infection. – Detection of antigens (circulation anodic and cathodic antigen) • Combined diagnosis: including epidemiological antecedent, symptoms and signs, parasitological and immunological examination. Treatment Praziquantel 60 mg/kg divided in 3 doses. Factors of Transmission and Prevention • Factors – Source of infection: patients and reservoir host – Intermediate host: Oncomelania – Contact with cercaria-infected water • Preventive measures – Detection and treatment of patients and reservoir host – Elimination or control of oncomelania – Protection of susceptible population and avoidance of contact with cercaria-infected water – Prevention of water contamination by human night soil Distinguishing of 3 major schistosomes (see page 54, Table 3-1)