Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
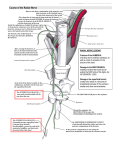
Cervical Anatomy 360º + Massage Taught by Christopher SovereignLMT, CNMT, CBAT, COSM [email protected] Sovereign Seminars on Facebook Cervical Anatomy 360º + Massage Taught by Christopher Sovereign- LMT, CNMT, CBAT, COSM In this class & manual we shall delve layer by layer through the neck, examining the individual tissues. Goal 1. Show the muscles individually. Goal 2. Increase your understanding of location and jobs of the cervical muscles. Goal 3. Show basic massage techniques for each tissue. The posterior neck is classically divided into 4 layers of muscles- AVIIA Upper trap ^ Spleni V Semispinalis II Multifidi & rotatores ^ Landmarks Trapezius Spleni V Semispinalis capitis II Semispinalis cervicis II Multifidi & Rotators ^ Erector Spinae group Spinalis Longissimus cervicis Longissimus capitis Suboccipitals Lateral neck Scalenes Levator scapulae Sternocleidomastoid Anterior neck Hyoid muscles A. supra-hyoids B. Infra-hyoids Longus coli Longus capitis Various Interspinous Rhomboid minor Serratus Posterior Superior Sovereignisms 1 Bump AKA: External Occipital protruberence SNL Superior Nuchal Line (SNL) Inferior Nuchal Line 1 1 C1; note- Does not have a spinous process. It has a small bump called a tubercle C2 ; note- large spinous, the largest in the upper cervical. Smaller than C7 spinous process. C7; note- this is the largest spinous process of the upper body T1; note- large, but smaller than C7. May stick out farther but less massive Note the space between the ‘transverse processes’ and the articular pillars Lateral mass. The group of these are known as an articular pillar 3 Trapezius Upper Trapezius Cranial attachment: External occipital protuberance (EOP), medial portion of superior nuchal line, nuchal ligament, possibly to spinous processes of C2-5. Laterally connects to: Lateral 1/3 of posterior clavicle. [middle trapezius attaches to scapula @ acromium & spine of scapula] Jobs: Elevation of scapula, lateral flexion of head & neck, helps resist weight carried on shoulder, upward rotation of scapula. Stabilization & checkrein of head. Of note: One of the most common muscles to have trigger points, commonly referring to temple & mastoid process (& inferior of it). Massage: Glide with skin @ EOP & superior nuchal line, midline & nuchal ligament, glides from midline out to posterior clavicle ( lateral 1/3 to acromium ). Thumbs are perfect for clavicle work when client is supine. clavicle Spleni Splenius capitis & cervicis V 13/36 Upper trap: lateral attachment: > Lateral 1/3 of the posterior aspect of the clavicle. Note: the upper trap does NOT attach to the scapula. Normally, this structure would be thought of as two structures- one going to the cranium & one to the upper cervicals. In my mind, this is more like a biceps muscle- a muscle with one base and 3 additional insertions. A cervical triceps if you will. Capitis: to the mastoid process and medially to the occiput between superior & inferior nuchal lines. This attachment is deep to ( underneath ) the SCM mastoid attachment. From the midlineFrom C3 lateral spinous process to T6 lateral spinous process. Cervicis section looking medially- Curls around to the lateral neck inserting into the posterior tubercles & posterior transverse processes of C1 & C2 & maybe C3. Jobs: Stabilization of head & neck, rotation of head to same side. Bilaterally: Stabilization & extension of head & neck. Massage: Glides from C3-T6 spinous processes upward & laterally towards mastoid process. Also treat mastoid process & lateral attachments @ C1-3 Of note: Remember this one by V 13/36: Bilaterally this is in a V shape and attaches above to C1-3 & below to C3-T6 Cervicis section- posterior view- note it’s curling about to the lateral. Anatomical landmarks: Spinous processes; mastoid process; C1 TP; C2 & 3 posterior tubercles Questions? Contact us via- [email protected] or 505-363-9004 Please ‘Like’ us on Facebook 5 Semispinalis Cervicis and Capitis Mainly straight up the spine Semispinalis Capitis: ˆC46-T17 From above:to occiput in between the superior and inferior nuchal lines. From below: C4-C6 articular processes, Transverse processes of T1-6 or 7 Actions: Stabilizing of Head in flexion, extension of head It lays in the lamina groove but does not attach to the spinous processes. Semispinalis cervicis: ˆ25/16 SP 25, TP 16 Above: spinous processes of C2-5 Below: Transverse P. of T1-5 or 6 Actions: stabilization of neck in cerv. flexion, extension of cspine, rotation to opposite side. Multifidi & Rotatores 3 These muscles work together typically. Of note: Each one of these is a mini-biceps ( rotatores ) or miniquadriceps ( multifidi ) as from one location on a transverse process these ‘reach up’ to multiple vertebrae above. Multifidi Above- Mid- lateral spinous processes of C2-C5 Below- Articular processes of C4-C7 This muscle spans 2, 3 or 4 vertebrae. Rotatores Above- Spinous process starting at C2 This muscle spans one to two vertebrae. Below- Transverse process starting at C3 and continuing on. Overall- stabilization & specific positioning of individual vertebrae Bilaterally- Extension of vertebral column Unilaterally- help rotate vertebral column towards opposite side.AKA: these muscles tighten on right and the neck is turned to the left. Massage:Gently sink into the lamina groove and perform small glides from a transverse process to the spinous process up one, up two, up three & up four. Repeat at the next vertebrae, working small and gently. Questions? Contact us via- [email protected] or 505-363-9004 Please ‘Like’ us on Facebook 7 Erector Spinae Group: Spinalis, longissimus & iliocostalis Spinalis cervicis- a rainbow m. part of the erector spinae group tends to help control ROM. This is what I call a rainbow muscle. If you looked at this muscle while someone were on their side-it is sharped just like a rainbow. Others think of it like suspension springs on a car. The fibers that attach to the spinous process of C2 have the longest fibers and go all the way back to the spinous process at T3, likewise C3 goes to T2 ( and is slightly shorter in length, C4 to T1, C5 to C7 ( and is the shortest ) Functions: Bilaterally- 1. Stabilization of the vertebral column 2. assist in extension of the vertebral column Unilaterally- lateral flexion of vertebral column ( side bending ) minor player Massage: sink in and gently work into the lateral spinous processes. Longissimus capitis & cervicis Longissimus capitis: a smaller strap of a muscle Below- To the articular processes ( lamina groove ) of C4 or C5 & T1-T4 or T5 Transverse processes Above-Mastoid process Function- 1. Bilaterally-Extension of the head ( think of what this might do in forward head posture ) 2. Unilaterally-Helps to laterally flex the head 3. Rotate head towards same side Longissimus cervicis Below- Superior portions of transverse processes of T1-T4 or T5 Above- Posterior tubercles of C2-C6 Functions: 1. Bilaterally-Extension of the vertebral column 2. Stabilization of cervical vertebrae Unilaterally- 3. lateral flexion towards the same side. Massage: Sink in using gentle glides in the lamina groove out to the transverse processes & the inferior mastoid process. Iliocostalis cervicis The most lateral of the 3 groups comprising the erector spinae muscles. Connects long fibers from the sacrum to the posterior tubercles of the lower cervical vertebrae. Note it is lateral of the transverse processes. Massage: Work between mid thorax and the lateral cervicals. Part of this shall put you in the lateral rhomboid area, as well as very near the posterior scalene. SUBOCCIPITALS This group of 4 muscles on each side are small and important. In their actions they act similar to the spinal ligaments and multifidi lower in the spine, tho acting on the head & first 2 vertebrae. They are frequently involved in headaches via trigger points Major & minor Rectus Capitis Posterior MajorConnects C2 spinous process to the occiput @ inferior nuchal line starting one thumb width lateral of the midline. minor- Connects C1 tubercle to the occiput @ inferior nuchal line starting at midline, is one thumb width wide. Their actions: Primary: stabilizing head, micro adjustments to C1 & C2 vertebrae. Assist in extension (Bilat) & rotation to same side. Massage: Sink into the C1 tubercle & press into the occiput & glide superiorly. Shift one thumb width lateral and repeat from C2. Superior & inferior Obliquus Capitis Superior Connects C1 transverse process & occiput in between superior & inferior nuchal lines. Lateral section is near mastoid process. Obliquus Capitis inferior Connects C2 spinous process to C1 transverse process. Their actions: Primary: stabilizing head, micro adjustments to C1 & C2 vertebrae. Assist in extension (Bilat) & rotation to same side. Massage: find C1TP-work the small area slightly posterior & above for superior. For inferior- work between the large C2 spinous process and C1TP using small partial glides & static pressure holds. Its longer than you might think. 9 Scaleni- anterior, middle & posterior. Of note: The subclavian artery, brachial plexus & auxiliary artery run between the anterior & middle scaleni. These have the ability to compress these arteries directly and the ability to raise up the first rib, compressing this neurovascular bundle indirectly. None attach to C1. The scaleni do not attach in the lamina groove, rather the tubercles of the transverse processes. Scalenus minimus: 7 [exists in at least half/3/4 of people on a minimum of one side] Connects the plural dome with the neck, allowing increased lung expansion. Scalenus anterior: 36/1 middle vertebrae connects the anterior tubercles of C3-6 to the anterior border of the first rib. Scalenus Medius: 27/1 connects the posterior tubercles of C2-7 diagonally with the superior surface of the first rib. Scalenus posterior: 57/2 lower neck: Connects the lowest 3 vertebrae via almost horizontal fibers to rib #2. Jobs: From above: Inspiration. From below: Lateral flexion of the cervical spine ( almost and extension of the lev. scap.), neck flexion, neck stabilization. Working the posterior scalene Glide from 2nd rib to C5 (where line is) My favorite is w/ client in sidelying and using my thumb Massage: Minimus we can’t get to. Anterior is difficult. We won’t be treating in this class. Medius is easily found- it’s just strait lateral and meaty. Posterior is best found in side lying position. From the side it is an easy and short stroke in the lower cervicals. Levator Scapulae Think Bi-14 From above: Transverse process of C1-4 (Posterior tubercles of C2-4) Note the 90º twist from scapula to vertebrae From below: Posterior edge of the superior angle of the scapula Jobs: Elevates shoulder, side bends neck, stabilizes/ counterbalances neck in FHP, May insist in same side ROT, Bilat. cerv. ext. Assists in rotation to same side. C1 (Atlas) @TP C2 (AXIS) @ Post Tub C3 @ Post Tub C4 @ Post Tub Notes: Lev. Scap does elevate the shoulder ( duh ! ) when the neck is fixed. It also can pull the neck laterally 11 Levator Scapulae Superior attachment work: Find C1 TP just inferior to mastoid process. It might be slightly anterior. High attachments: C2-4 Transverse processes (C2-4 posterior tubercles) Find the lateral articular pillars Sink fingertips to bone level Stay at bone level and shift slightly anterior to slight boney prominences ( post. tubercles) . Scapular attachment: Posterior superior angle of the scapula. Find the spine of the scapula at its medial end Glide slightly superior. Massage the posterior edge. Note: At the superior angle is a sandwich- levator scap then serratus anterior. Sternocleidomastoid: The greatest name in muscles Superior attachment is at mastoid process and posterior to lateral half of the superior nuchal line The two lower heads of the SCM: 1.Sternal @ the manubrium 2. Clavicular From above: Lateral surface of the mastoid process, lateral half of the superior nuchal line of the occiput From below: Sternal Head: Anterior superior surface of the manubrium Clavicular Head: Medial 1/3-1/4 superior and posterior surfaces of the clavicle Actions: Bilaterally: Neck flexion, pulls head forward, brings chin to chest, checkrein against hyperextension, stabilizes (with trapezius) head during talking and chewing Unilaterally: Rotates the face towards the opposite side, w/traps- side bends neck. Basically, almost every movement of the neck involves help from the SCM Note: the SCM does not attach to the neck ! 13 Keys to success with the SCM: working the deep SCM. on left- sidelying > Forget working the inferior attachments. They are almost always tender and do not improve much. Plus, clients hate it and get little improvement, a lose/lose. > Do work the mastoid attachment as it can improve and can be involved with headaches. > Many MTs mistake with the SCM is not working the deep portion. they work the superficial section only. The deepest part needs the most work and is also the hardest to get to. > A pincher grip works best to go around the superficial tissues. Once you grasp the tissue, you can hold and release or work your fingers back and forth gently. In the supine position, the fingers are recommended to treat the cranial attachments at the mastoid process and lateral superior nuchal line. Sink in, then determine pressure. Moving with the skin in a line back and forth or circles is excellent In prone, thumbs are recommended. Working the mastoid attachment ! ! ! ! SCM ! Carotid Artery Internal Jugular Vein You can see from this graphic that the SCM is quite thick and wide. Also note: the neurovascular bundle resides on the posterior aspect of the SCM. Don’t pinch 360º and you’ll be fine. Hyoid muscles Two different functions of these tissues attaching to the hyoid bone ( located where the jaw/mandible meets the neck ) : Supra hyoids- meaning above the hyoid. These are the ones you use when you do a hard gulp. Massage: these we gently work the ‘floor’ of the mouth. Follow the midline and also along the line of the medical jaw, always using easy pressure and slow speeds. Infra hyoids- meaning below the hyoid bone. They depress/pull down on the hyoid. Very important in swallowing. Massage: these we will use extra gentle pressure & use light finger circles onto the thyroid cartilage, then following the muscles down to the sternum. 15 Deep anterior throat muscles. Similar is design & function as the erector spinae, but for the cervical spine. Caution: We shall not be massaging them in this class. They can be worked, but this is not recommended unless you have had very specific instruction. Longus coli This powerful cervical flexor is deep and directly attaches to the anterior of vertebrae. Longus Capitis Connects the occiput to the transverse processes of C3-6 via a ^ shape. Jobs: Flexion of head, side flexion of head. Longus coli & capitis along with the more lateral Rectus Capitis Anterior & Lateralis. Longus coli connects C1-C6 superiorly attaching closer to the midline and as it is inferiorly- moving laterally into the transverse processes of C5 & 6. Jobs: Powerful cervical flexor working bilaterally, assists in lateral flexion. Rectus Capitis Anterior & Lateralis These are two small anterior & anterior-lateral sub occipitals mirror their posterior compadres. They connect the anterior occiput & mastoid process with the transverse process of C1. Jobs: Micro movements of C1, flexion of the head, side flexion /tilting of head. Interspinous This is a series of tiny muscles that connect the inferior border of one spinous process with the superior border of the next one. Jobs: It’s main action is micro movements of the spinous processes. Massage: Tiny and hard to reach. May be worked gently with a t-bar or an add-on pencil eraser Serratus Posterior Superior This muscles hides deep to the rhomboids and under the scapula. It does connect the C7 spinous process (& T1-3) with ribs 2-5. Jobs: Assists with inspiration Massage: move scapula as much out of the way as possible. Detailed work @ spinous processes followed by glides laterally & inferiorly. Rhomboid minor Rhomboid minor does cross from the thorax into the realm of the cervicals. Connects spinous processes of C7 & T1 to the upper medical border of the scapula. Jobs: Elevate, downwardly rotate & adduct the scapula. Massage: Glides between C7 spinous process & the angle just inferior of the superior angle. 17 1. Start Gentle 2. Work without lubrication for a while 3. Soft & slow improves the flow 4. Trust your intuition. 5. Trust your hands. They will take you far. And, the more you trust them, the better you will be. 6. Let tissue rest before you work it more 7. Tell tissue what you are going to do, do it, then remind tissue what you did. AKA general, specific, general 8. Biathlon thinking: Fast works great for flow and for general strokes; slow is important for detail. Sitting down helps you shift gears, give the time you need 9. Full body w/equal time everywhere is over-rated. Feel free to skip full areas or just say hello to allow more time for more important areas. AKA: where they asked for it !! 10. Talk less, Communicate more 11. Ask 12.Practice. Practice. Practice. 13.Finish Big !