Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
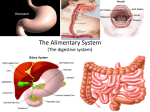
Dr .Muayad Abass Fadhel almadena copy 1 Gall bladder is a pear-shaped structure 7.5–12 cm long, with a normal capacity of about 35–50 ml almadena copy 2 The anatomical divisions are a fundus, a body and a neck that terminates in a narrow infundibulum The cystic duct is about 3 cm in length. Its lumen is usually 1–3 mm in diameter. almadena copy 3 the cystic duct joins the common hepatic duct in 80% of cases,in supradudenal portion it may extend down into the retroduodenal or even retropancreatic part of the bile duct before joining.(low insertion) the cystic duct may join the right hepatic duct or even a right hepatic sectorial duct almadena copy 4 The common hepatic duct is usually less than 2.5 cm long and is formed by the union of the right and left hepatic ducts. The common bile duct is about 7.5 cm long and is formed by the junction of the cystic and common hepatic ducts. almadena copy 5 CBD is divided into four parts: the supraduodenal portion, about 2.5 cm long, running in the free edge of the lesser omentum; • the retroduodenal portion; • the infraduodenal portion, which lies in a groove on the posterior surface of the pancreas; • the intraduodenal portion, which passes obliquely through the wall of the second part of the duodenum, where it is surrounded by the sphincter of Oddi, and terminates by opening on the summit of the ampulla of Vater. almadena copy 6 The cystic artery, a branch of the right hepatic artery. almadena copy 7 The most dangerous anomalies are where the hepatic artery takes a tortuous course on the front of the origin of the cystic duct, or the right hepatic artery is tortuous and the cystic artery short. The tortuosity is known as the ‘caterpillar turn’ or ‘Moynihan’s hump’ almadena copy 8 Lymphatics The lymphatic vessels of the gall bladder (subserosal and submucosal) drain into the cystic lymph node of Lund (the sentinel lymph node) almadena copy 9 Bile, is composed of 97% water, 1–2% bile salts and 1% pigments, cholesterol and fatty acids. The liver excretes bile at a rate estimated to be approximately 40 ml h–1. almadena copy 10 1-Reservoir for bile. During fasting, resistance to flow through the sphincter is high, and bile excreted by the liver is diverted to the gall bladder. After feeding, the resistance to flow through the sphincter of Oddi is reduced, the gall bladder contracts, and the bile enters the duodenum. These motor responses of the biliary tract are in part effected by the hormone CCK. almadena copy 11 2- concentration of bile by active absorption of water, sodium chloride and bicarbonate 5– 10 times. 3- secretion of mucus approximately 20 ml is produced per day. With total obstruction of the cystic duct in a healthy gall bladder, a mucocele developson account of this function of the mucosa of the gall bladder. almadena copy 12 Plain radiograph 1- radio-opaque gallstones in 10% of patients the centre of a stone may contain radiolucent gas in a triradiate or biradiate fissure, and this gives rise to characteristic dark shapes on a radiograph – the ‘Mercedes-Benz’ or ‘seagull’ sign. almadena copy 13 2- calcification of the gall bladder, a so called ‘porcelain’ gall bladder ,PREMALIGNANT in up to 25% of patients. SO indication for cholecystectomy. 3-Gas may be seen in the wall of the gall bladder (emphysematous cholecystitis). 4-Gas in the biliary tree may be seen after endoscopic sphincterotomy or surgical anastomosis almadena copy 14 ■ Ultrasound: stones and biliary dilatation ■ Plain radiograph: calcification ■ Magnetic resonance cholangiopancreatography: anatomy and stones ■ Multidetector row computerised tomography scan: anatomy, liver, gall bladder and pancreas cancer ■ Radioisotope scanning: function ■ Endoscopic retrograde cholangiopancreatography: anatomy, stones and biliary strictures ■ Percutaneous transhepatic cholangiography: anatomy and biliary strictures ■ Endoscopic ultrasound: anatomy and stones almadena copy 15 Ultrasonography biliary calculi, the size of the gall bladder, the thickness of the gall bladder wall, the presence of inflammation around the gall bladder, the size of the common bile duct and, occasionally, the presence of stones within the biliary tree. show a carcinoma of the pancreas occluding the common bile duct. In OBSTRUCTIVE JAUNDICE identify intra- and almadena copy 16 extrahepatic biliary dilatation and the level of obstruction. the cause of the obstruction may also be identified, almadena copy 17 Endoscopic ultrasonography : It provides accurate imaging of the common bile duct and is particularly useful in detecting stones within the bile ducts,choledocholithiasis. In addition, it has been shown to be highly accurate in diagnosing and stataging both pancreatic and periampullary cancers. almadena copy 18 Technetium-99m (99mTc)-labelled derivatives of iminodiacetic acid (HIDA, IODIDA) almadena copy 19 Oral cholecystography and intravenous cholangiography historical interest discarded replaced by more accurate imaging modalities Percutaneous transhepatic cholangiography Endoscopicretrogradecholangiopancreatograp hy almadena copy 20 Peroperative cholangiography Operative biliary endoscopy(choledochoscopy) Postoperative T-tube cholangiography almadena copy 21 Gallstones are the most common biliary pathology. 10–15% of the adult population in the USA. asymptomatic in the majority (> 80%). Approximately 1–2% of asymptomatic patients will develop symptoms requiring cholecystectomy per year, cholecystectomy one of the most common operations performed by general surgeons. almadena copy 22 three main types: cholesterol, pigment (brown/black) mixed stones. , almadena copy 23 Cholesterol or mixed stones contain 51–99% pure cholesterol plus an admixture of calcium salts, bile acids, bile pigments and phospholipids. almadena copy 24 The process of gallstone formation is complex Obesity, high-calorie diets and Certain medications can increase the secretion of cholesterol and supersaturate the bile, increasing the lithogenicity of bile. . Abnormal emptying of the gall bladder may promote the aggregation of nucleated cholesterol crystals; hence, removing gallstones without removing the gall bladder inevitably leads to gallstone recurrence. almadena copy 25 Pigment stone Less than 30% cholesterol. There are two types – black and brown. Black stones are largely composed of an insoluble bilirubin pigment polymer mixed with calcium phosphate and calcium bicarbonate. Overall, 20–30% of stones are black. Black stones accompany haemolysis, usually hereditary spherocytosis or sickle cell disease. For unclear reasons, patients with cirrhosis have a higher instance of pigmented stones. almadena copy 26 Brown pigment stones contain calcium bilirubinate, calcium palmitate and calcium stearate, as well as cholesterol. Brown stones are rare in the gall bladder. They form in the bile duct and are related to bile stasis and infected bile. almadena copy 27 Brown pigment stones are also associated with the presence of foreign bodies within the bile ducts such as endoprosthesis stents) or parasites such as Clonorchis sinensis and Ascaris lumbricoides almadena copy 28 80% asymptomatic Right upper quadrant or epigastric pain, may radiate to the back. colicky, more often is dull and constant. dyspepsia, flatulence, food intolerance, particularly to fats, some alteration in bowel frequency. almadena copy 29 Biliary colic is typically present in 10–25% of patients. This is described as a severe right upper quadrant pain that ebbs and flows for minutes to hours associated with nausea and vomiting almadena copy 30 Jaundice may result if a stone migrates from the gall bladder and obstructs the common bile duct. Rarely, a gallstone can lead to bowel obstruction (gallstone ileus). almadena copy 31 acute cholecystitis : When symptoms do not resolve, but progress to continued pain with fever and leucocytosis, almadena copy 32 In the gallbladder ■ Biliary colic ■ Acute cholecystitis ■ Chronic cholecystitis ■ Empyema of the gall bladder ■ Mucocele ■ Perforation In the bile ducts ■ Biliary obstruction ■ Acute cholangitis ■ Acute pancreatitis In the intestine ■ Intestinal obstruction (gallstone ileus) almadena copy 33 Common ■ Appendicitis ■ Perforated peptic ulcer ■ Acute pancreatitis Uncommon ■ Acute pyelonephritis ■ Myocardial infarction ■ Pneumonia – right lower lobe Ultrasound scan aids diagnosis Uncertain diagnosis – do CT scan almadena copy 34 history physical examination with confirmatory radiological studies In the acute phase, the patient may have right upper quadrant tenderness that is exacerbated during inspiration by theexaminer’s right subcostal palpation (Murphy’s sign). A positive Murphy’s sign suggests acute inflammation and may be associated with a leucocytosis and moderately elevated liver function test almadena copy 35 A mass may be palpable as the omentum walls off an inflamed gall bladder. Fortunately, in the majority of cases, this process is limited by the stone slipping back into the body of the gall bladder and the contents of the gall bladder escaping by way of the cystic duct. This achieves adequate drainage of the gall bladder and enables the inflammation to resolve. almadena copy 36 If resolution does not occur, an empyema of the gall bladder may result. The wall may become necrotic and perforate, with the development of localised peritonitis. The abscess may then perforate into the peritoneal cavity with a septic peritonitis – however, this is uncommon, because the gall bladder is usually localised by omentum around the perforation. almadena copy 37 A palpable, non-tender gall bladder (Courvoisier’s sign) . This usually results from a distal common duct obstruction secondary to a peripancreatic malignancy. Rarely, a non-tender, palpable gall bladder results from complete obstruction of the cystic duct with reabsorption of the intraluminal bile salts and secretion of uninfected mucus secreted by the gall bladder epithelium, leading to a mucocele almadena copy 38 Most authors would suggest that it is safe to observe patients with asymptomatic gallstones, with cholecystectomy only being performed for those patients who develop symptoms or complications of their gallstones. almadena copy 39 in diabetic patients, congenital haemolytic anaemia those due to undergo bariatric surgery for morbid obesity, Because increased risk of complications from gallstones. . almadena copy 40 For patients with biliary colic or cholecystitis, cholecystectomy is the treatment of choice in the absence of medical contraindications. almadena copy 41 The timing of surgery in acute cholecystitis remains controversial. early intervention, others suggest that a delayed approach is preferable almadena copy 42 Conservative treatment followed by cholecystectomy more than 90% of cases, the symptoms of acute cholecystitis subside with conservative measures. Nonoperative treatment is based on four principles: 1 Nil per mouth (NPO) and intravenous fluid administration. 2 Administration of analgesics. 3 Administration of antibiotics. As the cystic duct is blocked in most instances, the concentration of antibiotic in the serum is more important than its concentration in bile. A broadspectrum antibiotic effective against Gram-negative aerobes is most appropriate (e.g. cefazolin, cefuroxime or gentamicin). almadena copy 43 4 -Subsequent management. When the temperature, pulse and other physical signs show that the inflammation is subsiding, oral fluids are reinstated followed by regular diet. almadena copy 44 Ultrasonography is performed to ensure no local complications have developed the bile duct is of a normal size and no stones are contained in the bile duct. Cholecystectomy may be performed on the next available list, or the patient may be allowed home to return later when the inflammation has completely resolved. . almadena copy 45 Conservative treatment must be abandoned if the pain and tenderness increase; depending on the status of the patient, operative intervention and cholecystectomy should be performed If the patient has serious comorbid conditions, a percutaneous cholecystostomy can be performed under ultrasound control, which will rapidly relieve symptoms. A subsequent cholecystectomy is usually required almadena copy 46 Routine early operation some surgeons advocate urgent operation as a routine measure in cases of acute cholecystitis. Provided that : The operation is undertaken within 5–7 days of the onset of the attack, the surgeon is experienced and excellent operating facilities are available, almadena copy 47 BUT conversion rate in laparoscopic cholecystectomy is five times higher in acute than in elective surgery. If an early operation is not indicated, one should wait approximately 6 weeks for the inflammation to subside before proceeding to operate.(INTERVAL CHOLECYSTECTOMY) almadena copy 48 The gall bladder filled with pus. it may be a sequel of acute cholecystitis or the result of a mucocele becoming infected. The treatment is drainage and, later, cholecystectomy. almadena copy 49 Acute and chronic inflammation of the gall bladder can occur in the absence of stones and give rise to a clinical picture similar to calculous cholecystitis. Acute acalculous cholecystitis is seen particularly in patients recovering from major surgery (e.g. coronary artery bypass), trauma and burns. almadena copy 50 In these patients, the diagnosis is often missed, and the mortality rate is high. almadena copy 51 Preparation for operation ■ Full blood count ■ Renal profile and liver function tests ■ Prothrombin time ■ Chest X-ray and electrocardiogram (if over 45 years or medically indicated) ■ Antibiotic prophylaxis ■ Deep vein thrombosis prophylaxis Informed consent almadena copy 52 almadena copy 53 Serious complications of laparoscopic cholecystectomy fall into two major areas: access complications bile duct injuries. If either a visceral or a bile duct injury is suspected, conversion to an open technique isrecommended by most surgeons. almadena copy 54 For patients in whom a laparoscopic approach is not indicated or in whom conversion from a laparoscopic approach is required, an open cholecystectomy is performed. almadena copy 55 : • When the anatomy of the triangle of Calot is unclear, blind dissection should stop. • Bleeding adjacent to the triangle of Calot should be controlled by pressure and not by blind clipping or clamping. • When there is doubt about the anatomy, a ‘fundus-first’ or ‘retrograde’ cholecystectomy dissecting on the gall bladder wall down to the cystic duct can be helpful. almadena copy 56 • If the cystic duct is densely adherent to the common bile duct and there is the possibility of a Mirizzi syndrome (a gallstone ulcerating through into the common duct), the infundibulum of the gall bladder should be opened, the stone removed and the infundibulum oversewn. • almadena copy 57 A cholecystostomy is rarely indicated but, if necessary, stones should be extracted, and a large Foley catheter (14F) placed in the fundus of the gall bladder with a direct track externally. By so doing, should stones be left behind in the gallbladder, these can be extracted with a choledochoscope. almadena copy 58 In a situation in which sophisticated preoperative imaging or peroperative cholangiography is not available, the traditional indications for choledochotomy, which are: 1 palpable stones in the common bile duct; 2 jaundice, a history of jaundice or cholangitis; 3 a dilated common bile duct; 4 abnormal liver function tests, in particular a raised alkaline phosphatase. almadena copy 59 In 15% of patients, cholecystectomy fails to relieve the symptoms for which the operation was performed. ‘post-cholecystectomy’ syndrome. problems are usually related to the preoperative symptoms and are continuation of those symptoms. Full investigation should be undertaken to confirm the diagnosis presence of a stone in the common bile duct, a stone in the cystic duct stump or operative damage to the biliary tree. almadena copy 60 best DIAGNOSED by MRCP or ERCP. The latter has the added advantage that, if a stone is found in the common bile duct, it can be removed. almadena copy 61 almadena copy 62 almadena copy 63 almadena copy 64 almadena copy 65 almadena copy 66 almadena copy 67 almadena copy 68 almadena copy 69 almadena copy 70