Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
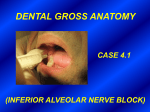
Dental Nerve Blocks Editor(s): Todd W Thomsen, MD Contributor(s): Adapted from Section Editor(s): Gary S Setnik, MD, FACEP PRE-PROCEDURE INDICATIONS Dental pain Dental trauma Incision and drainage Extensive wound care Laceration repair CONTRAINDICATIONS Allergy to local anesthetics Peripheral vascular, heart, and liver disease may increase the risk of severe complications. EQUIPMENT 3-mL Luer-lock syringe with a 1½-inch, 25- to 27-gauge needle or Monoject aspirating dental syringe (Kendall, Mansfield, Mass.) o Use a needle no smaller than 27-gauge for deep block techniques. Topical 20% benzocaine (HurriCaine, Beutlich Pharmaceuticals, Waukegan, Ill) or 5% to 10% lidocaine Cotton swabs for application of topical agents 2% lidocaine with a vasoconstrictor, such as 1:100,000 or 1:50,000 epinephrine, or other anesthetic agents with or without vasoconstrictor agents ANATOMY Maxillary nerve (V2; 2nd branch of the trigeminal nerve) o Posterior superior alveolar (PSA) nerve Supplies all the roots of the third and second molar teeth and two roots of the first molar tooth Landmarks for block: the posterolateral portion of the maxillary tuberosity and the second molar o Middle superior alveolar (MSA) nerve Supplies the maxillary first and second bicuspid teeth and the mesiobuccal root of the first molar Landmark for block: junction between the second premolar and first molar o Anterior superior alveolar (ASA) nerve Supplies the maxillary central, lateral, and cuspid teeth; the labial mucous membrane; the periosteum; and Figure 2 : Dental trauma. View Larger Image Figure 3 : Equipment. View Larger Image Figure 4 : Branches of the maxillary nerve. View Larger Image the alveoli on one side of the median line Landmark for block: the apex of the canine tooth o There is communication between the ASA, MSA, and PSA nerves. Mandibular nerve (V3; 3rd branch of the trigeminal nerve) o Supplies the lower face and temporal region, including the lower jaw and lip o Inferior alveolar nerve Descends under the external pterygoid muscle and passes between the ramus of the mandible and the sphenomandibular ligament to enter the mandibular canal, where it is accompanied by the inferior alveolar artery and vein The inferior alveolar nerve is blocked at the pterygomandibular triangle. Landmarks for this block: anterior border of the ramus of the mandible, the intraoral coronoid notch, and the occlusal plane of the molars Figure 5 : Inferior alveolar and lingual nerves. View Larger Image PROCEDURE Sample excerpt does not include step-bystep text instructions for performing this procedure Sign up for a FREE TRIAL to view full content The full content of this section includes: Step-by-step text instructions for performing the procedure Clinical pearls providing practical clinical tips from medical experts Patient safety guidelines consistent with Joint Commission and OHSA standards Links to medical evidence and related procedures Figure 10 : Deposit 1 to 2 mL of anesthetic at the apex of the tooth. View Larger Image Figure 13 : Needle entry occurs at the upper second molar. View Larger Image Figure 17 : Needle entry occurs between the second premolar and the first molar teeth. View Larger Image Figure 20 : Needle entry occurs at the apex of the canine tooth. View Larger Image Figure 23 : Palpate the anterior border of the ramus with your thumb, and retract the cheek laterally. View Larger Image Figure 24 : Proper needle trajectory. View Larger Image POST-PROCEDURE CARE Specific follow-up for the anesthetic procedure is not needed unless there is a complication. Advise the patient to not eat solid foods and to avoid hot foods or aggressive wound care until the anesthesia has worn off. o o Avoid ischemia-producing compression dressings. Advise the patient to follow up if signs of infection develop at the site of infiltration. Nerve injury is rare and most cases are transient and resolve completely. COMPLICATIONS Complications of the inferior alveolar nerve block o Temporary facial nerve paralysis Complications of the posterior superior alveolar nerve block Puncture of the pterygoid plexus and formation of a pterygoid hematoma If the needle is advanced too far posteriorly, a Division II block of cranial nerve V will result. Neuritis Intravascular injection Hematoma Infection Systemic toxicity