Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
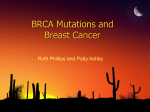
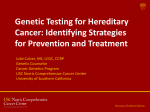
Oncocase BRCA2 gene mutation and risk of aggressive prostate cancer F. Baekelandt, MD1, W. Everaerts, MD, PhD1, M. Albersen, MD, PhD1, B. Van Cleynenbreugel, MD, PhD1, U. Milenkovic, MD1, C. Assenmacher, MD2, S. Joniau, MD, PhD1 BRCA2 mutation carriers generally present with prostate cancer at a younger age, with more aggressive disease and with a higher risk of nodal involvement or distant metastases at diagnosis. We present a patient with metastatic castrate resistant prostate cancer with a BRCA2 gene mutation and its clinical significance for daily practice. (Belg J Med Oncol 2016;10(6):223-227) Introduction The second most common cancer in men worldwide is prostate cancer (PC). Genetic background, along with lifestyle and differences in availability of PSA screening and cancer treatment, account for differences in incidence and mortality of prostate cancer.1 Breast cancer 2, early onset (BRCA2) gene is a very important gene for cancer susceptibility in men.2 Men with mutations in BRCA2 have an increased risk of PC. In BRCA2 mutation carriers the relative risk of PC is 2.5-fold to 8.6-fold before the age of 65 years.1,3 BRCA2 mutation carriers with PC present at a much younger age with more aggressive disease, are more likely to have lymph node involvement or metastatic disease at diagnosis, and have a higher mortality rate than non-mutation carriers.1,4 We present a case of metastatic castrate resistant pros- Figure 1. Choline-PET-CT image of the positive lymph node, posterior to the left external iliac artery (red arrow). 1 Department of Urology, UZ Leuven, Leuven, Belgium, 2Department of Urology, Ste-Elisabeth, Brussels, Belgium. Please send all correspondence to: S. Joniau, MD, PhD, University Hospitals Leuven, Herestraat 49, 3000 Leuven, Belgium Conflict of interest: The authors have nothing to disclose and indicate no potential conflict of interest.. Keywords: BRCA2, BRCA screening, metastatic castration resistant prostate cancer, PSA screening. Belgian Journal of Medical Oncology 223 Volume 10, Issue 6, September 2016 tate cancer (mCRPC) who was post-hoc identified as a BRCA2 mutation carrier due to BRCA screening in his family for breast cancer. We give an overview on the existing literature on BRCA2 gene mutations and discuss the clinical implications for mutation carriers and their offspring. Case report The patient was diagnosed with localised prostate cancer in 2010 at the age of 64 years. His initial PSA was 7.33 ng/ml, staging with bone scan and CT-abdomen was negative. He underwent an open radical prostatectomy elsewhere in August 2010. Pathology showed a poorly differentiated invasive adenocarcinoma of the prostate, Gleason score 4+3, with lymphovascular invasion, staged pT3aN0M0. There was a dubious surgical margin on the dorsal right side of the specimen. Three months after surgery his PSA was still 3.8 ng/ml. Choline-PET-CT showed a positive lymph node posterior to the left external iliac artery (Figure 1). Early 2011, he received adjuvant radiotherapy of the prostatic fossa (66 Gy, 33 fractions) and the pelvic nodes (52.8 Gy, 33 fractions) with concomitant goserelin for one year. In November 2012, PSA started to rise again and wholebody MRI showed a solitary bone metastasis in the vertebral body of T11 (Figure 2). He received local radiotherapy on vertebrae T10 to L2 (32 Gy, 8 fractions) and androgen deprivation therapy (ADT) was restarted (goserelin). Early 2013, bicalutamide 50 mg was associated because of a PSA rise to 9.3 ng/ml. After an initial drop in PSA levels, by late 2013 the PSA had risen again to 7.2 ng/ml. Bicalutamide was stopped for anti-androgen withdrawal effect, but the PSA rose even further to 19 ng/ml by early 2014. After adding abiraterone to goserelin, he now has a stable disease, with a PSA of 1.69 ng/ml. Calcium supplements and denosumab were added due to an osteoporotic compression fracture of L1. Recently, aged 69 years, he came to our consultation for counselling on a targeted mutation search test for BRCA gene mutations. Recent genetic screening in his family revealed a c.6270_6271delTA (p.His2090Glnfs*9) mutation in the BRCA2 gene of his niece. Two of his nieces were diagnosed with breast cancer before the age of 50 years and his father had prostate cancer. Because of his extensive medical and family history, the patient received a targeted mutation search test for the mutation found in his niece. Direct sequencing confirmed he is a mutation carrier of the c.6270_6271delTA (p.His2090Glnfs*9) in the BRCA2 gene. He was subse- Figure 2. Whole-body MRI of the solitary bone metastasis in the vertebral body of T11 (red arrow). quently counselled on the increased risk of breast and prostate cancer. His children have a 50% chance of inheriting the gene mutation. His children were offered the same targeted mutation search test. They were also advised to start screening for prostate cancer at the age of 40 years. Discussion In the last two decades, advances in the diagnosis and treatment of PC have led to improved survival. We now aim to individualise treatment according to the disease biology of each individual patient. Genome wide asso- Belgian Journal of Medical Oncology Volume 10, Issue 6, September 2016 224 6 Oncocase Table 1. Clinical trials addressing the use of poly (ADP-ribose) polymerase (PARP) in prostate cancer. Available from: https://clinicaltrials.gov, accessed May 26, 2016. 1 2 Not yet recruiting Studying the Effects of Olaparib Given to Men With Intermediate/High Risk Prostate Cancer Before Radical Prostatectomy Completed A Study Combining ABT-888, Oral PARP Inhibitor, With Temozolomide in Patients With Metastatic Prostate Cancer Interventions: Interventions: 3 4 5 7 8 Enzalutamide and Niraparib in the Treatment of Metastatic Castrate-Resistant Prostate Cancer (CRPC) Active, not recruting Ph II Study to Evaluate Olaparib With Abiraterone in Treating Metastatic Castration Resistant Prostate Cancer Active, not recruting Abiraterone Acetate and Prednisone With or Without Veliparib in Treating Patients With Metastatic Hormone-Resistant Prostate Cancer Interventions: Interventions: Drug: Enzalutamide; Drug: Niraparib Drug: Olaparib; Drug: Placebo; Drug: Abiraterone; Drug: Prednisone or prednisolone Drug: Abiraterone Acetate; Other: Laboratory Biomarker Analysis; Drug: Prednisone; Drug: Veliparib Active, not recruting Veliparib in Treating Patients With Malignant Solid Tumors That Did Not Respond to Previous Therapy Active, not recruting Study of Talazoparib, a PARP Inhibitor, in Patients With Advanced or Recurrent Solid Tumors Recruiting Phase 1 and 2 Study of MEDI4736 in Combination With Olaparib or Cediranib for Advanced Solid Tumors and Recurrent Ovarian Cancer Interventions: Interventions: Interventions: 9 Drug: ABT-888; Drug: temozolomide Active, not recruting Interventions: 6 Drug: Olaparib; Drug: Degarelix Completed Other: Laboratory Biomarker Analysis; Other: Pharmacological Study; Drug: Veliparib Drug: Talazoparib Drug: Olaparib; Drug: Cediranib; Drug: MEDI4736 A Study of MK4827 in Participants With Advanced Solid Tumors or Hematologic Malignancies (MK-4827-001 AM8) Intervention: Drug: MK-4827 ciation studies on PC have identified 70 susceptibility loci associated with the risk of developing PC, including BRCA2.4 The BRCA2 gene and its protein product play an important role in the homologous recombination repair of DNA double-strand breaks.3,5,6 A whole spectrum of BRCA2 mutations is present in 1.2% of PC patients and they are associated with a more aggressive phenotype of PC.4 Similarly, our case had a high risk, locally advanced PC (T3a, Gleason 4+3) at the time of diagnosis. Although initial staging with CT and bone scans in our case was negative, the high post-operative PSA levels indicate that the patient probably had nodal involvement or a metastasis at the time of diagnosis. It is possible that if the patient was staged with PET-CT or MRI that a positive lymph node would have been detected. This reflects what we found in the literature: PC patients with germline BRCA1/2 mutations present more frequently with Gleason ≥ 8, T3/T4 stage, lymph node involvement, and metastases at diagnosis than non-mutation carriers.4 The presence of a germline BRCA2 mutation is an independent prognostic marker for worse survival.1 A cohort study of patients treated for localised PC showed 3-, 5- and 10-year Cancer Specific Survival (CSS) rates of 99%, 97%, and 85%, respectively in non-mutation carriers, versus 96%, 76%, and 61% in BRCA mutation carriers. The Metastatic Free Survival 3, 5, and 10 years after treatment was 97%, 94%, and 84%, respectively for non-mutation carriers versus 90%, 72%, and 50%, respectively for BRCA mutation carriers.3 Our patient progressed to castration resistant status 1.5 years after starting ADT. Retrospective studies showed that BRCA1/2 mutation carriers more often develop mCRPC earlier and are more likely to receive chemo- Belgian Journal of Medical Oncology 225 Volume 10, Issue 6, September 2016 Key messages for clinical practice 1. Male BRCA2 mutation carriers have an increased risk of developing prostate cancer, breast cancer, pancreatic cancer and malignant melanoma. 2. BRCA2 mutation carriers with prostate cancer have a poorer survival outcome, present at a younger age, are more likely to have aggressive disease, nodal involvement and distant metastases at diagnosis. 3. BRCA2 mutation carriers should be screened for prostate cancer from the age of 40 years and older. 4. BRCA screening in males should be offered to: a. Patients with a significant family history of breast or ovarian cancer, preferably at young age so that early PSA screening can be started. b. P atients with prostate cancer and a close blood relative with ovarian or breast cancer < 50 y. c. Male patients with breast cancer. 5. Targeted mutation search tests should be offered to any family member of a patient with a known deleterious family BRCA1/2 mutation. 6. BRCA2 mutations are present in 20% of mCRPC tumour cells and could help in tailoring the optimal treatment. therapy.4 Whole-exome sequencing of 150 mCRPC metastases demonstrated that 19% had aberrations in DNA repair genes including BRCA1 and BRCA2.7 This can be very useful for a personalised treatment approach. Studies on breast and ovarian cancers show that mutations in homologous recombination genes such as BRCA2 are associated with a better response to compounds that induce double-strand breaks such as platinum based chemotherapy or inhibitors of poly (ADP-ribose) polymerase (PARP).3,6,8 Several studies addressing the use of PARP inhibitors in prostate cancer are ongoing (Table 1).10 A recent case series of three mCRPC patients suggest that homozygous inactivation of BRCA2 may confer sensitivity to platinum agents, which are not commonly used in PC treatment.6 Furthermore androgen receptormaintained activity has been shown to increase chromosomal instability, which means that an increased duration of ADT may possibly benefit patients with DNA repair defects, such as BRCA mutations.3 Our patient has a c.6270_6271delTA BRCA2 gene mutation. Studies suggest that BRCA2 6174delT may be associated with better outcomes than other BRCA2 mutations.4 A possible explanation for this could be that this mutation lies inside the ovarian cancer cluster region (OCCR; nucleotides 3035 to 6629) of exon 11. Mutations in this region are associated with a lower risk of PC (19.2% before the age of 80 years) than mutations outside the OCCR (33.6% before the age of 80 years).2 Several studies address the need for PSA screening in BRCA mutation carriers. BRCA2 mutation carriers have a higher incidence of clinically significant disease at a younger age when screened. The IMPACT study, addressing the utility of PSA screening and the incidence of PC in the BRCA population, showed that the positive predictive value of using a PSA threshold of 3.0 ng/ ml in BRCA2 mutation carriers is 48%, which is double of what we find in a normal population. The only cancers detected in men younger than 50 years in this study were in BRCA1/2 mutation carriers. BRCA2 mutation carriers had significantly more intermediate- or high-risk disease.1 These studies and guidelines promote the PSA screening and digital rectal examination in BRCA mutation carriers from the age of 40 years and older.2,9,11 At this moment however, there is not enough evidence to change recommendations regarding PSA Belgian Journal of Medical Oncology Volume 10, Issue 6, September 2016 226 6 Oncocase screening and biopsy in men with BRCA1/2 mutations relative to men without mutations.11 The literature addresses the issue of screening for BRCA1/2 mutations as well. Patient education and genetic counselling is of high clinical importance in every hereditary cancer.9 Despite the worse CSS in BRCA1/2 mutation carriers, it is not justified to screen unselected patients for germline BRCA mutations due to the current cost of the investigation and the low frequency in sporadic PC patients.3 National Comprehensive Cancer Network guidelines advise screening in patients with a personal history of prostate cancer (Gleason score ≥7) at any age with ≥1 close blood relative (first-, second-, and third-degree relatives on same side of family) with ovarian carcinoma at any age or breast cancer < 50 y or two relatives with breast, pancreatic or prostate cancer (Gleason score ≥7) at any age. Men with breast cancer are eligible as well.12 Targeted mutation search tests should be offered to any family member of a patient with a known deleterious family BRCA1/2 mutation.12 Besides PC, male BRCA2 mutation carriers have an increased risk of developing breast cancer, pancreatic cancer and melanoma. Although breast cancer accounts for less than 1% of all cancers in men, BCRA2 mutation carriers have a 6.9% risk of developing breast cancer before the age of 80 years. Self-examination is recommended instead of screening mammography in this population in the absence of other risk factors such as gynaecomastia.2 BRCA2 mutation carriers have a lifetime risk of pancreatic cancer of 5%. They present at a younger age and frequently lack family history of breast or ovarian cancer.2 The relative risk of developing malignant melanoma is 2.6-fold in BRCA2 mutation carriers. Annual clinical examination of the skin is recommended for this specific population.2 positive lymph nodes or distant metastases at diagnosis. Although they have a worse survival compared to non-mutation carriers, novel therapies are emerging specifically for BRCA mutated PC, with optimistic results. Screening for BRCA mutations should be offered to patients with a significant family history of breast and ovarian cancers. PSA screening is recommended in BRCA mutation carriers from the age of 40 years. References 1. Bancroft EK, Page EC, Castro E, et al. Targeted prostate cancer screening in BRCA1 and BRCA2 mutation carriers: results from the initial screening round of the IMPACT study. Eur Urol. 2014;66(3):489-99. 2. Liede A, Karlan BY, Narod SA. Cancer risks for male carriers of germline mutations in BRCA1 or BRCA2: a review of the literature. J Clin Oncol. 2004;22(4):735-42. 3. Castro E, Goh C, Leongamornlert D, et al. Effect of BRCA Mutations on Metastatic Relapse and Cause-specific Survival After Radical Treatment for Localised Prostate Cancer. Eur Urol. 2015;68(2):186-93. 4. Castro E, Goh C, Olmos D, et al. Germline BRCA mutations are associated with higher risk of nodal involvement, distant metastasis, and poor survival outcomes in prostate cancer. J Clin Oncol. 2013;31(14):1748-57. 5. Bryant HE. The Clinical Impact of BRCA2 Loss in Prostate Cancer. Eur Urol. 2015;S0302-2838(15):01217-8. 6. Cheng HH, Pritchard CC, Boyd T, et al. Biallelic Inactivation of BRCA2 in Platinum-sensitive Metastatic Castration-resistant Prostate Cancer. Eur Urol. 2015;S0302-2838(15):01177-X. 7. Robinson D, Van Allen EM, Wu YM, et al. Integrative clinical genomics of advanced prostate cancer. Cell. 2015;161(5):1215-28. 8. Mateo J, Carreira S, Sandhu S, et al. DNA-Repair Defects and Olaparib in Metastatic Prostate Cancer. N Engl J Med. 2015;373(18):1697-708. 9. Lynch HT, Kosoko-Lasaki O, Leslie SW, et al. Screening for Familial and Hereditary Prostate Cancer. Int J Cancer. 2016;138(11):2579-91. 10.ClinicalTrials.gov [Internet]. Washington. Available from: https://clinicaltrials. gov. Accessed May 26, 2016. 11. National Comprehensive Cancer Network. NCCN guidelines for detection, prevention, & risk reduction - Prostate cancer early detection (Version 2.2016). Conclusion Male BRCA2 mutation carriers have an increased risk of developing prostate cancer, breast cancer, pancreatic cancer and malignant melanoma. BRCA2 mutation carriers with PC present at a younger age, with more aggressive disease and with increased risk of having Available from: https://www.nccn.org/professionals/physician_gls/pdf/prostate_ detection.pdf. Accessed May 26, 2016. 12.National Comprehensive Cancer Network. NCCN guidelines for detection, prevention, & risk reduction - Genetic/Familial High-Risk Assessment: Breast and Ovarian (Version 2.2016). Available from: https://www.nccn.org/professionals/physician_gls/pdf/genetics_screening.pdf. Accessed May 26, 2016. Belgian Journal of Medical Oncology 227 Volume 10, Issue 6, September 2016