Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
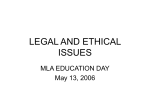
Surviving SARS, Preparing for Pandemics: Ethics, Infectious Diseases and Modern Health Care Organizations Ross E.G. Upshur, BA(HONS), MA, MD, MSc, CCFP, FRCPC Director, Joint Centre for Bioethics Canada Research Chair in Primary Care Research University of Toronto 1 6.1 Time series of respiratory ambulatory visits to primary care providers, age and gender aggregated, 1992-2002 900,000 800,000 700,000 Number of visits 600,000 500,000 400,000 300,000 200,000 100,000 Jul-02 Jan-02 Jul-01 Jan-01 Jul-00 Jan-00 Jul-99 Jan-99 Jul-98 Jan-98 Jul-97 Jan-97 Jul-96 Jan-96 Jul-95 Jan-95 Jul-94 Jan-94 Jul-93 Jan-93 Jul-92 Jan-92 0 Month/Year Note: "Respiratory ambulatory visits" include all ambulatory visits to a physician for COPD, asthma, pneumonia or repiratory infectious diseases. 2 Objectives In the aftermath of SARS and in anticipation of an influenza pandemic: Appreciate ethical principles and concepts relevant to understanding infectious disease outbreaks in modern health care organizations, Understand the complex relationship between self and other regarding acts in the care of patients with infectious diseases, Understand the silences and gaps in current codes of ethics in setting expectations for health care professionals in infectious disease outbreaks. 3 Overview of Presentation 1. 2. 3. 4. 5. The past and present context Ethics and Infectious Diseases The Challenges of the Duty to Provide Care During Infectious Disease Emergencies Preparing for the Pandemic Conclusions 4 Plague of Athens Thucydides Neither were the physicians at first of any service, ignorant as they were of the proper way to treat it, but they died themselves the most thickly, as they visited the sick most often; nor did any human art succeed any better. Supplications in the temples, divinations, and so forth were found equally futile, till the overwhelming nature of the disaster at last put a stop to them altogether. 5 6 Prayer of Separation I forbid you to ever enter a church, a monastery, a fair, a mill, a market or an assembly of people. I forbid you to leave your house unless dressed in you recognizable garb and also shod. I forbid you to wash your hands or to launder anything or to drink at any stream or fountain, unless using your own barrel or dipper. I forbid you to touch anything you buy or barter for, until it becomes your own. I forbid you to enter any tavern; and if you wish for wine, whether you buy it or it is given to you, have it funneled into your keg. I forbid you to share house with any woman but your wife. I command you, if accosted by anyone while travelling on a road, to set yourself down-wind of them before you answer. I forbid you to enter any narrow passage, lest a passerby bump into you. I forbid you, wherever you go, to touch the rim or the rope of a well without donning your gloves. I forbid you to touch any child or give them anything. I forbid you to drink or eat from any vessel but your own. 7 8 The Plague Diaries Daniel Dafoe So the plague defied all medicines; the very physicians were seized with it…men went about prescribing to others and telling them what to do…and they dropped down dead, destroyed by that very enemy they directed others to oppose. This was the case of several of the most skilful surgeons. 9 Fumigation box for treatment of syphillis 10 Ellis Island Quarantine Station 11 WHO head warns of ‘incalculable' suffering Monday, November 7, 2005 12 13 14 15 16 17 Romania 18 Why are infectious diseases important to ethics? Long time neglect of ID issues by ethicists Of historic and future significance Challenge traditional and familiar concepts (e.g. autonomy) Cross borders from personal to global ethics Universal vulnerability 19 Why have infectious diseases been neglected by ethicists? 1. 2. 3. 4. Infectious Diseases no longer considered relevant Ethics concerned with high technology The other Complexity 20 Complexity Microbiology Immunology Clinical medicine Epidemiology Zoology Geography 21 Integration of Levels of Ethical Reflection Personal Ethics Clinical Ethics Professional Ethics Organizational Ethics Public Health Ethics Global Health Ethics 22 23 24 The Duty to Care Health care workers’ duty to care, and the duty of institutions to support them 25 26 27 SARS AND HEALTH CARE WORKERS IN TORONTO 40% of probable cases in Toronto outbreak were health care workers 2 nurses and one physician died Hundreds in quarantine Psychological impact substantial 45% of nurses in one survey scored above the GHQ12 cut point for psychological stress 65% of respondents report SARS related concerns for personal or family health In aftermath many considering alternative careers 28 29 Case Mary, works in a pediatric ICU, caring for patients with serious respiratory diseases. During an outbreak of serious respiratory illness, her husband asks her to call in sick, as the mother of 3 small children she should not to risk giving them the illness. Mary feels torn between the need to protect her children, husband and self from infection & her commitment to her patients, colleagues and profession. 30 31 Nightengale Her heart it means good – for no bounty she’ll take She’d lay down her life for the poor soldier’s sake, She pray’d for the dying, gave peace to the brave, She felt that a soldier had a soul to be saved; The wounded they lov’d her, as it has been seen, She’s the soldier’s preserver they call her their queen. May God give her strength, & her heart never fail, One of heaven’s best gifts is Miss Nightingale. 32 33 Archilocus Some Saian mountaineer Struts today with my shield. I threw it down by a bush and ran When the fighting got hot. Life seemed somehow more precious. It was a beautiful shield. I know where I can buy another Exactly like it, just as round. 34 Infectious Diseases and Duty to Care: Sources of Guidance Codes of Ethics Professional Standards Virtue Ethics Contract Law Public Expectations 35 36 Do We Expect Heroism? "...when pestilence prevails, it is their (physicians') duty to face the danger, and to continue their labours for the alleviation of suffering, even at the jeopardy of their own lives". 1922 CMA Code of Ethics 2004 CMA Revision silent on the issue. Other codes of ethics from other health care professions similarly offer no direction. What about non-professional health care providers? 37 Duty to Care: Ethical Values duty to care • Principles: autonomy and beneficence • virtue ethics Reciprocity/relationality • society, institutions • necessary supports • no penalization • transparency 38 Duty not to harm others by communicating diseases. Harris and Holm BMJ 1995 The moral duty to behave responsibly and not knowingly put other people at risk is not a duty that is confined to HIV infection or to other life threatening diseases. It is a duty which all people with communicable diseases have. It is, however, also a duty which we can expect people to discharge only if they live in a community that does not leave them with all the burdens involved in discharging this duty. 39 Traditional Principles Autonomy Beneficence Non-maleficence Justice 40 Autonomy Autonomy is a form of personal liberty of action where the individual determines his or her course of action in accordance with a plan chosen by him or herself. 41 Autonomy Leslie Francis “ … Infectious disease reminds us that we are related in our vulnerability.” In the case of infectious diseases agency is not isolated but inherently relational 42 The issue of autonomy Infectious diseases challenge notions of autonomy Victim and vector 43 44 Do public expectations matter? Health professionals self-regulated Health care a public good Do we know what the public expects? 45 What standard do we wish to uphold? Supreme Samaritan Good Samaritan Minimally Decent Samaritan 46 Duty to Care: Lessons Learned health care professionals have an obligation to care for • • • • the sick themselves in order to care for the ill their families limit to personal risk is unclear 47 Duty to Care: Lessons Learned institutions have a reciprocal duty to support and protect health care workers, and to help them cope with very stressful situations need for clear expectations of employees reward, not penalization for following safe practices recognition of heroism by the public & institutions 48 49 Recommendations 1. Professional colleges and associations should provide, by way of their codes of ethics, clear guidance to members in advance of a major communicable disease outbreak, such as pandemic flu. Existing mechanisms should be identified, or means should be developed, to inform college members as to expectations and obligations regarding the duty to provide care during a communicable disease outbreak. 2. Governments and the health care sector should ensure that: a. b. 3. care providers’ safety is protected at all times, and providers are able to discharge duties and receive sufficient support throughout a period of extraordinary demands; and disability insurance and death benefits are available to staff and their families adversely affected while performing their duties. Governments and the health care sector should develop human resource strategies for communicable disease outbreaks that cover the diverse occupational roles, that are transparent in how individuals are assigned to roles in the management of an outbreak, and that are equitable with respect to the distribution of risk among individuals and occupational categories. 50 WHO Consultation How useful are these recommendations at the global level? How to manage systems that cannot assure protection to HCW’s? Does the absence of this reciprocity absolve HCW’s of their obligations to care? What about sanctions? 51 Conclusions Infectious diseases pose important challenges to traditional medical ethical frameworks Professional codes of ethics are of limited value in providing limits to risk in care for patients with infectious diseases Need for global response based on solidarity 52 Thanks to Solomon R. Benatar Mark Bernstein Abdallah S. Daar Bernard Dickens Sue MacRae Peter A. Singer Linda Wright Randi Zlotnik Shaul Tarif Bakdash Amy Haddad Shari Gruman Jennifer Gibson Alison Thompson Karen Faith Kumanan Wilson Shawn Tracy Laura Hawryluk Bob Williams Cecile Bensimon Chris McDougall Marian Adly Wayne Gold Rima Styra 53 Acknowledgements CIHR Canada Research Chair City of Toronto Public Health 54 Links Joint Centre for Bioethics Report “Stand on Guard for Thee” http://www.utoronto.ca/jcb/home/new s_pandemic.htm Ontario Pandemic Plan http://www.health.gov.on.ca/english/p roviders/program/emu/pan_flu/pan_f lu_plan.html 55 56