Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
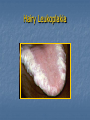
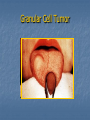
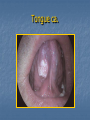
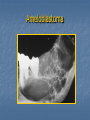
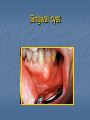
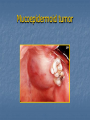
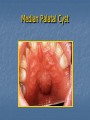
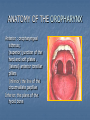
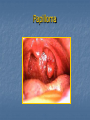
DISEASES OF THE ORAL CAVITY Prof. İlhan TOPALOĞLU Otolaryngology Department Yeditepe University School of Medicine ANATOMY OF THE ORAL CAVITY anterior : vermillion border of the lips posterior: oropharynx oropharyngeal isthmus : (superior) junction of the hard and soft plates . (lateral) anterior tonsillar pillars (inferior) the line of the circumvallate papillae ANATOMY OF THE ORAL CAVITY 1234567- Lips Anterior portion of the tongue Buccal mucosa Upper and lower alveolar ridges Retromolar trigone Floor of the mouth Hard palate Exam: Lips Exam: Lips-palpation Color, consistency Area for blocked minor salivary glands Lesions, ulcers Pyogenic granuloma Fibroma Lip cancer Lower lip carcinoma CANCERS OF THE LIP 88-98% lower lip 2-7% upper lip 0,09-6,1% oral commisure Male and older than 60 years old SCC Basal cell ca, melanoma, minör salivary gland tm. Sensory innervation of the tongue 1 – chorda tympani and lingual nerve 2 – glossopharyngeal nerve 3 – vagal nerve Motor innervation of the tongue Extrinsic muscles of the tongue are innervated by cranial nerve XII -Genioglossus -Hyoglossus -Styloglossus -Palatoglossus Intrinsic muscles of the tongue are also innervated by cranial nerve XII -Superior longutudinal -Inferior longutudinal -Vertical -Transverse Exam: Tongue Exam: Tongue You may observe lingual varicosities Exam: Tongue You may observe geographic tongue (erythema migrans) Exam: Tongue You may observe drug reaction Exam: Tongue Observe signs of nutritional deficiencies Hairy Leukoplakia Hemangioma Granular Cell Tumor Exam: Tongue You may observe cancer CANCER OF THE ANTERIOR PORTION OF THE TONGUE Tongue ca. Tongue ca. CANCERS OF TONGUE Lateral border Ocult met. 30% No supraomohyoid dissection T1- T2 surgery or RT T3- T4 surgery+RT Stage, nodal metastases, lenfovasculer, perineural invasion and thickness of tumor are important prognostic factors. Examination: Buccal Mucosa Linea alba Stenson’s duct Examination: Buccal Mucosa Lesions – white, red Lichen Planus, Leukedema CANCER OF THE BUCCAL MUCOSA Advanced stage Tm pterigoid muscles, maxilla, mandible, skin clinic N(+)RND or MRND + cheek resection There is no natural barrier T1 surgery or RT T2 surgery or RT T3 and T4 surgery+ RT Ameloblastoma Gingival cyst Malignant Melanoma Mucoepidermoid tumor CANCERS OF THE GINGIVA AND ALVEOLAR RIDGE 80 % lower gingiva and 1/3 posterior region. Incidance of mandibular invasion rate is high upper gingiva invasion of maksillary sinus Pull out the tooth invasion of bone marrow uncommon Lower jaw ( posterior 1/3 dental arch) Marginal mandibular resection Stage 1-2 , surgery Stage 3-4 ,surgery+ (+) neck MRND (-) Neck Rtx Exam: Retromolar trigone Exam: Retromolar trigone Edentulous RETROMOLAR TRİGONE CA Uncommon Invasion of mandible Late diagnose , advanced stage, cervical metastases are bad prognostic factors T1 T2 surgery or RT T3 T4 surgery + RT Exam: Floor of mouth Visualize, palpate - bimanually Wharton’s duct Must dry to observe Does “lesion” wipe off? Where are the two most likely areas for oral cancer? lateral border of the tongue Floor of mouth Exam: Floor of mouth Palpation of the floor of the mouth Exam: Floor of mouth Squamous Cell Carcinoma Squamous Cell Carcinoma FLOOR OF THE MOUTH CA. Incidance of mandibular invasion rate is high Ocult met 10-30% Primary resection of the floor of the mouth is peformed with ipsilateral or bilateral neck dissection (if the tumor is located at the midline) Exam: Hard palate Minor salivary glands Median Palatal Cyst CANCER OF THE HARD PALATE uncommon SCC and Adenoid cystic ca Misdiagnosed as maxillary sinus tm Incidance of neck metastases is low Elective neck treatment is unnecessary Prostodontist ORAL PREMALİGNANCY Leukoplakia Erythroplakia Mucosal atrophy MALIGNANT LESIONS SQUAMOUS CELL CARCINOMA VERRUCOUS CARCINOMA MINOR SALIVARY GLAND TUMOURS SARCOMATOID CARCINOMAS MALIGNANT MELANOMA PATIENT EVALUATION Diagnosis Neoplasms of the oral cavity Complete head and neck examination Chest x-ray and liver function tests plus additional laboratory tests dictated by patient’s medical history CT/MRI scan for extent of primary and possible cervical nodal evaluation Dental evaluation Radiotherapy evaluation Staging endoscopy and biopsy ETIOLOGY Risk factors for oral cavity and oropharyngeal cancer include: Cigarette Alcohol Exposure to the human papilloma virus (HPV) or Epstein-Barr virus (EBV) ionizing radiation Prolonged sun exposure, especially linked to cancer in the lip area and skin cancer. Fair skin, also linked to lip cancer and skin cancer. Age. People over the age of 45 years old are at increased risk for oral cancers (though it can develop in people of any age). Poor nutrition. Irritation from poorly fitting dentures in people who use alcohol and tobacco products. Chewing betel nuts, a nut containing a mild stimulant popular in Asia. Weakened immune system. Vitamin A deficiency. A rare condition called PlummerVinson Syndrome, which involves iron deficiency and causes difficulty swallowing. Gender. Men are more likely to get lip cancer than women. lichen planus discoid lupus erythematosus dystrophic epidermolysis bullosa Symptoms Otalgia Odynofagia Bleeding Dysfagia Loss of teeth Restriction of mouth movement Trismus EPIDEMIOLOGY 95 % SCC 95 % patiet 40 years old Mean age 60 years old After the treatment of oral cavity ca if the patient doesn’t give up smoking, second primary or recurrence rate is 40 % CARCINOGENESIS tobacco ionizing radiation dental travma and poor oral hygiene alcohol tertiary syphilis human papilloma virus candida albicans some nutritional factors oral submucous fibrosis lichen planus discoid lupus erythematosus dystrophic epidermolysis bullosa dyskeratosis congenita TREATMENT surgery RT surgery + RT KT + RT Surgery + RT + adjuvant KT The last cigarette DISEASES OF OROPHARYNX Prof. Dr. İlhan TOPALOĞLU Otolaryngology Department Yeditepe University School of Medicine ANATOMY OF THE OROPHARYNX Anterior : oropharyngeal isthmus; (superior) junction of the hard and soft plates . (lateral) anterior tonsillar pillars (inferior) the line of the circumvallate papillae İnferior: the plane of the hyoid bone OROPHARYNX SUBSIDES Soft palate and uvula Base of the tongue Tonsillar region (tonsillar fossae and pillars) Oropharyngeal walls (lateral and posterior) Diseases of the Tonsils & Adenoid Waldeyer's ring Waldeyer's tonsillar ring (or pharyngeal lymphoid ring) is an anatomical term describing the lymphoid tissue ring located in the pharynx and to the back of the oral cavity. It was named after the nineteenth century German anatomist Heinrich Wilhelm Gottfried von Waldeyer-Hartz. Waldeyer's ring Pharyngeal tonsil (also known as 'adenoids' when infected) Tubal tonsil (where Eustachian tube opens in the nasopharynx) Palatine tonsils (commonly called "the tonsils" in the vernacular, less commonly termed "faucial tonsils") Lingual tonsils Anatomy Tonsils Between arcus palatoglossus (ant plica) and arcus palatofaryngeus (post plica) Adenoids Blood Supply Tonsils Ascending and descending palatine arteries Tonsillar artery 1% aberrant ICA just deep to superior constrictor Adenoids Ascending pharyngeal, sphenopalatine arteries Histology Tonsils Specialized squamous Extrafollicular Mantle zone Germinal center Adenoids Ciliated pseudostratified columnar Stratified squamous Transitional Common Diseases of the Tonsils and Adenoids Acute adenoiditis/tonsillitis Recurrent/chronic adenoiditis/tonsillitis Obstructive hyperplasia Malignancy Acute Adenotonsillitis Etiology 5-30% bacterial; of these 39% are beta-lactamaseproducing (BLPO) Streptococcus pyogenes (Group A beta-hemolytic streptococcus GABHS most important pathogen because of potential sequelae Microbiology of Adenotonsillitis Most common organisms cultured from patients with chronic tonsillar disease (recurrent/chronic infection, hyperplasia): Streptococcus pyogenes (Group A betahemolytic streptococcus) H.influenza S. aureus Streptococcus pneumoniae Acute Adenotonsillitis Differential diagnosis Infectious mononucleosis Malignancy: lymphoma, leukemia, carcinoma Diptheria Scarlet fever Agranulocytosis Medical Management PCN is first line, even if throat culture is negative for GABHS Antibiotics aimed against BLPO and anaerobes For acute UAO: IV abx, NP airway, steroids, and immediate tonsillectomy for poor response Obstructive Hyperplasia Adenotonsillar hypertrophy most common cause of SDB in children Diagnosis Indications for polysomnography Interpretation of polysomnography Perioperative considerations Unilateral Tonsillar Enlargement Apparent enlargement vs true enlargement Non-neoplastic: Acute infective Chronic infective Hypertrophy Congenital Neoplastic Peritonsillar Abscess ICA Aneurysm Pleomorphic Adenoma Toncil ca. Papilloma Other Tonsillar Pathology Hyperkeratosis, mycosis leptothrica Tonsilloliths Candidiasis Syphilis Retention Cysts Supratonsillar Cleft Indications for Tonsillectomy Paradise study Frequency criteria: 7 episodes in 1 year or 5 episodes/year for 2 years or 3 episodes/year for 3 years Clinical features (one or more): T 38.3, cervical LAD (>2cm) or tender LAD; tonsillar/pharyngeal exudate; positive culture for GABHS; antibiotic treatment Indications for Tonsillectomy AAO-HNS: 3 or more episodes/year Hypertrophy causing malocclusion, UAO Halitosis, not responsive to medical therapy UTE, suspicious for malignancy Individual considerations Indications for Adenoidectomy Paradise study (1984) 28-35% fewer acute episodes of OM with adenoidectomy in kids with previous tube placement Adenoidectomy or T & A not indicated in children with recurrent OM who had not undergone previous tube placement Gates et al (1994) Recommend adenoidectomy with M & T as the initial surgical treatment for children with MEE > 90 days and CHL > 20 dB Indications for Adenoidectomy Obstruction: Chronic nasal obstruction or obligate mouth breathing OSA with FTT, cor pulmonale Dysphagia Speech problems Severe orofacial/dental abnormalities Infection: Recurrent/chronic adenoiditis (3 or more episodes/year) Recurrent/chronic OME (+/- previous BMT) PreOp Evaluation of Adenoid Disease Triad of hyponasality, snoring, and mouth breathing Rhinorrhea, nocturnal cough, post nasal drip “Adenoid facies” “Milkman” & “Micky Mouse” Overbite, long face, crowded incisors PreOp Evaluation of Adenoid Disease Evaluate palate Symptoms/FH of CP or VPI Midline diastasis of muscles, bifid uvula CNS or neuromuscular disease Preexisting speech disorder? PreOp Evaluation of Adenoid Disease Lateral neck films are useful only when history and physical exam are not in agreement. Accuracy of lateral neck films is dependent on proper positioning and patient PreOp Evaluation of Tonsillar Disease History Documentation of episodes by physician Cor pulmonale Poststreptococcal GN Rheumatic fever PreOp Evaluation of Tonsillar Disease TONSIL SIZE 0 in fossa +1 <25% occupation of oropharynx +2 25-50% +3 50-75% +4 >75% Avoid gagging the patient PreOp Evaluation for Adenotonsillar Disease Coagulation disorders Historical screening CBC, PT/PTT, BT, vWF activity Hematology consult von Willebrand’s disease ITP Sickle cell anemia Principles of Surgical Management Numerous techniques: Guillotine Tonsillotome Beck’s snare Dissection with snare (Scissor dissection, Fisher’s knife dissection, Finger dissection Electrodissection Laser dissection (CO2, KTP) … Surgeon’s preference Post Operative Managment Criteria for Overnight Observation Poor oral intake, vomiting, hemorrhage Age < 3 Home > 45 minutes away Poor socioeconomic condition Comorbid medical problems Surgery for OSA or PTA Abnormal coagulation values (+/- identified disorder) in patient or family member Complications #1 Postoperative bleeding Other: Sore throat, otalgia, uvular swelling Respiratory compromise Dehydration Burns and iatrogenic trauma Rare Complications Velopharyngeal Insufficiency Nasopharyngeal stenosis Atlantoaxial subluxation/ Grisel’s syndrome Regrowth Eustachian tube injury Depression Laceration of ICA/ pseudoaneursym of ICA Toncil ca. TONCIL CA 75-80% of oropharyngeal cancer İncidance of lymphatic metastases rate is high 75% (mostly jugulodigastric met.) T1 – T2 RT N2 – N3 surgery + RT T3 – T4 surgery + RT