Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
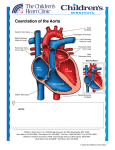
Asymptomatic coarctation in an adult female – A case report Key wards: Coarctation, Balloon angioplasty,Hypertension, Congenital malformation Abstract Coarctation of the aorta is typically a disease of childhood and early adulthood, and there is a reduced life expectancy in patients who have not undergone correction. Survival to older age is rare, due to severe cardiovascular complications. We describe the case of a woman first diagnosed with coarctation of aorta at adult age. Introduction Coarctation of the aorta accounts for 5%–10% of congenital heart disease and occurs more frequently in males. It is usually diagnosed during childhood by routine examination of blood pressure and femoral pulse palpation. We describe the case of a woman first diagnosed with coarctation of aorta at an adult age. We present this case to highlight the importance of systematic clinical examination while evaluating patients with hypertension. Case Report We report a case of asymptomatic coarctation of aorta in a young female presented to our Medical clinic. Medline search did not reveal any case reported from United Arab Emitates. A 26 year old female was referred from Primary care centre to our medical clinic for management of hypertension. She presented to primary care centre with abscess of the axilla and was found to be hypertensive. She did not have any other symptoms. Clinical examination showed moderately built young lady. Blood Pressure was 166/93 both upper limbs. Upper limbs pulses were felt normally. However, lower limb pulses including femorals were not felt. There was no femoral or renal bruit. There was 2/6 systolic murmur heard below the left clavicle which radiates to left infrascapular region. In view of these clinical findings, aortic coarctation was suspected Investigations: Results of renal functions and urinalysis were normal. ECG showed left ventricular hypertrophy with strain pattern. Chest x-ray showed bilateral rib notching (Figure 1). Chest X-ray demonstrates the rib notching bilaterally due to the dilated collaterals. CT angiography of the thorax revealed aortic coarctation of the descending segment below the level of subclavian artery (Figure 2 and 3). ECT Axial cuts at the level of Aortic coarctation Axial Enhanced CT demonstrates the Aortic coarctation with the post stenotic dilatation. Dilated collaterals were also seen (Figure 4). Axial enhanced CT images at the level of the internal mammary vessels showing dilated internal mammary and para vertebral collaterals. She was started on betablocker and referred to cardiology department for echocardiogram and further evaluation. Echocardiogram showed tight coarctation of aorta with a gradient of 50 mm Hg. Echocardiogram also revealed bicuspid aortic valve. Cardiac catheterization with possible stent implantation was advised. Discussion Coarctation of aorta is a congenital malformation that usually presents early in life. Coarctation of the aorta occurs in 6-8% of patients with congenital heart disease. (1, 2) The male-to-female ratio is 2:1, although this ratio is not valid in abdominal coarctation of the aorta, in which this rare lesion predominantly affects females. No definitive racial differences have been documented in coarctation of the aorta, although some authors have suggested that coarctation of the aorta is less common in Asians. (3) Generally, patients with coarctation of the aorta present early in life with CHF or later in life with hypertension. Many patients are asymptomatic except for the incidentally noted hypertension.Studies continue to document that coarctation of the aorta is often missed in the first year of life, (4,5)and the median age of referral to a pediatric cardiologist in one study was 5 years. Among 2192 patients reported to the Pediatric Cardiac Care from 1985-1993, 1337 were infants, 824 were children, and 31 were adults. (6) Palpation of femoral pulses and measurement of blood pressure during routine examination is necessary to avoid a delay in the diagnosis. The mean survival for untreated patients is 35 years with a 25% survival rate beyond 50 years. The natural history of unrepaired coarctation of the aorta includes the development of systemic hypertension and subsequent morbidity and death from cardiovascular disease (7). The age at correction is the most important factor for the relief of hypertension and long-term survival (8). Coarctation of the aorta is a constricted aortic segment .The classic coarctation of the aorta is located in the thoracic aorta distal to the origin of the left subclavian artery. Rarely, a coarcted segment is present in the lower thoracic or abdominal aorta. The localized constriction may form a shelf like structure with an eccentric opening or may be a membranous curtain like structure with a central or eccentric opening. The coarctation may be discrete, or a long segment of the aorta may be narrowed; the former is more common. Dilatation of the descending aorta immediately distal to the coarctation segment (post-stenotic dilatation) is usually present. Collateral vessels that connect arteries from the upper part of the body to the vessels below the level of coarctation may be seen; these may be present as early as a few weeks to a few months of life. The most commonly associated clinically significant defects include patent ductus arteriosus, VSD, and aortic stenosis. Mitral valve anomalies, although less common than those of the aortic valve, are also associated with coarctation of the aorta. Numerous theories have been proposed for the etiology of coarctation of the aorta, including postnatal ductal constriction,(9,10) translocation of ductal tissue on to the aorta, (11, 12) and a theory that alterations in intrauterine blood flow cause altered flow through the aortic arch and result in the substrate for coarctation. Coarctation of the aorta manifests when the ductus closes starting at the pulmonary end, with gradual involution of ductal tissue toward the aorta. Similar to most forms of congenital heart disease (CHD), the etiology of coarctation of the aorta may be explained by multifactorial inheritance hypothesis. The prevalence of coarctation of the aorta in genetic abnormalities such as Turner syndrome (45X), is as high as 15-20%. Investigations Radiography in patients with early onset of coarctation of the aorta may reveal cardiomegaly, pulmonary edema, and other signs of congestive heart failure. Radiography in patients with late onset of coarctation of the aorta may reveal cardiomegaly. Rib notching secondary to collateral vessels may also be seen. Echocardiography: Echocardiography delineates intracardiac anatomy and allows assessment of associated significant intracardiac anomalies. The suprasternal notch 2-dimensional echocardiographic view allows evaluation of the aortic arch to assess the transverse aortic arch, isthmus, and severity of coarctation. Doppler echocardiography is used to measure the gradient at the site of coarctation and to identify the pattern of diastolic runoff typically seen in patients with severe obstruction. MRI and CT are useful in older or postoperative patients to assess residual arch obstruction, arch hypoplasia, or formation of aneurysms. (13, 14) Cardiac catheterization: Cardiac catheterization and selective cineangiography may not be required for diagnosis; however, they allow evaluation of the severity of coarctation, anatomic nature of the aortic obstruction (discrete vs. long segment), and arch anatomy, including hypoplasia of the transverse arch or isthmus. Cardiac catheterization helps confirm the diagnosis when echocardiography findings are not completely clear. Cardiac catheterization allows the evaluation of intracardiac anatomy and the contribution of associated lesions to the overall hemodynamic disturbance. Cardiac catheterization is a prerequisite for intervention in the form of either balloon angioplasty or stent implantation in native or recurrent coarctation. When catheterization is performed, elevations of left ventricular and ascending aortic peak systolic pressures with a peak-to-peak systolic pressure gradient across the coarcted segment are usually found. A peak-to-peak gradient in excess of 20 mm Hg is generally considered indicative of significant obstruction. However, the magnitude of the gradient is not necessarily indicative of the degree of narrowing because the gradient depends on not only the extent of aortic narrowing but also the size and number of collateral vessels. Treatment: Early presentation of coarctation of the aorta: Treatment in patients with congestive heart failure includes the use of diuretics and inotropic drugs. Prostaglandin E1 (0.05-0.15 mcg/kg/min) is infused intravenously to open the ductus arteriosus. If the coarctation has a significantly adverse effect on the physiology of the associated defects, and consequently the clinical status, the coarctation should be initially relieved with surgery or balloon angioplasty and the patient reassessed with regard to need for intervention for the associated defects. Late presentation of coarctation of the aorta Treatment of hypertension: Preoperative hypertension can be effectively treated using betablockers. Significant hypertension or congestive heart failure is an indication for intervention. Surgical relief of the aortic obstruction and catheter interventional techniques (balloon angioplasty and stents) are available alternatives. Symptomatic neonates and infants should undergo urgent intervention soon after the infant is stabilized. Asymptomatic infants, children, adolescents, and adults should undergo the procedure electively. If neither hypertension nor heart failure is present, elective surgical or balloon therapy in children aged 2-5 years is suggested. Waiting beyond age 5 years for surgery or balloon therapy to relieve aortic obstruction is not advisable because of the evidence of residual hypertension if intervention is performed after age 5 years. (15) Since the introduction of surgical correction by Crafoord and Nylin (1945) and by Gross and Hufnagel (1945) in the early 1940s, surgical therapy has been the preferred treatment for aortic coarctation. Various surgical techniques have been used to treat patients with coarctation of the aorta, namely, resection and end-to-end anastomosis, patch aortoplasty, left subclavian flap aortoplasty, and tubular bypass grafts. The techniques are occasionally combined or modified to fit the individual patient's anatomy. (16) In most centers, associated defects may be addressed at the time of surgery for coarctation by proceeding with a median sternotomy to repair lesions. Some groups of workers consider balloon angioplasty the initial therapy of choice and reserve surgical intervention for the following coarctations: Coarctations that involve the long segment of the aorta Coarctations that are completely or almost completely occluded so that no catheter or guide wire can be passed across the coarcted segment Coarctations that is associated with a large patent ductus arteriosus and ventricular septal defect that requires prompt surgical intervention for the primary cardiac problem. Surgery compared with balloon therapy: Based on reviews, the effectiveness of balloon angioplasty appears to be comparable with that of surgery; the mortality rates are similar and are probably related to the associated cardiac defects, not related to type of intervention performed), and morbidity and complication rates are lower with balloon angioplasty than with surgical therapy. Balloon angioplasty may be an effective alternative to surgery for the relief of aortic coarctation. (17, 18) Summary of treatment: At initial presentation, if cardiac failure or hypertension is the presenting problem, it should be addressed to stabilize the patient. Subsequently, the aortic obstruction should be relieved. The available options include surgical and catheter interventional procedures; the latter procedures include balloon angioplasty and bare or covered stents. In general, surgical intervention in neonates and young infants (extremely ill babies with poor left ventricular function may benefit from balloon angioplasty), balloon angioplasty in children, and stent deployment in adolescents and adults appear to be appropriate options. Of course, the anatomy of the coarcted aortic segment and the aortic arch would greatly influence the method of therapy in a given patient. Follow up Assess postoperative BP response to exercise prior to discontinuation of antihypertensive therapy. Many patients may be weaned from antihypertensive therapy over months or years following repair of coarctation. Other patients may require some form of ongoing antihypertensive therapy. Search for late complications of coarctation repair, including recurrent coarctation and aneurysm formation. Patients should receive antibiotic prophylaxis before undergoing any bacteremia-producing surgery or procedures, especially in view of reported incidence of bacterial endocarditis during follow-up. (19) References: 1. Nadas, AS, Fyler DC. Pediatric Cardiology. 3rd Ed. Philadelphia, PA: Saunders; 1972:p. 683. 2. Keith JD, Rowe RD, Vlad P. Heart Disease in Infancy and Childhood. 3rd Ed. New York, NY: Macmillan; 1978:pp. 4-6. 3. Rao PS. Balloon angioplasty of native aortic coarctation. J Am Coll Cardiol. Sep 1992;20(3):750-1. [Medline]. 4. Strafford MA, Griffiths SP, Gersony WM. Coarctation of the aorta: a study in delayed detection. Pediatrics. Feb 1982;69(2):159-63. 5. Thoele DG, Muster AJ, Paul MH. Recognition of coarctation of the aorta. A continuing challenge for the primary care physician. Am J Dis Child. Nov 1987;141(11):1201-4. [Medline]. 6. Norton JB Jr. Coarctation of the Aorta. In: Moller JH, ed. Surgery of Congenital Heart Disease: Pediatric Cardiac Care Consortium. Armonk, NY: Futura Publishing Co; 19841995.:143-57. 7. M. Campbell, “Natural history of coarctation of the aorta,” British Heart Journal, vol. 32, no. 5, pp. 633–640, 1970. 8. R. M. H. J. Brouwer, M. E. Erasmus, T. Ebels, and A. Eijgelaar, “Influence of age on survival, late hypertension, and recoarctation in elective aortic coarctation repair: including long-term results after elective aortic coarctation repair with a follow-up from 25 to 44 years,” Journal of Thoracic and Cardiovascular Surgery, vol. 108, no. 3, pp. 525– 531, 1994 9. Rudolph AM, Heymann MA, Spitznas U. Hemodynamic considerations in the development of narrowing of the aorta. Am J Cardiol. Oct 1972;30(5):514-25. [Medline]. 10. Talner NS, Berman MA. Postnatal development of obstruction in coarctation of the aorta: role of the ductus arteriosus. Pediatrics. Oct 1975;56(4):562-9. [Medline]. 11. Cassels DE. The Ductus Arteriosus. Springfield, IL,: Charles C. Thomas; 1973:161. 12. Skoda J. Demonstration eines Falles Ven Obliteration de Aorta. Wochenblatt Zeischrift de kaiserlichen-Konighiche Gesellschaft der Aerttze Zur Wien. 1995;1:710-720. 13. Mohiaddin RH, Kilner PJ, Rees S, Longmore DB. Magnetic resonance volume flow and jet velocity mapping in aortic coarctation. J Am Coll Cardiol. Nov 1 1993;22(5):1515-21. [Medline]. 14. Pitlick PT, Anthony CL, Moore P, Shifrin RY, Rubin GD. Three-dimensional visualization of recurrent coarctation of the aorta by electron-beam tomography and MRI. Circulation. Jun 15 1999;99(23):3086-7. [Medline]. 15. Liberthson RR, Pennington DG, Jacobs ML, Daggett WM. Coarctation of the aorta: review of 234 patients and clarification of management problems. Am J Cardiol. Apr 1979;43(4):835-40. [Medline]. 16. Lacour-Gayet F, Bruniaux J, Serraf A, Chambran P, Blaysat G, Losay J. Hypoplastic transverse arch and coarctation in neonates. Surgical reconstruction of the aortic arch: a study of sixty-six patients. J Thorac Cardiovasc Surg. Dec 1990;100(6):808-16. [Medline]. 17. Rao PS, Chopra PS. Role of balloon angioplasty in the treatment of aortic coarctation. Ann Thorac Surg. Sep 1991;52(3):621-31. [Medline]. 18. Rao PS. Neurologic complications following balloon angioplasty. Pediat Cardiol. 1993;14:63-4. 19. Morris CD, Reller MD, Menashe VD. Thirty-year incidence of infective endocarditis after surgery for congenital heart defect. JAMA. Feb 25 1998;279(8):599-603. [Medline].