Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
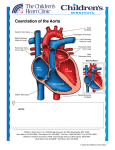
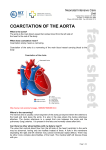
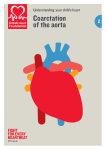
奇美醫學中心胸腔內,外,放射科臨床病例綜合討論會 題目:胸腔影像綜合討論會:Coarctation of aorta 聯絡人: 鄭舒帆 主持人:謝俊民 時間:106 年 06 月 06 日 PM 4:00 地點:奇美醫學中心 9 樓空橋討論室 摘要: Introduction: Coarctation of the aorta (CoA) is a relatively common defect that accounts for 5-8% of all congenital heart defects. CoA may occur as an isolated defect or in association with various other lesions, most commonly bicuspid aortic valve and ventricular septal defect (VSD). The diagnosis of CoA may be missed unless an index of suspicion is maintained, and diagnosis is often delayed until the patient develops congestive heart failure (CHF), which is common in infants, or hypertension, which is common in older children. This article discusses the pathology, pathophysiology, clinical features, noninvasive and invasive evaluation, and therapy in patients with CoA. CoA may be defined as a constricted aortic segment that comprises localized medial thickening with some infolding of the medial and superimposed neointimal tissue. The localized constriction may form a shelflike structure with an eccentric opening or may be a membranous curtainlike structure with a central or eccentric opening. The coarctation may be discrete, or a long segment of the aorta may be narrowed; the former is more common. In the past, CoA has been described as preductal (or infantile) type or postductal (or adult) type, depending on whether the coarctation segment is proximal or distal to the ductus arteriosus, respectively. However, a closer examination of the anatomy suggests that all coarctations are juxtaductal. The classic CoA is located in the thoracic aorta distal to the origin of the left subclavian artery at about the level of the ductal structure. However, rarely, a coarcted segment is present in the lower thoracic or abdominal aorta. In such instances, the coarcted segment may be long and fusiform with irregular lumen; many consider these to be inflammatory or autoimmune in origin, and they may be variants of Takayasu arteritis. Chest radiographic findings: Radiography in patients with early onset of coarctation of the aorta (CoA) may reveal cardiomegaly, pulmonary edema, and other signs of CHF. Radiography in patients with late onset of CoA may reveal cardiomegaly. An inverted “3” sign of the barium-filled esophagus or a “3” sign on a highly penetrated chest radiograph (frontal view) may be visualized. Rib notching secondary to collateral vessels may also be seen. Computed tomographic findings: MRI and CT are useful in older or postoperative patients to assess residual arch obstruction, arch hypoplasia, or formation of aneurysms. Ultrafast CT scan is preferable if multiple surgical clips or a stent is present in the area of coarctation. Dilatation of the descending aorta immediately distal to the coarctation segment (poststenotic dilatation) is usually present. A jet lesion on the wall of the aorta distal to the coarctation site may also be present. Varying degrees of hypoplasia of the isthmus of the aorta (the portion of the aorta between the origin of the left subclavian artery and ductus arteriosus) are present in most patients with thoracic coarctation; this hypoplasia may be significant in symptomatic coarctation of the neonate and infant, while, in children and adults, the isthmus may have only mild narrowing. The transverse aortic arch (the arch between the origin of the right innominate artery and the left subclavian artery) is also hypoplastic in symptomatic neonates and infants. Collateral vessels that connect arteries from the upper part of the body to the vessels below the level of coarctation may be seen; these may be present as early as a few weeks to a few months of life. The most commonly associated clinically significant defects include patent ductus arteriosus, ventricular septal defect, and aortic stenosis. The earlier the infant presents, the more likely a significant associated defect is present. Bicuspid aortic valve may be seen in nearly two thirds of infants with CoA, while only 30% of those infants have an older sibling with such an anomaly. Mitral valve anomalies, although less common than those of the aortic valve, are also associated with CoA. Sometimes, CoA is a complicating feature of a more complex cyanotic heart defect, such as transposition of the great arteries, Taussig-Bing anomaly, double-inlet left ventricle, tricuspid atresia with transposition of the great arteries, and hypoplastic left heart syndrome. Aortic coarctation is extremely rare in patients with severe right ventricular outflow tract obstructions such as tetralogy of Fallot and pulmonary atresia with intact ventricular septum. Some patients with CoA may have cerebral aneurysms, predisposing them to cerebrovascular accidents with severe hypertension later in life. CoA is the most common cardiac defect associated with Turner syndrome.