Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
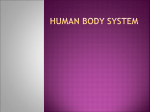
Module Title: Obstetric and Gynecologic Emergencies Module Code: HEO321T Unit Title: Introduction of Obstetric and Gynecology HEO321T- 1 Emergency Nursing Program Khan Younis Training Centre – KYTC Department of Education, Gaza Field Office, UNRWA Contents: 1.1 Anatomy of the Male Reproductive System 1.1.1 Testes 1.1.2 The Genital Ducts 1.1.3 Accessory Reproductive Glands 1.1.4 Supporting Structures 1.2 Anatomy of the female Reproductive System 1.2.1 Female pelvis 1.2.2Ovaries 1.2.3 Uterus 1.2.4 Uterine tube 1.2.5 Vagina 1.2.6 Uvula 1.2.7 Breast 1.3 Female reproductive cycles 1.4 Physiological changes in the reproductive system 1.5 Minor disorder of pregnancy 1.6 Antenatal care of pregnancy 1 1.1 Anatomy of the Male Reproductive System The importance of the reproductive system is the production of off spring & continued existence of the genetic code. The male reproductive system, like that of the female, consists of those organs functioning to produce a new individual. The male organs are specialized to produce and maintain the male sex cells, or sperm; to transport them, along with supporting fluids, to the female reproductive system; and to secret the male hormone testosterone. The Male reproductive organs include the two testes (Where the sperm cells and testosterone are made), the penis, the scrotum, and the Accessory organ (epididymis, vas deferens, seminal vesicles, ejaculatory duct, urethra, bulbourethral glands, and prostate gland). Figure 1.1: Male reproductive organs; Sagittal section of pelvis showing placement of male reproductive organs. 2 1.1.1 Testes They are located in the scrotum; one testis in each of the two scrotal compartments. The left testis is lower than the right one. Each testis is composed of several lobules which contain many seminiferous tubules and interstitial cells. Seminiferous tubules in testis open into a series of efferent ductules that emerge from the top of the organ & enter the head of epididymis. Figure 1.2: Tubules of the testis and epididymis. The functions of testes are: Spermato genesis which is formation of mature male gametes by seminiferous tubules. 1.1.2 Secretion of hormone (testosterone) by interstitial cells. The genital Ducts 3 Epididymis: Each one is formed of a single, coiled tube enclosed in a fibrous tissue. It lies along the top of testis & behind it. It forms comma shape. It's divided into head, body & tail, which is continuous with the vas deference. Functions: It is one of the ducts systems. Maturation of the sperm which stays 1-3 weeks in this segment. Secretion of a small part of the seminal fluid. Vas deferens: It's the extension of the tail of the epididymis. It passes up in the inguinal canal to the top of the urinary bladder, to join the ampulla of the seminal duct, forming the ejaculatory duct. Function: Ductal system connects the epididymis with ejaculatory duct. The storage time is about 30 days & the sperm will not loose their fertility power. Ejaculatory duct: Both ducts are short tubes. Pass through the prostate gland to terminate in urethra and they carry the spermatozoa and the seminal fluid. 4 Urethra: is a tube for micturation & semen secretion. 1.1.3 Each is formed of the union of vas deferens & seminal vesicle. Accessory Reproductive Glands Seminal vesicles: They are convoluted pouches, lies along the lower part of the posterior surface of the bladder, directly in front of the rectum. Functions: Secretion of an alkaline viscous liquid component of the semen. It contains fructose which is considered an energy source for sperm motility after ejaculation. Its secretion also contains prostaglandins. Prostate gland: It's a compound tubuloalveolar gland. It lies just below the bladder. The urethra passes in the centre of the gland. Functions: It secretes a thin alkaline substance that constitutes bout 30% of the seminal fluid. Its alkalinity protects the sperm from the acidity of the male urethra & female vagina. 5 Bulbourethral glands: Cowper's glands are small pease in size & shape. They are just below the prostate and around the penile part of urethra. Functions: 1.1.4 Secretion of an alkaline fluid. Secretion of mucous which is lubricant for urethra. Supporting Structure Scrotum: It's a pouch covered by skin. Scrotum has a dartos muscles which causes wrinkling of the scrotal pouch with slight elevation of the testis. The main function of the scrotum is to provide the optimum temperature for testes for proper spermatogenesis; it's about 3° c below normal body temperature. Penis: It's formed of 3 cylindrical masses of erectile or cavernous tissue, enclosed in separate fibrous covering of skin. The larger upper two are called corpora cavernosa & the smaller lower one which contains the urethra is called the corpus spongiosum. The distal part of the corpus spongiosum overlaps the terminal ends of the two corpora cavernosa forming a slight bulging, called glans penis. The skin is folder over it. It is called foreskin or prepuce that's cut during circumcision. 6 The opening of urethra at the tip of glans penis is called the external urinary meatus. The main function of penis is erection (enlargement & rigidity of the penis) by filling of the cavernous tissue by blood for penetration of the vagina to reach the semen deeply near the women’s cervix. Spermatic cord: It's a fibrous covering of the vas deferens, blood vessels, lymph vessels & nerves. It extends from the top of the testis along the inguinal canal, up to the internal inguinal ring. Note: a) Sperm count is 70 million per ml of semen. b) Semen volume is 3-5 cm. 7 1.2 Anatomy of the Female Reproductive System The female reproductive system produces the female reproductive cells (the eggs, or ova and contains an organ (uterus) in which development of the fetus takes place. The system is includes the ovaries, uterus, uterine tubes, vagina, vulva, pelvis & breast. 1.2.1 Female pelvic Figure 1.3: Female reproductive organs. A, Sagittal section of pelvis lows location of female reproductive organs a) Function Allows movement of the body, especially walking and running. 8 Helps in child bearing (increased width and rounded brim woman are less speedy than men). Transmit the weight of the trunk to the legs, acting as a bridge between femurus. Protect the pelvic organ. b) Types of pelvic Gynecoid pelvis: The ideal pelvis for childbearing, its rounded brim. Android pelvis: It resembles the male pelvis and it’s the suited for childbearing. Its brim is heart- shaped with a narrow fore pelvis. Anthropoid pelvis: It has a long oval brim. Women with this type of pelvis tend to be tall, with narrow shoulders. The labour does not usually present any difficulties. Platypelloid pelvis (Flat): Has a kidney shaped brim, It is found in short and heavy woman. Figure 1.4 Characteristic inlets of the four types of pelvis. 9 Pelvic floor a) Function Responsible for voluntary control of micturition and play an important part in sexual intercourse. Allows exit to the fetus b) Muscle layer of the pelvic floor Deep layers Superficial layers 1.2.2 Ovaries Both ovaries are nodular glands of uneven surface, like large almonds in size & shape. Attached to the posterior surface of the broad ligament. The end of the uterine tube cup is over it without actual attachment. Functions: Oogenesis (egg production). Endocrine function: ovaries are the source of the female sex hormones estrogen & progesterone which are essential hormones in menstrual cycle & pregnancy. 1.2.3 Uterus In unmarried woman, the uterus is pear shaped, measures approximately 7.5 cm length, 5 cm in width, and 2.5 cm in thickness. The upper part is called the body, the bulging upper part of the body is called the fundus & the lower part is called the cervix (neck). 10 Uterine wall: consists of 3 layers: I) Endometrium: is the innermost layer It connects the endometrium to the underlying myometrium. This layer is stable, while the others will slough off during menstruation & deliver. Figure 1.5: Female pelvic organs in a frontal section. The entire uterus is shown, with the upper portion of the vagina and the left uterine tube and ovary. II) Myometrium: It's the thick middle layer. The fundus has the thickest part of myometrium. III) Parietal peritoneum: It's the outermost layer. 11 It covers all the parts except the lower fourth of the anterior surface & the cervix. Uterine cavity: The cavity is small because of the thick wall. It's flat & triangular. The base is upward & its apex is downward, constitutes the internal os which opens into the cervical canal which narrows on its lower end forming the external os which opens into the vagina. Blood supply of the uterus: The uterine blood supply is generous. The two uterine arteries are branches of the internal iliac arteries. The uterine & vaginal veins return to the internal iliac veins. Functions of the uterus: It's one of the genital tracts. Pregnancy site. Nutritional source for the fetus. Labor. Menstruation. 1.2.4 Uterine (Fallopian) Tubes Each one is about 10 cm long, attached to the outer upper angle of the uterus. 12 The mucosa of it has free connection with the uterine cavity medially & the peritoneal cavity laterally, so any infection in the tube "salpingitis" may extend to the peritoneal region caused peritonitis. It consists of 3 divisions: A medial third (isthmus) from the uterus. Ampulla: is the middle third, dilated part, passing over the ovary. Infundibulum: has a finger like processes called fimbriae with an opening that receive ovum. Functions: It is one of the ductal systems. It is the site of fertilization. Figure 1.5 uterine tubes in section. Note the ovum entering the fimbriated end. 1.2.5 Vagina It's a collapsabel tube, 7-8 cm long. It presents between the bladder & urethra (anteriorly) & the rectum (posteriorly). Functions: Receives the sperms during the sexual intercourse. 13 Birth canal. 1.2.6 Vulva Figure 1.6: External genitals of the female. It's the external genitalia which include mons pubis, labia majora, labia minora, urethral meatus, vaginal orifice, and bartholin's glands. Mons pubis: is a skin – covered pad of fat over the symphysis pubis. Labia majora (large lip): It's a pigmented skin, the outer surface is hairy & the inner surface is smooth. It's formed mainly of connective tissue & fat with numerous sweat & sebaceous glands. Labia minora (small lip): They are hairless folds of skin. The area in between the labia minora is called the vestibule. Clitoris: It's small erectile tissue and it’s sensitive during sexual intercourse. 14 It presents just behind the anterior junction of the labia minora. Urinary meatus (urethral orifice): is a small opening of the urethra, between clitoris & vaginal orifice. Greater vestibular gland (bartholin's gland): It's bean-shaped, one on each side of the vaginal orifice. Each opens by a long duct in a space between labia minora & the hymen and they secret mucus which lubricates the vaginal opening. 1.2.7 Breast Breast lays over the pectoralis muscles, connected to them by fibrous tissue and its Size depends on the amount of fat deposited. 15 Figure 1.7: Lateral view of breast. breast tissue is formed of two major organs: 1) Mammary systems: which include : a) Lactating glands: which are formed of distal alveoli, forming lobules, united to form lobes, arranged in grape like clusters. b) Ductal system: The ducts from the various lobules unite forming a single lactiferous( milk carrying) duct for each lobe, each enlarges slightly before reaching the nipple into small lactiferous sinuses, each duct terminates in a tiny opening on the surface of the nipple, each nipple is bordered by a circular pigmented area called areola, which contains many sebacious glands. 2) The connective tissue & fat: Which form the bulk of the breast, it is made mainly of fat, and the skin is anchored to the pectoral fascia by many fibrous suspensory ligaments. Breast function: The function of the breast is lactation, the factors affecting milk production are: 1) Estrogen hormones promote the ductal growth. 2) Progestrone stimulates the alveolar system. 3) Prolactin stimulates milk secretion. 4) Oxytocin stimulates milk ejection from the breast. Mechanisms of breast function: A high blood concentration of estrogen during pregnancy inhibits anterior pituitary secretion of prolactin, so no milk will be made during pregnancy. Shedding of placenta, after labor leads to marked decrease in estrogen level in the blood that stimulates anterior pitutary to secrete prolactin. 16 Sucking movements of a baby stimulates the anterior pituitary to secrete prolactin, and the posterior pituitary to secrete oxytocin to increase milk ejection. 1.3 Female reproductive cycles There are many periodical changes in female during the years between the onset of the menses (menarche) and their cessation (menopause) on the level of endometrium, ovarian, myometrial & gonadotropic cycle. 1) Ovarian Cycle: Before birth, the ovarian tissue begins a meiosis division; it reduces the number of chromosomes in the daughter cell by half. When a child was born, her ovaries contain many primary follicles, each contains an oocytes that have temporarly suspended the meiotic process before it's complete, once each month, on about the first day of menstruation, the oocytes within many primary follicles resume meiosis, one of them matures & migrates to the surface of the ovary, to be expelled from the ruptured wall of the mature follicle during ovulation. Ovulation usually occurs 14 days before the next menstrual period begins. Immediately after ovulation, cells of the ruptured follicle enlarged & transformed into a golden colored body which called corpus luteum. The corpus luteum which grows for 7-8 days, during this period will secrete high amount of progesterone. Then the corpus luteum will be nonfunctioning white scar, called corpus albicans which moves to the center of the ovary & finally disappears. 2) Endometrial( menstrual) cycle: During menstruation, parts of compact & spongy layers of the endometrium slough off, leaving denuded areas. After menstruation, this cell layer will proliferate causing the endometrium to 17 reach a thickness of 2-3 mm by the time of ovulation. Part of this is secreting a nutrient fluid during the time between ovulation & the next menses. A day before menstruation starts again, a drop in progesterone level causes contraction of the muscle layer of the arteries that supply the glands, producing endometrial ischemia, leading to the death of the tissue, and sloughing of the endometrium(bleeding) . So we can divide menstrual cycle into phases: a) Menses: occurs on days 1-5 of a new cycle. b) Postmenstrual phase( between the end of menses & ovulation), so it can be described as " preovulatory phase" it starts from the 6 th to 13th day of a 28 days-cycle. This period is called estrogenic or follicular or proliferative phase. c) Ovulation: occurs on cycle day 14 in a 28- day cycle. d) Premenstrual phase (postovulatory) between ovulation & the onset of menses, it's secretory or luteal phase so progesterone will be secreted, it takes from 14 days to 28 in a 28-day cycle. 3) Myometrial cycle: Myometrium contracts mildly but with increasing frequency during the two weeks preceding ovulation, to decrease or stop during ovulation & after that. 4) Gonadotropic cycle: Control of female reproductive cycles: The anterior pituitary gland secretes two hormones, LH & FSH The hormones will play a major role in producing the cyclic changes in woman. Control of cyclical changes in the ovaries: 18 FSH & LH are responsible for the ovarian changes. Control of cyclical changes in the uterus: The main factors are the level of estrogen & progesterone. Increase of estrogen during the post menstrual phase will cause: a) Proliferation of the endometrium cells. b) Growth of the endometrial glands. c) Increase in endometrium water content. d) Increase in myometrial contraction. 19 Figure 1.8 MENSTRUAL CYCLE (left half). Diagrammatic representation of the action of the gonadotrophic hormones on the ovary and of the ovarian hormones on the endometrium. EARLY PREGNANCY (right half). Diagrammatic representation showing ovulation, fertilisation, decidual reaction and embedding of the fertilised ovum. Increase of progesterone during the premenstrual phase will cause: a) Increase secretion by endometrial glands. b) Increase in the endometrium water content. c) Decrease in myometrial contraction. 20 Importance of female reproductive cycles: 1) Production of ovum is the main role. 2) Preparing the uterine endometrium for suitable implantation, so constant renewable of the endometrium makes successful implantation. Notes: Manarche: is the first flow of menstruation, at puberty, at about the age of 13 years, with many variations. Menopause (climacteric) is the cessation of menstruation from about the age 45-50 years. After menopause, estrogen concentration decreases dramatically, which causes negative feedback response that increases the gonadotropin levels. 21 1.4 The Physiological Changes in the reproductive system due to Pregnancy Pregnancy is a period of enormous physiological change in a relatively short space of time. Understanding the normal changes can help to: Differentiate normality from the minority of women who experience pathological changes. Explain the multitude of symptoms described in “normal” pregnancy. Explain the altered reference ranges in pregnancy for laboratory investigations and their subsequent interpretation. Explain the different responses to some emergencies in pregnancy. 1.4.1 The Uterus in weight from 60 gm in size from 7.5 × 5 × 2.5 Contract and shorten during labour causing the upper uterine segment to 900gm. 30 × 23 × 20 cm. thicken and shorten. Blood supply increase to meet the demands of a growing uterus. 1.4.2 The Cervix Softer, cervical glands secrete mucus plug-like as a barrier against infection. 1.4.3 The Vagina Hypertrophy, more elastic, amount of white vaginal discharge = Acid media leucorrhea. Mucosa cell in glycogen content + doderlin bacilli more protection but candida increased. 22 1.4.4 Endocrine System Placental hormones: Human placental lactogen alter the metabolism of the mother. a) Maternal energy needs are met by mobilizing free fatty acid. progesterone muscle tone. b) More insulin is produced centrally, but its action is blocked leading to insulin sensitivity blood glucose. Pituitary hormones: AP gland enlarged. Adrenocortrophic hormone, melanocyte-stimulating hormone and thyrotrophic hormones . FSH & LH by progesterone and estrogen. Prolactin PP gland stimulated to produce oxytocin. Aldosterone produced due to response to the rennin-angiotension. (Prolactin × estrogen). Adrenal glands: Corticosteriod production (one of the reasons for glycosuria in pregnancy). BP and striae gravidarum are caused by Na+ , Cl- excretion due to response to the rennin – angiotension. secretion. 23 Thyroid function: Figure 1.10 1.4.5 Changes in the Respiratory System Progesterone acting on the respiratory center in the hypothalamus threshod for Pco2 excretion of co2 from the fetus. deeper breathing o2 tension. Respiratory rate not alter, but the amount of air exhaled/min Pco2 from 7 – 11 liters. 1.4.6 The Breasts Estrogen develops the ducts system and progesterone on the glandular tissue. Prolactin stimulates the production of colostrum. The breasts enlarge due to tissue growth, blood supply and fat deposition. 24 1.4.7 Maternal Weight 2.0 kg in the first 20 weeks O R weeks 0.5 kg/per week until term 4.0 kg in the first 20 0.4kg/week until term 12.0kg approximate total 12 kg approximate total a) Breast 0.5kg b) Fat 3.5kg c) Placenta 0.6kg d) Fetus 3.4kg e) Amniotic fluid 0.6kg f) 0.9kg Uterus g) Blood volume 1.5kg h) Extra cellular 1.0kg fluid Total 12.0kg 1.4.8 Changes in the Gastrointestinal System Estrogen makes the gum spongy and lead to bleeding. Gingivitis. Salivation, change in taste, food craving for uncommon substances as clay, coal etc (pica). gastric empting and peristalsis . Progesterone relaxes smooth muscle Heartburn, gastric reflux. Constipation, hemorrhoids. N & V (nausea and vomiting) due to estrogen,HCG. 1.4.9 Skin changes Melanin –stimulating hormones Lingea nigra pubis to umbilicus. Striae gravidarum =red strips during pregnancy, could be due to deeper pigmentation = chloasma. in corticosteroid hormone, after delivery these red colour changed to slivery white one = lingea alba. 25 1.4.10 Skeletal changes Progesterone and relaxin lead to relaxation of ligament and muscle. Readiness for labour. Backache and ligament pain. 1.4.11 Changes in the cardiovascular system Due to workload, increase in size. Cardiac output Co = SV x HR. CO = Red blood cell mass from 5-7 liters/min. V. x HR (15 B/Min). 18-30% and plasma cell 50% (increase in plasma cell exceed the increase of RBC lead to hemodilution ( hemoglobin) which lead to Physiological anemia. Acceptable Hgb for pregnant women 11 – 12 gm/dl. Iron metabolism: a) Stored for mother use to maintain her circulating Hgb level and to supply the fetus. b) The greatest need for iron in the last 4 weeks of pregnancy. Plasma Protein: a) in pregnancy but in concentration due to hemodilution. b) Mainly albumin component osmotic pressure which lead to increase physiological edema. Clotting factors: a) Fibrinogen, factor 7 & 10 & platelets are change in coagulation time from 12 – 8 min. b) Capacity for clothing high risk for thrombosis, embolism and DIC (disseminated intravascular coagulation). 26 White blood cells: a) WBC 10 – 15 x 109 /liter. b) c) Level of immunoglobulin. Immune system. Bp remains the same or drops slightly in the first trimester. Blood flow to placenta (80%) and to the kidney urination. 1.4.12 The Growth of the Pregnant Uterus 8 weeks: Can not be palpated abdominally. 12 weeks: on the symphysis pubis. 16 weeks: Half way between the symphysis pubis and the umbilicus or 7.5cm above the symphysis pubis. 20 weeks: 2 fingers below the level of the umbilicus or 15 cm above the symphysis pubis. 24 weeks: The fundus is at upper margin of the umbilicus. 20 cm above symphysis pubis. 30 weeks: The fundus is midway between the umbilicus and the xiphisterum. 24 cm above symphysis pubis. 36 weeks: Highest level and contact with the xiphisterum. 30 cm above the symphysis pubis. 40 weeks: Uterus is ready to go into labour. 27 Figure 1.11: Fundal heights at pregnancy 28 1.5 Minor Disorder of Pregnancy Causes: Hormonal changes, metabolic changes, postural change. Nausea and Vomiting: 4 - 6 weeks. Hormonal causes. Human chorionic gonadotrophin HCG, progestrone and estrogen. Early morning, "morning sickness". Nursing role: Reassurance, explanation. Salad, light diet, avoids full meal. Carbohydrate snacks at bed time "before out of bed". If sever vomiting, mother lose weight, dehydrated, hyperemesis gravidarum (treated in the hospital). Heartburn: Burning sensation in the midiastinal region. Progestrone relaxes the cardiac sphincter of the stomach and allows reflux of gastric contents into the esophagus. Difficult at 30-40 weeks (fetus growing). Nursing role: Avoid bending over. Small frequent meals. Sleeping with more pillows. May prescribe antacids. 29 Ecessive salivation (ptyalism): At 8 weeks due to hormonal changes. Linked with heartburn. Explanation and attentive listening are helpful. Pica: Mother craves certain foods or unnatural substances such as coal, lemons, and clays. Nursing Role: Unknown cause? Hormonal and metabolic changes. Inform the mother that unnatural substances could harm the baby. Constipation: Progestrone causes relaxation and decrease peristalsis of the intestine. Nursing role: a) Eat fibre diet. b) Increase exercise. c) Increase fluid in take. d) Practice usual bowel habit. Backache: Due to changing center of gravity. Hormonal soften the ligaments of the pelvis. Backache linked with the Urinary Tract Infection. Cramp: Unknown cause, could be due to ischemia or result from changes in the ph or electrolytes. Dorsiflex the foot (Knee straight and stretch the calf muscle by pulling the foot upwards at the same time). Gentle leg movement, raise the foot 25cm. 30 Warm bath. B complex and calcium. Frequency of micturition: Leucorrhea: a) White, non-irritant vaginal discharge in pregnancy. b) Personal hygiene, underwear and avoid tights. c) Washing with plain water, talcum powder. d) ? thrush or trichomonas. Fainting: a) Vasodilation due to progestrone. b) Avoid long period of standing id helpful. c) Side lying position should be encouraged. Varicosities: a) Progestrone relaxes the smooth muscles of the veins and result of sluggish circulation. b) Valves dilated become inefficient and varicosities result. c) Hemorrhoids, vulval varicosities. d) Family history, long period of standing or sitting, exercising the calf muscle. Skin: a) Linea nigra and areola of the breast. b) Chloasma. c) Itching in the abdomen ( bilirubin level). 31 1.6 Antenatal Care of Pregnancy 1.6.1 Aims of Antenatal Care To support & encourage family's healthy psychological adjustment to child bearing. To promote an awareness of sociological aspect of childbearing. To monitor the progress of pregnancy to ensure maternal health & normal fetal development. To recognize deviation from normal & provide management or treatment as required. To prepare the woman to delivery. To support the mother in breast- feeding & infant feeding. To offer family advice on parenthood. To build up a trusting relationship between the family & their caregivers. Menstrual History: 1.6.2 History Last menstrual Day(LMD) Expected date of delivery. Obstetric History: Gravida: total number of pregnancies including the present pregnancy. Grand multigravida: woman who has been pregnant five times or more Para: The number of fetuses delivered after the point of viability (20 weeks’ gestation. Whether or not they are born alive. Grand multipara: woman who has given birth five times or more. 32 Medical history: History of UTI Essential hypertension Asthma, epilepsy, infection. Family history Any genetic problems, genetic disease, diabetes, hypertension. Physical Examination: a) Height b) Weight c) Blood pressure d) Urine analysis(check for ketones,glucose,protein) Blood Test: a) Blood group & RH b) Hgb c) HIV d) Rubella e) Alpha fetoprotein screening General appearance & Breast Examination. Abdominal exam edema Definitions used for assessment: a) Fetal Lie: describes the long axis of the fetus in relation to the axis of pregnant woman . b) Fetal Attitude: refers to the relationship of the fetal parts to one another. c) Fetal Presentation: refers to the foremost part of the fetus theat enters the pelvic inlet. 33 d) Fetal Position: is determined by comparing the relationship of an arbitrarily determined reference point on the presenting part to the quadrants of the maternal pelvis. Reference points for determining position Presenting Part Reference Point Vertex Occiput Brow Frontum(Brow) Face Mentum(Chin) Breech Sacrum Shoulder Scapula e) Engagement: When the presenting part of fetus descends to the level of the ischial spines. Risk factors arising during pregnancy: Fetal movement pattern changed Hb lower than 10 g/dl Poor weight gain ,weight loss Proteinurea, glycosuria, bacilluria BP systolic above 155, diastolic above 90 mmhg Uterus large or small for dates Excess or decreased liquid Malpresentation Head not engaged in prim gravid woman by 38 weeks Any vaginal bleeding Premature labour Vaginal infection 34