Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
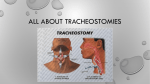
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES, BANGALORE, KARNATAKA SYNOPSIS PROFORMA FOR REGISTRATION OF SUBJECT FOR DISSERTATION 1st YEAR. M.Sc NURSING MEDICAL SURGICAL NURSING YEAR 2010– 2011 RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES BANGALORE, KARNATAKA PROFORMA FOR REGISTRATION OF SUBJECTS FOR DISSERTATION KARTHEC SHIVARAJ 1. NAME OF THE CANDIDATE SHANTI DHAMA COLLEGE OF NURSING,SUNKADAKATTE, AND ADDRESS MAGADI MAIN ROAD,BANGALORE-91 SHANTI 2. NAME OF INSTITUTION DHAMA COLLEGE OF NURSING 3. COURSE OF STUDY AND I YEAR M.SC. NURSING DEPT SUBJECT OF MEDICAL SURGICAL NURSING 4. DATE OF ADMISSION TO 07-06-2010 COURSE A STUDY TO ASSESS THE EFFECTIVENESS OF STRUCTURED TEACHING PROGRAMME ON KNOWLEDGE ABOUT CARE OF CHILD IN COMA AMONG STAFF NURSES IN SELECTED HOSPITAL IN BANGALORE. 5. TITLE OF THE STUDY 2 BRIEF RESUME OF THE INTENDED WORK “With every birth, man may calculate that God is still hopeful in his creature”. - Wordsworth 6. INTRODUCTION There is an evidence that surgical incision into the trachea is an attempt to establish an artificial airway was performed by a Roman physician 124 years before the birth of Christ. A tracheostomy, commonly called a ‘Trach’ refers to a surgically created hole that extends from the neck skin into the windpipe or trachea. Tracheostomy should rarely be considered for emergency access and control of the airway. 1 The procedure may require for various reasons, those include obstruction in the upper airway caused by oedema of the glottis or by carcinoma of the larynx, potential protect the lungs from potential threats such as obstruction or aspiration, effective removal of secretions from the trachea and lower airways, patients with sputum retention, a very common indication is to permit long term ventilatory support. Many persons have tracheostomy to bypass obstruction in their airway from injuries, scarring or tumours, and for treatment of sleep disorders such as obstructive sleep apnea.2 3 Appropriate care for patients with tracheostomy in hospital settings is an important issue. Each year more than 700000 patients receive tracheostomy. Tracheostomy in the intensive care unit is increasingly used as a means to speed weaning from mechanical ventilation and to provide a safe airway. Tracheostomy allows earlier discharge of patient’s from the ICU, thus allowing better management of limited ICU resources, and may be associated with reduced mortality.3 Tracheostomy requires more sophisticated skill and equipment. Surgical tracheostomy is performed in the operating room or less commonly in an intensive care unit under general or local anesthesia. With the patient positioned with neck hyper extended, the skin area is prepared and an incision is made bellow the cricoid cartilage . The trachea is located with blunt dissection, bleeding is controlled if necessary, and an incision (one or many types) is made through the second and third or fourth tracheal cartilage. A cuffed tracheostomy tube of proper size and length is inserted through the anterior wall of the trachea as the endotracheal tube is fixed on the ostomy site. The tracheostomy tube is gently positioned and ventilation is confirmed.4 Although details vary depending on the type of tracheostomy tube, tracheostomy care includes cleaning or changing the inner cannula, changing the dressing and tracheostomy tube holder, and suctioning if needed. Most tracheostomy tubes have disposable inner cannulas, which are replaced and secured using aseptic technique. Never clean and reuse a disposable cannula. Reusable inner cannulas require careful cleaning. Perform hand hygiene, don a face shield (or goggles and mask) and sterile gloves, and maintain aseptic technique during the procedure. Unlock and remove the inner cannula 4 and place it in a solution of equal parts hydrogen peroxide and 0.9% sodium chloride unless the manufacturer directs otherwise. Remove encrusted secretions from the lumen with sterile pipe cleaners. After cleaning, rinse the cannula thoroughly with sterile 0.9% sodium chloride solution. Reinsert the inner cannula and securely lock it into place.5 While providing tracheostomy care, inspect the skin for signs of irritation or infection, such as erythema, pain, or discharge. Thoroughly assess the skin around the tracheostomy for evidence of skin breakdown related to the tracheostomy device, tube securement device, or mucus and secretions. Clean the area around the tracheostomy tube with a non cyto toxic cleanser using a sterile cotton-tipped applicator. Then rinse the skin with water and dry it gently with sterile gauze. If you see skin breakdown, consult a wound/ostomy/continence nurse for an individualized patient plan of care.6 Absorbing secretions helps prevent maceration and skin breakdown. Place a prepackaged, sterile tracheostomy dressing under the tube flanges. Always use a manufactured split sponge rather than cutting a gauze pad. Never place anything with loose fibers around the stoma or tracheostomy tube because they can cause irritation. Inform the healthcare provider if sutures used to secure the tube after insertion are irritating the skin or preventing routine maintenance. Obtain an order for suture removal 7 days after tracheostomy tube insertion. If twill tape was used, change it to a Velcrosecuring device as soon as possible because it's more comfortable and less likely to abrade the skin.7 Maintaining humidification is another key nursing responsibility. Normally, the nasopharynx humidifies inhaled air. Because the tracheostomy tube bypasses the upper 5 airway, you need to provide adequate humidity to keep the airway moist. In hospitalized patients, this can be accomplished by a heat and moisture exchanger on a mechanical ventilator or a T-piece or tracheostomy mask. In addition, your patient must be properly hydrated; for example, with I.V. fluids.8 Because the patient can't cough effectively to clear secretions, be prepared to suction him as needed. Suctioning raises the risk of hypoxemia, bronchospasm, and other adverse reactions, so suction only when needed, not on a set schedule, and suction for the shortest time necessary to clear secretions. Indications for suctioning include coughing, secretions in the airway, respiratory distress, presence of rhonchi on auscultation, increased peak airway pressures on the ventilator, and decreasing SaO2 or PaO2.9 Besides hypoxemia and bronchospasm, complications associated with suctioning include atelectasis, dysrhythmias (including bradycardia), increased intracranial pressure, and airway trauma. Bradycardia is attributed to vagal nerve stimulation. It helps to prevent hypoxemia, hyperoxygenate the patient before and after suctioning. As you suction, look for signs of hypoxemia, such as hypertension, dysrhythmias, and a drop in SpO2 by pulse oximetry. If this occurs, stop suctioning and hyperoxygenate the patient. If the patient is on mechanical ventilation, allow time for the increased oxygen percentage to come through the ventilator tubing and reach the patient. Use the ventilator, not a manual resuscitation bag.10 6.1 NEED FOR THE STUDY A growing trend in recent years has been the long term management of stable, but chronically ill and technology dependent patients in the home. Same way some patients 6 may sent home with tracheostomy. In this case, the nurse and respiratory therapist are both responsible for teaching the patient and the family how to perform site care at home.11 Without specific strategies to address tracheostomy care on the wards. Patient discharged from the intensive care unit with the tracheostomy may receive suboptimal care. Choch’s and colleagues reported the ICU patients who received tracheostomies and were sent to the ward from the ICU with a tracheostomy in situ had significantly higher adds of death than those patients decannulated in the ICU prior to discharge.12 Early discharge planning, and care giver training are required competent of the care and treatment of any patient with a chronic illness. In a health care environment moving qualitatively into an evidence based approach to medical procedures and care there appears to be an absence of such scientific evidence when seeking guidance and standards for the long term management of patients with tracheostomy.13 A study conducted to assess the effectiveness of the multidicipilinary training to the staff regarding tracheostomy care. To evaluate the service, data were properly collected over the course of 3 years on 400 ICU patients in Vincent’s hospital, Melbourn.The data was compared with outcomes in the year preceding the introduction of the service. Result revealed that 176(62.9%) of patients got early discharge and decannulisation . Chronic illness decreased over time from 50 to 30. The multivariate analysis showed that the hazard for decannulisation increased by 24% per year. An intensivist tracheostomy team is associated with shorter decannulisation time and length of stay which may result in financial benefit to the institutions.14 7 6.2 REVIEW OF LITERATURE A study conducted to assess the effectiveness of multi disciplinary care for tracheostomy patients in U.K. The prospective data over a period of 24 months were collected from 117 patients. The result showed that survival rate was higher from p=0.006 to p=0.008, and 57 (49%) survivers were successfully decannulated with mean post tracheostomy days of 24+_15. The major complications were reduced to 15%. Only six patients had an episode of desaturation after procedure and there were three episode of a bleeding and onl;y 2 patients developed stomal cellulites.15 A study conducted to assess the indications for tracheostomy among 124 patients, there were 99 (85%) males and 18 (15%) were females. Mean age was 46+_17 years for males and 6+_ 24 years of females, there were 57 (49%) patients with road traffic accidents resulting in polyttrauma and head injury, while 60 (51%) patients had medical reasons for admission. Among medical group opf patients 18 (30%) were admitted with the diagnosiss of sepsis, 27(45%) with hemorrhagic or ischemic cerebrovascular accident , 12 (20%) were with acute poisoning. Most of the polytrauma patients were young adults, but the most common co morbidities among both medical and polytrauma group were hypertension( 62%).and others by diabetes mellitus(43%), and ischemic coronary artery disease(23%).16 An observational retrospective study conducted to assess the tracheostomy patients in Nigeria among 500 patients. Hospital records were reviewed for demographic indications for admissions, duration of a admission, outcome. Result showed that 10(2%) had tracheostomy while admission. All patients had surgical tracheostomy . Eight 8 patients had post surgical tracheostomy to maintain a patent airway following post operative airway obstruction, while 2 patients had tracheostomy for Guiilien Bare Syndrome, and severe head injury, there were 4 deaths.17 A reterospective descriptive study conducted to assess the epidemiologic profile of patients with tracheostomy among 87 patients in Terapia. Result showed that mean age was 58+_17 years orotracheal intubation before tracheostomy was 11.17+_4.78 days, mean age of patients who died (65+_17) years was greater than who shifted to ward 53+_16 years, p=0.003. Mean age of who died in hospital 62+_17 years was also higher than survivers 52+_16 years, p=0.008, old age (>65 years ) was related to mortality. Thete were no other variables related to mortality in the sample.18 A comparative study conducted for tracheostomy versus prolonged intubation in medical intensive care unit patient in Rock university over 7 years among 60 patients, tracheostomy group consists of (n=30), medical intubated group consists of (n=30). They measured duration of hospital, length of stay in hospital, incidence of each technique and mortality in ICU, TG 30.96+_9.47 versus 34.26+_ 9.74;p=0.2, difference in mortality rate in ICU TG 26.7% VS IG 46.7%, p=0.1, No tracheal stenosis noted in two groups. Nasocomial pnemoniopathy was precocious in the IG than TG, they noticed one case of minor bleeding.19 A study conducted to assess the malposotion of the tube causes barrier to early weaning. A retrospective study conducted on 403 patients in Canada. Malposition of tube found in 40 (10%) patients, malposotion of tube caused anoxia in 6.42% of patientsand 9 delayed recovery seen in 1.82% of patients, malposotioned tube changed in 805 of patients. Malposition associated with prolonged mechanical ventilation. 20 A comparative study conducted to assess the outcome of early and late tracheostomy among 15,950 subjects in U.K. Randomised controlled trial used. Result revealed that early tracheostomy did not significantly altered mortality (relative risk of 0.19 (95%) confidence interval 0.45 to 1.39). The risk of pneumonia was also unaltered by the timing of tracheostomy (0.90, 0.66 to 1.21), Early tracheostomy significantly reduced duration of artificial ventilation (weighted mean difference – 8.5 days, 15% confidence interval – 15.3 to 1.7 and length of stay in intensive care -15.3 days, -24.6 to 6.1). The study concluded that critically ill patients who require prolonged mechanical ventilation, performing a tracheostomy at an earliar stage than is currently practiced may shorten the duration of artificial ventilation and strength of stay in intensive care unit.21 A prospective study conducted to assess resource utilization benefits in early tracheostomy patients among 653 subjects. Result showed that 136 (21%) required tracheostomies, 29of whom were early and 107 were late. Duration of hospital stay found with early tracheostomy, (mean standard deviation was 9.6+_1.2 days versus 18.7+_1.3 days p < 0.0001). Similarly ICU stay was significantly (10.9+_1.3 days versus 21.0+_ 1.3 days, p < o.ooo1). Tracheostomy patients were discharged from the ICU after comparable period in both groups (4.9 +_ 1.2 days, not significant) when using multivariate analysis, late tracheostomy was an independent predictor of prolonged ICU stay(>14 days).22 10 6.3 STATEMENT OF THE PROBLEM A study to assess the effectiveness of S T P on knowledge regarding care of patient with tracheostomy among IV- year B. Sc Nursing students at selected nursing college Bangalore. 6.4 OBJECTIVES OF THE STUDY: 6.3.1 To assess the pre knowledge of students regarding tracheostomy care. 6.3.2 To assess the post knowledge of students regarding tracheostomy care. 6.3.3 To compare the pre and post knowledge regarding tracheostomy care. 6.3.4 To associate the findings with the demographic variables. 6.3.5 To evaluate the students level of understanding with S T P. 6.4 OPERATIONAL DEFINITIONS: Assessment: It refered as a evaluation of students basic knowledge score and knowledge improvement after STP. Effectiveness: Effectivenesss referred as improvement of knowledge among the students after phamphlet view. Knowledge: Knowledge referred as student’s awareness regarding tracheostomy care. STP Referred as a planned teaching with audio visual aids. Tracheostomy: Referred as an surgical open made in the wind pipe to promote airway . 11 6.6. HYPOTHESIS: H1 Students knowledge may increase after STP. H2 students will gain in depth knowledge regarding care of patient with tracheostomy 6.7 ASSUMPTIONS: Students may have inadequate knowledge regarding tracheostomy care. Students knowledge may improve after the structured teaching programme. 6.8 LIMITATION: 1. The study was limited to students in selected nursing college Bangalore. 2. The study was limited to those who are able to understand Kannada and English 3. 6.9 The sample size was limited only for 60 samples. VARIABLES: Independent variable: students knowledge score improvement after S T P. Dependent variable: knowledge score variation with different students. 7.0 MATERIALS AND METHODS: 7.1. SOURCE OF DATA COLLECTION: Data will be collected from IV-year B.Sc nursing students at selected nursing college, Bangalore. 7.1.1 RESEARCH DESIGN: An experimental design on group with pretest and post test. 7.1.2. RESEARCH APPROACH: 7.1.3. SETTING OF THE STUDY: Data collection from the students will be conducted in 7.2. METHOD OF DATA COLLECTION: 12 Data will be collected with structured administered questionnaire on knowledge regarding care of patient with tracheostomy. 7.2.1. SAMPLING TECHNIQUE: The selected sampling technique for the study is convenient sampling technique. 7.2.2. SAMPLE SIZE: Sample size for the study is 60. DURATION OF THE STUDY: Study duration will be 4 weeks. 7.2.3 SAMPLING CRITERIA: INCLUSION CRITERIA: 1. Students who are willing to participate. 2 Students who study IV-year B.Sc nursing. 3. Students who know to read and write Kannada and English language. EXCLUSION CRITERIA: 1. Students who are not willing to participate. 2. Students who are not IV-year B.Sc nursing. 3. Students who do not know to read kannada and English. 7.2.4. TOOL FOR DATA COLLECTION: Procedure for data collection, the investigator will collect data from students using structured administered questionnaire schedule to assess the knowledge after obtain the prior permission from participant. Pretest will be conducted following which the structured knowledge questionnaire will be given. Post test will be 13 conducted after 7 days and data will be analyzed using descriptive and inferential statistics. 7.2.5. DATA ANALYSIS METHOD: Descriptive statistics: A data analysis will be include descriptive statistics such are frequency, mean, mean percentage, standard deviation to interpret the knowledge scores, demographic variables, emotional well being assessment. Inferential statistics: Inferential statistics such are ‘t’ test will be used ti find the difference between pre test and post test knowledge score and chi square will be used to see the association between selected demographic variables and post test knowledge score. These findings will be documented in tabulation, graphs, and diagrams. 7.3 DOES THE STUDY REQUIRE ANY INTERVENTION TO BE CONDUCTED ON PATIENT OR OTHER HUMANS OR ANIMALS? Yes, this study will be conducted as an intervention to IV- year B.Sc nursing students regarding care of patient with tracheostomy at selected nursing college. 7.4 HAS THE ETHICAL CLEARANCE BEEN OBTAINED FROM THE INSTITUTION? Yes, Permission will be obtained from 1. The research committee of 2. Authority of selected nursing college at Bangalore. 3. Informed concern will be taken from the students who are willing to Participate in the study. 14 8.0 LIST OF REFERENCES: 1. Dr.Lyoop, Bedert L, Tracheostomy; clinical review and guidelines, Europian journal of cardio thorasic surgery, 32 (3); 2007. 2. Stauffer JT, Olson DN, Endotracheal intubation and tracheostomy, American journal for medicine 70(180); 2005. 3. Rodenjuez JL, Stainberg SM, Early tracheostomy for primary airway management, British medical journal, 108(4); 2004. 4. Racy E, Bobbin, Laryingeal and tracheal complications, American journal of medicine, 90(3); 1986. 5. Griffins JF, Barber VS, Systemic review of tracheostomy in adult patients, British medical journal, 330(7502); 2005. 6. Zollinger JR, Zollinger Sr, Zollinger’s Atlas of surgical operations, 8 th edition, Newyork, McGrew- Hill 2003. 7. Clum S, Rembhark M, Mortality and tracheostomy, Critical medical journal 35(3); 2007. 8. Jeanna Brigs, Tracheal suctioning of adults with an artificial airway- Best practice 4(4); 2000. 9. Simpson TP, Day CJ Care of critically ill, Critical care journal 54(8); 1999. 10. Combes A Luyt CE Tracheostomy associated with better outcome, Critical care medical journal, 35(8); 2007. 11. Lewis T, Oliver G , Improving tracheostomy care in home, Nursing standard, 9(33); pubmed abstract,2005. 12. Leung R, Mac Gregor L, et al, Decannulisation and survival following tracheostomy in an intensive care unit, American nursing journal,112; 1846;2003. 13. Flatton H, Gierde S, Heimdal JH, The effect of tracheostomy on outcomes in intensive care unit patients, Acta anesthetical scand, 50;92;2006. 14. Mohamed siddique, Is tracheostomy associated with better outcomes for patients regarding long term mechanical ventilation, critical care medical journal 2(35); 2007. 15 15. Ahmed R, Raddy SR, Percutaneous tracheostomy in critically ill patients, Annual thorasic medical review5(26); 2010. (Available on http:// www. Thorasic medicine.org/text.asp/2010/51/26/58956.). 16. Dayal VS, Masri W, Tracheostomy in the intensive care setting, American medical journal, 8(347); 2008. 17. Klaus westpaul, Christian Byhaun, Tracheostomy saves life, British medical journal, 84(10); 2007. 18. Claudio Dornes, De Oliveria, Leonard de Cruz, Epidemiologic profile of tracheostomy patients, British medical journal, 48(3); 2007. 19. Berlauck JR, Prolonged endotracheal intubation versus tracheostomy, Critical care medical journal, 14(8); 2006. 20. Ulrich schnidk MD, Tracheostomy tube malposition, Critical medical journal, 24(3); 2005. 21. John griffitts, Early tracheostomy recovers soon, American nursing journal, 34(8); 2005. 22. Yashan, Arabi, Early tracheostomy improves resource utilization , ccritical care medical journal, 8(347); 2004. 16 9 SIGNATURE OF THE CANDIDATE 10 REMARKS OF THE GUIDE 11 NAME AND DESIGNATION OF THE GUIDE 11.1 GUIDE NAME AND ADDRESS 11.2 SIGNATURE OF THE GUIDE 11.3 HEAD OF THE DEPARTMENT 11.4 SIGNATURE OF THE HOD 12.1 REMARKS OF THE PRINCIPAL 12.2 SIGNATURE OF THE PRINCIPAL 17