Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
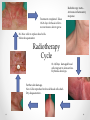
Support of the Head and Neck patient during Radiotherapy/Combined Chemo-Radiation(CRT) Anne Hope Head and Neck CNS RSCH AIMS • • • • Gain an understanding treatment implications/toxicities of RT/CRT . The Role of the Holistic Needs Assessment. Involvement of MDT Evidence Based symptom control/supporting patient. The Current Practice • Increase in use of combined Chemo-radiation – HPV RELATED ? • Overall increase in 100% over past year. • Most common sites treated: Oropharynx/Hypopharynx/Tongue/Larynx. • Cisplatin /Carboplatin/Cetuximab. • 5/10/20/30 # RT (Depending on goal/disease) Pre - Treatment Support • • • • • Introduce to the MDT – attend MPC. Holistic Assessment Patient Information/Education BUDDY ? Referrals to necessary support services. Holistic Assessment Holistic Assessment • Cancer Reform Strategy (CRS) (2007), Nice Guidance in supportive and palliative care(2004), Cancer Action Team (2007). • Buzz word in Cancer Care • Peer Review Measure • Enables MDT approach/Team work • Encouraged at key points of the Patient journey. Common ProblemsPsycho-social • • • • • • • Withdrawn Depression Anxiety Inability to work Sexuality/Body Image Loss of role in family/relationship Financial difficulty Common ProblemsClinical • • • • • • • • • Oral Mucositis Skin Reaction Pain Xerostomia Dysphagia Copious/thick secretions Aspiration Fatigue ORN Oral Mucositis Presentation • OM defined as ‘ Inflammation of the mucosal membrane, often characterised by ulceration resulting in the impairment of the ability to talk, pain and dyshagia.’ (Rubenstein et al, 2004) • 40 % of patients undergoing chemotherapy for solid tumours. • 97% receiving RT to H&N will suffer with OM. Presentation …contd • • • • • • Pain/Discomfort Ulceration Erythema Dysphagia Bleeding Necrotic/sloughy ulceration Prevention • • • • • • • Little evidence/ no avoidance. Dental Assessment pre treatment. Necessary dental extractions. Avoidance alcohol/smoking/spicy foods. Oral brushing/rinsing after every meal. Soft tooth brush/Flossing. High Fluoride Toothpaste. Management • Manage symptom e.g pain WHO ladder. • Use of recognised oral assessment Guide e.g WHO Oral Toxicity Scale. • Consistent Assessment…..Daily ? • Saline mouth rinses QDS/Sodium bicarbonate. • Asprin Gargles 300mg QDS. • Topical Agents, e.g Gelclair/Mugard • Difflam/Corsodyl. • Preventative Rinses- Caphosol? • Manage Infections/Candida. Skin Care Presentation • 85% Patient receiving external beam RT will experience moderate –severe skin reaction. • 10 % Moist Desquamation. • Usually seen 10-14 days following first fraction. • Is not a burn ! – Reaction differs /damage to skin with RT migrates upwards and effects epidermal layer only. • Usually increases up to 7-10 following last treatment. • 4-6 weeks following completion of treatment skin healing well. Radiotherapy starts – Activates inflammatory response Treatment completed- Takes 10-21 days for basal cells to recover &new skin to grow. No New cells to replace dead cellsMoist desquamation Radiotherapy Cycle 10-14/Days damaged basal cells migrate to skin surface. Erythema develops. Further skin damage. New Cells reproduce before old dead cells shedDry desquamation . RTOG Grading Scale Assessment / Observation Effects of Radiotherapy on Skin Cells RTOG 0 No visible change to skin RTOG 1 Faint or dull erythema. Mild tightness of skin and itching may occur RTOG 2 Bright erythema / dry desquamation. Sore, itchy and tight skin RTOG 2.5 Patchy moist desquamation Yellow/pale green exudate. Soreness with oedema RTOG 3 Confluent moist desquamation. Yellow/pale green exudate. Soreness with oedema RTOG 4 Ulceration, bleeding, necrosis (rarely seen) Cetuximab Reaction Management • • • • • • • Priority – To avoid treatment breaks – delays Maintain comfort/function Maintain skin integrity. Reduce pain. Promote hydrated skin. To avoid /reduce Infection. Reduce risk of complications/further trauma. Management…..contd • Avoid tight fitting clothing. • General moisturisers stop-if skin broken. • Hydrocolloid gel –skin breakdown. e.g Intrasite Gel. • Non adhesive dressings- moist desquamation. • Soft silicone dressings e.g Polymem, Meplilex lite. Recommendations • Wash Daily with a simple soap and water. • Avoid rubbing/irritating affected area. • Moisturise skin twice daily- Product choice little evidence. • However do avoid SLS, Lanolin, products with high levels of paraffin/petroleum. • Aquamax- RSCH preference. • Avoid wet shaving/waxing/hair removal creams. • Pliazon cream for cetuximab reaction. • Aveeno cream. Secretions • • • • • • • • Most Difficult symptom to manage. Distressing for patient and carers. Causes Halitosis. Unsociable ! Thick tenacious phlegm. Source of infection/aspiration. Maintains healthy PH oral cavity. Main cause or nausea/retching. Mangement • • • • • Good oral hygiene. Regular rinsing…..saline mouth washes. ?? Sodium Bicarbonate Rinses. Steam Inhalation. Nebulisers. Conclusion Promote patient comfort Control Symptoms Complete proposed treatment. Reduce/control pain Avoid admission Holistic Assessment Maintain nutrition intake Avoid Infection Avoid aspiration/maintain safe swallow Psychological support MDT Working Avoid further trauma to skin/oral mucosa