Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
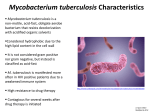
Mycobacterium
Learning Objectives
At the end of this lecture, the student should be able to:
List the important characteristics of Mycobacteria
List
the medically important genera of
Mycobacteria
List the most important epidemiological
properties of Mycobacteria
List the most important diagnostic tests in the
diagnosis of Mycobacteria
List the main properties of the vaccine for
tuberculosis
Mycobacterium
Aerobic bacilli
The rods occasionally form branched filaments
Mycobacterium
Cell wall is rich in lipids
Hydrofobic surface
resistant to many
disinfectants & stains
resistant to decolorizing
“acid-fast bacilli”
Grow slowly (dividing every 12-24 h):
requiring as long as 6-8 weeks before growth is detected in
laboratory
Mycobacterium
Once stained,
the rods also cannot be decolorized with acid
solutions;
hence the name acid-fast bacteria.
Other species of bacteria may also be
acid-fast
Nocardia,
Rhodococcus,
Tsukamurella,
Gordonia
they stain less intensely (are partially acid-fast), and
their mycolic acids chains are shorter.
Mycobacterium
Mycobacteria are a significant cause of
morbidity and
mortality,
particularly in countries with limited medical resources.
Currently, more than 130 species of mycobacteria
have been described, many of which are associated
with human disease
TUBERCULOSIS
kills about 3 million people/year
infects almost 9 million others/year
wherever poverty, malnutrition and poor housing prevail.
It affects the apparently healthy as well as being a
serious disease of the immunocompromised, as has
become particularly obvious in patients with AIDS.
Tuberculosis is primarily a disease of the lungs, but
may spread to other sites or proceed to a
generalized infection ('miliary' tuberculosis).
Infection is acquired by inhalation
of Mycobacterium tuberculosis
in aerosols and dust.
Air-borne transmission of tuberculosis is efficient
because infected people cough up enormous
numbers of mycobacteria,
projecting them into the environment,
where their waxy outer coat allows them to withstand
drying and therefore survive for long periods of
time in air and house dust.
Mycobacterium
Despite the abundance of mycobacterial species, the
following few species or groups cause most human
infections:
M. tuberculosis
M. avium complex
M. kansasii
M. fortuitum
M. chelonei
M. abscessus
M. leprae
Mycobacteria possess
a complex, lipid-rich cell wall
This cell wall is responsible for many of the
characteristic properties of the bacteria:
acid-fastness,
slow growth,
resistance to detergents,
resistance to common antibacterial antibiotics
antigenicity
clumping
Mycobacteria possess
The basic structure of the complex, lipid-rich cell
wall
is of typical for gram-positive bacteria:
an inner plasma membrane overlaid with a thick
peptidoglycan layer and
no outer membrane.
However, the mycobacterial cell wall structure is far
more complex than that in other gram-positive
bacteria.
The proteins in the cell wall:
biologically important antigens, stimulating the
patient's cellular immune response to infection.
Extracted and partially purified preparations of
these protein derivatives (purified protein
derivatives, or PPDs) are used as skin test reagents
to measure exposure to M. tuberculosis.
Similar preparations from other mycobacteria have
been used as species-specific skin test reagents
Mycobacterium
The mycobacterial cell wall is complex,
This group of organisms is fastidious,
Most mycobacteria grow slowly, dividing every 12 to
24 hours
Requiring as long as 8 weeks before growth is detected
in laboratory cultures.
Mycobacterium
Slow-growings
3 to 8 weeks of incubation
Rapid-growings
> 3 days
Non-growing: Mycobacterium leprae
Classification
Growth properties and
Colonial morphology
are used for the preliminary classification of
mycobacteria.
M. tuberculosis and closely related species in the M.
tuberculosis complex are slow-growing bacteria.
The colonies of these mycobacteria are either
nonpigmented or of a light tan color
Mycobacterium tuberculosis colonies grow on
Löwenstein-Jensen agar medium fter 8 weeks of
incubation
Downloaded from: StudentConsult (on 27 April 2009 07:47 AM)
© 2005 Elsevier
Other species of mycobacteria
referred to as
atypical mycobacteria,
mycobacteria other than tuberculosis (MOTT) or
non-tuberculous mycobacteria (NTM)
also cause infection in the lungs
«Nontuberculous mycobacteria» or NTM
Classified originally by Runyon by their rate of
growth and pigmentation
Pigmented mycobacteria produce intensely yellow
carotenoids which may be stimulated by exposure to
light (photochromogenic organisms)
or
produced in the absence of light (scotochromogenic
organisms).
Mycobacterium kansasii colonies grow on Middlebrook agar in
one day after exposure to light.
Downloaded from: StudentConsult (on 27 April 2009 07:47 AM)
© 2005 Elsevier
The Runyon classification scheme
consisted of four groups:
slow-growing photochromogens (e.g., M. kansasii, M.
marinum),
slow-growing scotochromogens (e.g., M. gordonae-a commonly
isolated nonpathogen),
slow-growing nonpigmented mycobacteria (e.g., M. avium, M.
intracellulare),
rapidly growing mycobacteria (e.g., M. fortuitum, M. chelonae,
and M. abscessus).
Currently used methods for the rapid detection and identification
of mycobacteria have made this scheme less important.
Nonetheless, a pigmented or a rapidly growing mycobacterium
should never be mistaken for M. tuberculosis.
M. tuberculosis Complex
M. tuberculosis Strictly pathogenic
M. leprae
M. africanum
M. bovis
M. bovis (BCG strain)
M.microti
M.canettii
M.pinnipedii
Strictly pathogenic
Strictly pathogenic
Strictly pathogenic
Rarely pathogenic
Slow-Growing Nontuberculous Mycobacteria
M. avium complex (MAC): Usually pathogenic
M. kansasii: Usually pathogenic
Rapidly Growing Nontuberculous
Mycobacteria
M. abscessus: Sometimes pathogenic
M. chelonae: Sometimes pathogenic
M. fortuitum: Sometimes pathogenic
Mycobacterium
tuberculosis/Pathogenesis
Virulence
Capable of intracellular growth in
unactivated macrophages
Disease primarily from host response to
infection
M. tuberculosis is an intracellular pathogen that is
able to establish lifelong infection.
Mycobacterium tuberculosis/Diagnosis
Clinical diagnosis +
Radiographic evidence of pulmonary
disease
Positive skin test reactivity
The laboratory detection of mycobacteria
either with
-microscopy
-culture
-molecular methods
Laboratory diagnosis
Tuberculin skin test (TST) and IFN-γ release tests
(IGRA) are sensitive markers for exposure to
organism
Microscopy and culture are sensitive and specific
Direct detection by PCR.
Downloaded from: StudentConsult (on 27 April 2009 07:47 AM)
© 2005 Elsevier
Mycobacterium leprae(Hansen
disease )
Weakly Gram-positive, strongly acid-fast bacilli
Unable to be cultured on artificial media
Diagnosis made with specific skin test or acid-fast
stain
Capable of intracellular growth
Leprosy disease: tuberculoid-lepromatousintermediate forms
Biology, Virulence, and Disease
Lipid-rich cell wall
Disease primarily due to host response to
infection
Tuberculoid (paucibacillary) and lepromatous
(multibacillary) forms of leprosy
Diagnosis
Microscopy is sensitive for the lepromatous form
but not the tuberculoid form
Nasal scrapings and biopsies of skin lesions should
be stained by Ziehl-Neelsen or auramine stain to
demonstrate acid-fast rods.
Skin testing is required to confirm tuberculoid
leprosy
Culture is not useful
Mycobacterium avium Complex
In environment:
Water(fresh, brackish,ocean, drinking water)
Soil
Before AIDS epidemic
Transient colonizer in asymptomatic patients
Disease in patients with compromised
pulmonary function
With AIDS, a new spectrum of disease
“The most common mycobacterial disease”
disseminated
Laboratory Diagnosis of Mycobacterial
Disease
Detection
Skin test
Microscopy
Carbolfuchsin acid-fast stain
Fluorochrome acid-fast stain
Culture
Solid agar-based or egg-based media
Broth-based media
Acid-fast stains of Mycobacterium tuberculosis.
A, Stained with carbolfuchsin
B, Stained with the fluorescent dyes auramine
Downloaded from: StudentConsult (on 27 April 2009 07:47 AM)
© 2005 Elsevier
Laboratory Diagnosis of Mycobacterial
Disease
Identification
Morphologic properties
Biochemical reactions
Analysis of cell wall lipids
Nucleic acid probes
Nucleic acid sequencing
Updated Guidelines for the Use of Nucleic
Acid Amplification Tests in the Diagnosis of
Tuberculosis
Conventional tests for laboratory confirmation of TB include
• acid-fast bacilli (AFB) smear microscopy(24 hours)
• culture
Although rapid and inexpensive,
AFB smear microscopy is limited by its poor sensitivity
(45%–80% with culture-confirmed pulmonary TB cases)
Updated Guidelines for the Use of
Nucleic Acid Amplification Tests in the
Diagnosis of Tuberculosis
NAA tests can provide results within 24–48 hours.
Updated Guidelines for the Use of Nucleic
Acid Amplification Tests in the Diagnosis of
Tuberculosis
Compared with AFB smear microscopy,
the added value of NAA testing lies in its
1) greater positive predictive value (>95%)
with AFB smear-positive specimens in settings
in which nontuberculous mycobacteria
are common and
2) ability to confirm rapidly the presence of M. tuberculosis
in 50%–80% of AFB smear-negative, culture-positive specimens
Compared with culture, NAA tests
can detect the presence of M. tuberculosis bacteria in a specimen weeks earlier
than culture for 80%–90% of patients suspected to have pulmonary TB
whose TB is ultimately confirmed by culture
Culture remains the gold standard for laboratory
confirmation of TB and is required for isolating
bacteria for drug-susceptibility testing and
genotyping.
Routinely collect respiratory specimens (e.g., sputum),
process (liquefy, decontaminate, and concentrate),
and test by AFB smear microscopy and culture as
previously recommended . Specimen collection and
microbiologic testing should not be delayed to await
NAA test results.
The positive predictive value of FDA-approved NAA
tests for TB is >95% in AFB smear-positive cases
If the NAA result is negative and the AFB smear result
is positive, a test for inhibitors should be performed
and an additional specimen should be tested with
NAA. Sputum specimens (3%–7%) might contain
inhibitors that prevent or reduce amplification and
cause false-negative NAA results
Currently available NAA tests are not sufficiently
sensitive (detecting 50%–80% of AFB smear-negative,
culture-positive pulmonary TB cases) to exclude the
diagnosis of TB in AFB smear-negative patients
suspected to have TB
For culture
Sputum: early morning specimen on three consecutive days
Bronchial aspirate,BAL
Gastric lavage
Urine:early morning specimen on three consecutive days
Sterile body fluids(CSF,peritoneal,pericardial,synovial)
Tissue
Abscess contents
Blood
Stool
Should be refrigirated until being processed!
IFN-γ release tests -quantiferon
On May 2, 2005, a new in vitro test, QuantiFERON®-TB Gold (QFT-G,
manufactured by Cellestis Limited, Carnegie, Victoria, Australia), received
final approval from the U.S. Food and Drug Administration (FDA) as an aid in
diagnosing Mycobacterium tuberculosis infection, including both latent
tuberculosis infection (LTBI) and tuberculosis (TB) disease.
This enzyme-linked immunosorbent assay (ELISA) test detects the release
of interferon-gamma (IFN-g) in fresh heparinized whole blood from
sensitized persons when it is incubated with mixtures of synthetic peptides
simulating two proteins present in M. tuberculosis: early secretory antigenic
target--6 (ESAT-6) and culture filtrate protein--10 (CFP-10). ESAT-6 and
CFP-10 are secreted by all M. tuberculosis and pathogenic M. bovis strains.
IFN-γ release tests
QFT-G is expected to be more specific for M. tuberculosis than
tests that use tuberculin purified protein derivative (PPD) as the
antigen.
Tuberculin skin test and IFN-γ release tests are
sensitive markers for exposure to organism
Tuberculin skin test
purified protein derivative (PPD) from the
mycobacterial cell wall
In this test, a specific amount of the antigen (5
tuberculin units of PPD) is inoculated into the
intradermal layer of the patient's skin.
Skin test reactivity (defined by the diameter of the area
of induration) is measured 48 hours later.
A positive skin test indicates previous infection but not
necessarily active disease
Becomes positive 4-6 weeks after infection.
Tuberculin skin test
Additionally, individuals from countries where
vaccination with attenuated M. bovis (bacille
Calmette-Guérin [BCG]) is widespread will have a
positive skin test reaction.
Mycobacteria
are innately resistant to most antibacterial agents,
specific antituberculous drugs have to be used
The number of strains resistant to the first-line
antituberculous drugs has increased
multidrug resistant (MDR) TB
drug susceptibility assay
Tuberculosis
is prevented by improved social conditions,
immunization and chemoprophylaxis
Immunization with a live attenuated BCG (bacille
Calmette-Guérin) vaccine, has been used effectively in
situations where tuberculosis is prevalent.
Immunization, which confers positive skin test
reactivity, does not prevent infection, but it allows the
body to react quickly to limit proliferation of the
organisms. In areas where there is a low prevalence of
disease, immunization has been largely replaced by
chemoprophylaxis.
BCG (bacille Calmette-Guérin)
vaccine
ATTENUATED VACCINE
M.BOVIS IS ATTENUATED BY
Passage for 10 years in glycerol-bile-potato medium
BCG vaccination is now given to approximately 90% of
the world's babies at birth, and protects against the
most severe disseminated forms of tuberculosis such
as TB meningitis in children, even if its effectiveness
against pulmonary TB in adults is more variable
Susceptibility to physical and chemical agents
Survives weeks to months on inanimate objects
protected from sunlight
Chlorine compounds
70% ethanol
2%glutaraldehyde
Peracetic acid
Hidrogen peroxide
Treatment and resistance
Multidrug therapy
Long term
Organism that become resistant to one drug will be
inhibited by the other
Although therapy is given usually for months but the
patient sputum becomes noninfectious within 2 to 3
weeks.