Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
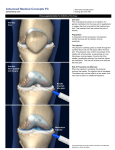
Focus on Clinical Skills Part 1: Advanced Skills to Examine Injuries of the Shoulder, Knee, Back and Ankle Part 2: Injection technique, Pelvic Exam and IUD placement Family Medicine Clerkship – 2014/2015 ***Sources used in Handout: 1. Essentials of Musculoskeletal Care 3rd edition; BMJ 1995, Bandolier 1998. 2. Essentials of Family Medicine 6th edition; LWW 2011. 3. Pfenninger and Fowler’s Procedures for Primary Care 2nd edition; Mosby 2003. Use of a Pressurized Metered-Dose Inhaler 1) Shake the inhaler well immediately before each use 2) Remove the cap from the actuator mouthpiece 3) Breathe out fully through your mouth 4) Place the mouthpiece fully into your mouth, holding the inhaler in a mouthpiecedown position, and close your lips around the mouthpiece, making sure that your tongue does not obstruct the mouthpiece. 5) While breathing in deeply and slowly, depress the top of the metal canister (at the beginning of the breath) 6) Hold your breath for up to 10 seconds 7) Replace the cap on the mouthpiece ** Priming Shake the inhaler well Release 1–4 test sprays into the air, away from your face, before using for the first time or when the inhaler has not been used for more than 3 days. **Clean the actuator or mouthpiece at least once a week. Wash the actuator by rinsing it under running water, shake off the water, and let the device air dry. **Discard the canister after you have used the labeled number of doses. Never immerse the canister in water to determine how full the canister is. Use of a Pressurized Metered-Dose Inhaler with a Valved Holding Chamber (Spacer) **Spacers are used with MDIs. They make the inhaler much easier to use and increase the amount of medication received. 1) Take cap off the pMDI boot and insert into chamber 2) Shake pMDI with chamber 3) Spray 1 dose into chamber 4) Inhale from the chamber for several breaths 5) Slow deep breath with breath hold if possible (adults should do three breaths), or tidal breathing (Infants: ≤10 breaths or 30 seconds tidal breathing) 6) Remove MDI from chamber 7) Replace cap on MDI and chamber 8) Store both chamber and MDI properly **Spacer maintenance: Periodically wash spacer in warm soapy water, rinse, and air dry Use of a Dry Powder Inhaler (DPI), eg Advair, Serevent, Flovent (also comes as an MDI) 1) Open the device 2) Slide the lever to load dose 3) Keep device level 4) Exhale away from device, to residual volume 5) Inhale rapidly and fully 6) Breath-hold, ideally for at least 10 seconds 7) Remove device from mouth and exhale away from device 8) Close the device and store in a cool, dry place Use of a Peak Flow Meter 1) Stand up or sit up straight. 2) Make sure the indicator is at the bottom of the meter (zero). 3) Take a deep breath in, filling the lungs completely. 4) Place the mouthpiece in your mouth; lightly bite with your teeth and close your lips on it. Be sure your tongue is away from the mouthpiece. 5) Blast the air out as hard and as fast as possible in a single blow. 6) Remove the meter from your mouth. 7) Record the number that appears on the meter and then repeat twice. **Calculate predicted peak flow using chart that comes with the meter or an online calculator Nebulizers vs Inhalers When used properly, they are equally efficacious There is ONE reason to use nebulizers over inhalers: the patient is physically unable to use an inhaler (too young, past stroke, tachypneic, etc) The Back I. Lessons from ICM: - Inspection – general appearance (comfort level, leaning forward or backward), deformity, symmetry - Palpation – palpate for tenderness: SI joints, spinous processes, paraspinal muscles and soft tissue - Range of Motion – flexion - 40-60 degrees extension - 20-35 degrees side flexing - 15-20 degrees - Strength – hip flexors, quadriceps, hamstrings, lower leg, great toe. - Neuro Exam - sensory function on medial, dorsal and lateral aspects of the feet. - DTR of patellar and achilles. - walk on heels and toes. - Babinski - positive (upgoing toes) if there is an upper motor neuron lesion (cord compression) Lumbar Neuro Exam Findings: Sensory Loss Motor Screening weakness exam Medial foot Knee extension Squat and rise Herniation Nerve root L3-4 disc L4 L4-5 disc L5 Dorsal foot L5-S1 disc S1 Lateral foot Dorsiflex ankle/great toe Plantarflex ankle/toes Reflex Patellar Heel walking None Toe walking Achilles The RED FLAGS of back pain: These may indicate more serious disease and a more urgent need for imaging, treatment and/or referral. IV drug use h/o osteoporosis h/o cancer chronic steroid use immunosuppression significant trauma fever/chills unexplained weight loss saddle anesthesia urinary retention/incontinence fecal incontinence unrelenting pain at night or pain at rest progressive motor or sensory deficit II. Common injuries/illnesses with associated symptoms & physical exam signs: Lumbar strain/sprain The most common cause of back pain. Symptoms: Lumbar pain that can radiate to the buttocks or legs. Physical Exam: Neuro exam is normal. Typically decreased ROM of spine and soft tissue tenderness. Special Tests – Straight leg raise (SLR) With patient laying supine elevate the symptomatic leg. The test is positive if this reproduces radiating pain down the raised leg at 30-60 degrees. - Reasonably sensitive, not specific for herniation - Crossed SLR is pain on lifting the opposite leg More specific less sensitive Spinal stenosis Typically in older individuals, degenerative changes in the spine. Symptoms: Leg pain, numbness, paresthesias. Pain is better when leaning forward (flexion) Pseudoclaudication - the leg symptoms get worse with exercise. Physical Exam: Sensory loss, muscle weakness Herniated disc = sciatica Symptoms: Pain radiates in dermatomal pattern below the knee. (This is key!). Physical Exam: Potential muscle weakness, sensory loss and/or diminished reflexes. Pain is aggravated by valsalva maneuvers or sitting and is worse with flexion. Cauda equina syndrome Surgical emergency. Most commonly caused by central disc herniations and tumors Symptoms: Bladder dysfunction (urinary retention), bowel incontinence, saddle anesthesia, bilateral neurologic deficits and pain. Physical Exam: Decreased rectal tone, sensory deficits, neurologic deficits Vertebral compression fracture Risk factors include older age, osteoporosis and cancer. Symptoms: Pain is typically worse with activity, palpation over the spine and flexion. Can occur without trauma. Physical Exam: Bony tenderness, increased pain with flexion. When to Image??? - Consider imaging in patients with any Red Flags described above. - Plain x-rays should be used initially to evaluate for tumor, infection and fracture. However, X -rays are not useful for identifying herniated discs. Spondylolysis – a fracture in the pars interarticularis of the vertebrae. Look at the neck of the ‘Scotty Dog’ on plain films L4-L5 Herniated disc on MRI - The initial treatment for a herniated disc is similar to that for lumbar strain: NSAIDS, muscle relaxants, physical activity as tolerated or physical therapy. However, MRI is indicated for patients who have radicular symptoms that have not improved after 6 weeks of conservative treatment. - MRI or CT should be ordered earlier for patients in whom you suspect tumor, infection, cauda equina syndrome or patients with progressive neurologic deficits Osteolytic lesions from metastatic disease The Shoulder I. Lessons from ICM: - Inspection – symmetry, muscle atrophy, swelling, erythema, ecchymosis - Palpation – AC joint, subacromial bursa, coracoid process, long head of the biceps tendon - Range of Motion – flexion/elevation 160-180 degrees, adduction, abduction, external and internal rotation 90 degrees - Strength – deltoid, biceps, infraspinatous/teres minor, supraspinatous, serratus anterior Range of Motion II. Common injuries with associated symptoms & physical exam signs: AC Joint Separation Symptoms: pain and deformity over superior aspect of shoulder after falling directly on shoulder Physical Exam: Palpation of AC joint – any abduction causes pain Cross body adduction to assess for arthritis of AC joint Arm is forward flexed to 90 degrees and then horizontally adducted as far as possible – positive is pain over AC joint Shoulder Dislocation (joint separation)/Subluxation (sensation of ‘slipping’) Described by the direction of the humerus in relation to the glenoid fossa (anterior vs posterior) Traumatic dislocations are >90% anterior dislocations. Symptoms: sensation of shoulder slipping out of joint with initial insult being fall or forceful throwing motion but simple changes in position may provoke subsequent dislocation. Physical Exam: Apprehension test: place arm in 90 degrees abduction with elbow at 90 degrees and then maximally externally rotate the humerus. Checks for anterior instability. Sulcus Sign – more than 2cm is typically positive for glenohumeral instability Rotator Cuff Syndrome = Impingement Syndrome/Rotator Cuff tendonitis/Subacromial bursitis Typically starts as mild inflammation of the bursa or rotator cuff tendons and can progress to chronic pain, decreased range of motion and rotator cuff weakness. When severe can progress to a partial thickness or full thickness tear. Symptoms: The symptoms are secondary to repeat mechanical insult as rotator cuff tendons pass under the coracoacromial arch consisting of coracoid process, the coracoacromial ligament, the acromion, and AC joint capsule. Uncommon in young patients and often co-exists with adhesive capsulitis (frozen shoulder). Chronic pain can be referred to lateral deltoid region and exacerbated by overhead activities. May cause night time pain which makes sleeping on affected side difficult. Over time the humeral head migrates superiorly compressing the bursa and the rotator cuff tendons against the acromion, causing impingement. Coracoacromial arch (in yellow) Physical exam: Assess for muscle atrophy and weakness Neer impingement sign: depress scapula with one hand while lifting arm with other Hawkins impingement sign: abduct arm 90, flex elbow, internally rotate humerus Isolate muscles of the rotator cuff: Isolate supraspinatous with arm in same position and thumbs down and push down Isolate Infraspinatous and teres minor with arms down and elbows extended resisting external rotation Isolate subscapularis with lift off hand behind back with palm away from body. Rotator Cuff Tear Symptoms: Weakness and loss of active elevation and external rotation. Physical exam: Significant weakness when muscles of rotator cuff are isolated Muscle atrophy depending on time course of injury Cases: 1- A 22 year old male presents to your office complaining of right shoulder pain. He is a baseball pitcher for a neighborhood league and has been having increasing pain after games. It is difficult to lift his arm to the side and he complains of pain more on the outside of his shoulder. He is unable to sleep on his right side. Exam findings? Diagnosis? Treatment? 2- A 32 year old female presents to your office complaining of right shoulder pain. She was playing basketball and fell, landing on her shoulder. She did not hear a ‘pop’ and can still move the arm but it hurts, especially on the ‘top of the shoulder’. Exam findings? Diagnosis? Treatment? The Knee: I. Lessons from ICM: - Inspection – symmetry, valgus/varus, atrophy, swelling, erythema, ecchymosis, gait - Palpation – effusion, patellar tendon and ligament, joint line, pes anserine bursa, tibial tuberosity, popliteal fossa, warmth - Range of Motion – (active and passive) flexion 135-145 degrees, extension to 0 degrees (flat) - Strength – quadriceps, hamstrings Range of Motion II. Common injuries with associated symptoms & physical exam signs: Fractures, especially patella: Symptoms: significant pain after blunt trauma or a fall Physical Exam: Swelling and significant pain apply Ottowa rules (see appendix) Patellar Dislocation Symptoms: acute onset of pain after sudden movement or contraction of the quads when decelerating quickly (especially in sports) Physical Exam: Pain and swelling that occurs within hours of the dislocation The patella usually relocates once the leg is straightened making the dx more difficult Typically a lateral displacement as the vastus lateralis is stronger than vastus medialis Patellar Apprehension Test: displace patella laterally and flex knee to 30 degrees Meniscal injuires: Symptoms: usually caused by trauma in the young, older pts require less force for injury. Locking sensation after twisting injury Physical Exam: Joint line tenderness Valgus vs Varus stress – can tell you the location of injury McMurrays: external rotation in flexion then extend to stress medial meniscus, then do same with internal rotation to stress lateral meniscus Collateral Ligament injury Symptoms: trauma from the side (medial or lateral) Physical exam: Valgus stress to test MCL and Varus stress to test LCL both with knee flexed 25 degrees Anterior Cruciate Ligament injury: (sprain vs rupture) Symptoms: popping sound at time of injury, immediate tense effusion Physical exam: Lachman: pull anterior on tibia while knee is flexed 25 degrees Anterior Drawer test: less sensitive than Lachman. Pull tibia forward at 90 degree flexion Patellar Tracking Syndrome Symptoms: pain behind the patella, gritty sound or feeling when moving the patella Physical Exam: Caused by wear on the back of the patella, asymmetry of the posterior surface Pain with quadriceps contraction while pushing patella toward the femoral groove Osgood-Schlatter Disease Symptoms: occurs generally in rapidly growing adolescents Physical Exam: Tenderness over the tibial tuberosity Cases: 1- A 78 year old male presents to your office for left knee pain. He has been working in the garden lately and yesterday when he stood up from a kneeling position he felt a sharp pain in the knee. Now the knee is slightly swollen and has a clicking sensation when he bends it. He has always had arthritis in that knee, but this is a new type of pain. Exam findings? Diagnosis? Treatment? 2- A 30 year old female presents with left knee pain. She was playing soccer and fell, twisting her knee. The knee is swollen and very painful. She comes to your office on crutches. Exam findings? Does this patient need an xray? The Ankle and Foot I. Lessons from ICM: Inspection - swelling, erythema, ecchymosis, alignment of heels, toes, high arches or pes planus, calluses, gait (intoeing, outtoeing, limp) - Palpation - medial and lateral malleoli, Achilles tendon, plantar fascia - Range of Motion - zero starting position is with the foot perpendicular to the tibia Range of Motion II. Common injuries with associated symptoms & physical exams: Fractures vs Sprain Ankle sprains are the most common injury in sports. 85% of sprains involve the lateral ligaments. The weakest lateral ligament is the anterior talofibular ligament. Symptoms: Pain, swelling and inability to bear weight comfortably. Ankle “gives out”, typically rolls laterally. Physical Exam: Ankle sprain is a clinical diagnosis. Apply Ottowa rules (see appendix) Anterior Drawer test: grasp hindfoot and pull forward with 20 degrees of plantar flexion to assess anterior talofibular ligament (remember, the weakest of the lateral ligaments) This test is most sensitive about 4 days after injury as pain improves. Talar Tilt test: when foot is in plantarflexion this tests the anterior talofibular ligament. When foot is in neutral flexion it tests the calcaneofibular ligament. Reverse Talar Tilt test: tests the deltoid ligament for medial ankle sprains Syndesmotic Sprain – High ankle Sprain These sprains generally occur when the ankle is externally rotated and hyperdorsiflexed (like being tackled). Symptoms: Patients will have pain but less swelling than a lateral ankle sprain. Physical Exam: Tenderness over the anterior inferior tibiofibular ligament and interosseous membrane. Squeeze test: squeezes the tibia and fibula putting pressure on the interosseous membrane Plantar Fasciitis: The most common cause of heel pain in adults. Caused by repetitive microtears in the plantar fascia. Little or no inflammation involved. Symptoms: Pain in the heel, worse with the first few steps in the morning or after rest. Improves with walking. Occurs more commonly in patients with flat feet or high arches. Physical Exam: Diagnosed clinically, typically no need for xrays. Pain is worse when standing on tip toes. Heel Spurs DO NOT cause this pain and don’t need to be removed. Maximal pain is at the medial tubercle on the plantar aspect of the calcaneus. Achilles Tendonosis: Risk factors include running, overuse, increase in hill running, decreased calf and hamstring flexibility Symptoms: Pain related to activity that is localized to the Achilles tendon. Typically the patient has had a change in shoes or an increase in training intensity Physical Exam: Tenderness and swelling about 3-4 cm above the insertion of the tendon at the calcaneus. If concerned about tendon rupture – while the patient is sitting, squeeze the calf and there should be reflexive plantar flexion. If there is no flexion there is concern for a complete tear. Tarsal Tunnel Syndrome: Entrapment of the tibial nerve in the tarsal tunnel (the space behind the medial malleolus covered by the flexor retinaculum. Can be caused by chronic ankle sprains, fractures, dislocations, repetitive stress, flat feet. Symptoms: Heel pain, paresthesias (tingling) around the medial aspect of the heel Worse with weight bearing and walking Physical Exam: Pressure or tapping over the posterior tibial nerve reproduces symptoms (Tinel’s sign). EMG and nerve conduction studies confirm the diagnosis. Hallux Valgus (Bunions): Lateral deviation of the great toe with respect to the 1st metatarsal Treatment includes wider shoes, padding the area to avoid direct pressure, arch supports, and surgery. Symptoms: Pain on the medial aspect of the forefoot Worse with tight fitting shoes Physical Exam: Red, swollen, painful area on the medial aspect of the 1st metatarsal head Morton’s Neuroma: Interdigital neuroma typically in runners and dancers. Caused by entrapment of the plantar nerve between the metatarsal heads – usually between the 3rd and 4th toes. Treatment includes metatarsal pads, arch supports, steroid injections and surgery. Symptoms: Numbness and tingling in toes and burning in the distal forefoot Made worse by tight fitting shoes, walking on hard surfaces The patient can occasionally feel a “painful ball” between the metatarsal heads Physical Exam: Occasionally the neuroma can be palpated between the 3rd and 4th metatarsal heads. Palpating the area of pain and squeezing the forefoot at the same time will worsen the pain. Jones Fracture: A fracture of the 5th metatarsal occurring and the diaphyseal-metaphyseal junction. (near the base of the metatarsal) Symptoms: Typically a results of forced adduction of the forefoot. Commonly occur in soccer and football players. Sudden pain in the lateral forefoot. Physical Exam: Localized tenderness over the fracture site. Cases: 1- A 48 year old female marathon runner presents with right ankle pain. She has been intensifying her training schedule over the past few days and has noted a gradual worsening of the pain. The pain is worse at the beginning of a run, resolves after a mile or two and also resolves with rest. Exam findings? Does this patient need an xray? 2- A 19 year old male presents to your office with ankle pain. He was at a football game the night before and tried to jump off the side of the bleachers, landing on his left ankle. He can’t bear weight on it and is worried it might be broken. Exam findings? Does this patient need an xray? Large Joint Injections I. Risks of Steroid Injections – increased risk with repeated injections - infection (very rare) - steroid flare causing worse pain for 24 hours - bleeding (rare) - failure to obtain relief - skin atrophy, depigmentation and/or slight indentation - increase glucose levels in diabetics for 24 hours II. Indications - Osteoarthritis - Crystal arthritis - Bursitis - Tenosynovitis/tendonitis - Costochondritis III. Procedure - Draw up 5-10 ml lidocaine/marcaine with 1 ml steroid (usually 40mg triamcinalone or methylprednisolone) - Identify the entry site (use landmarks!) and mark it (thumbnail or a pen) - Clean area with alcohol or povidone-iodine - May use ethyl chloride spray for 1-2 seconds for anesthesia - Insert needle, pull plunger to make sure you aren’t in a vessel, then inject - Remove the needle slowly IV. Knee - Intra-articular Injection – typically used for relief of pain caused by degenerative disease (osteoarthritis) – 21 gauge needle, 1 ½ inch o Patient is either lying down with knee flexed and towel underneath for support or seated with knee flexed at 90 degrees. o The joint space is large and can be entered from several directions. o Anterior approach – (best used with patient seated) Insert the needle at the medial or lateral border of the patellar tendon. Direct the needle toward the center of the knee, insert about 1 ½ inches, the medication should flow easily. o Lateral approach – (best used with patient supine) Locate the superior lateral margin of the patella and insert the needle 1cm superior and lateral to this point. - Aspiration – indicated for relief of pain caused by an effusion or diagnostic purposes using fluid analysis (gout, infection etc) - 18-22 gauge needle, 1 ½ inch, 60-mL syringe o The lateral approach used above is also used for aspiration. o If infection is not suspected the needle can be kept in place after aspiration and a new syringe containing the steroid can be injected through the same needle. o After aspiration of a tense effusion, apply compression dressing to prevent recurrence. - Anserine Bursa – indicated for bursitis – 25 gauge needle, 5/8 inch o The bursa lies beneath the common insertion of the sartorius, semitendinous, and gracilis tendons on the medial aspect of the tibia. o Locate the point of maximal tenderness. o Insert the needle perpendicular to the tibia. o When you hit the bone, withdraw 2-3mm and inject - Iliotibial Band Syndrome – injection is done to relieve the inflammation caused by the IT band as it crosses the lateral femoral condyle – 25 gauge, 5/8 inch o Locate the lateral femoral condyle and Gerdy’s tubercle on the anterolateral tibia o Identify the point of maximal tenderness o Insert the needle angled posterior, avoiding the IT band itself. o The intent is to inject the medication between the IT band and the epicondyle. V. Shoulder - AC Joint – 25 gauge needle, ½ to 1 inch o Follow the clavicle laterally until you reach a prominence, about 1.5-2cm inward from the lateral edge of the acromion o Pushing down on the distal clavicle while your finger is on the AC joint will help verify the location o Insert needle from anterior/superior position and angle medially - Intraarticular shoulder – for osteoarthritis – 25 gauge needle, 1 ½ inch Anterior approach – (star) rotate shoulder outward, palpate the coracoid process and insert needle 1cm inferior and 1cm lateral to coracoid process. Direct the needle slightly laterally. It should not hit bone. Posterior approach – arm is resting at side, medially rotated. Find the inferior-posterior aspect of acromion with thumb, find coracoid process with index finger. Insert needle below acromion and aim for coracoid process. - Subacromial Bursa – typically used for bursitis – 21 gauge needle, 1 ½ inch o Locate the posterolateral edge of the acromion and find the soft spot between that edge and the head of the humerus (about 1 inch inferior). That is the subacromial bursa. o Direct the needle perpendicularly and insert through the deltoid and into the bursa (approx 1-1 ½ inches). The medication should flow in easily, if not you may be in too far and should withdraw the needle slightly. Basic Injection Technique I. Intramuscular injections – ‘IM’ - Indications – typically used for drugs of greater volumes or that are not very soluble o Immunizations – Gardasil (HPV), Hepatitis A and B, Hib, DTaP o Medications – prednisone, naloxone, penicillin - Contraindications o Thrombocytopenia, coagulopathy – can lead to hematomas - Locations – the goal is to minimize the chance of hitting a nerve or vessel o Middle third of deltoid o Upper outer quadrant of buttock o Anterior lateral surface of thigh - Procedure o Use a needle at least 1 inch long o Prepare the syringe, depress the plunger to remove any air o Clean the skin with alcohol o Quickly insert the needle at a 90 degree angle through the skin and into the muscle o Draw back on the plunger to verify that the needle is not in a vessel. If you get immediate blood return, withdraw and start over with a new needle. (when injecting immunizations it is not necessary to draw back on the plunger) o Smoothly inject and withdraw the needle o Apply a band-aid if necessary II. Subcutaneous injections – injections into the loose subcutaneous tissue just under the epidermal and dermal layers - ‘SC’ - Indications – volumes of less than 2cc, non-irritating drugs o Immunizations – MMR, varicella, zoster o Medications - Insulin - Locations – fatty areas are best o Upper arm o Abdomen o Lateral thigh - Procedure o Use a needle 3/8 to 5/8 inches long o Prepare the syringe, depress the plunger to remove any air o Clean the skin with alcohol o If necessary gently pinch up the skin to avoid injecting into the muscle o Insert the needle at a 45 degree angle (again to avoid injecting into muscle) o Smoothly inject and withdraw the needle Subcutaneous Injection Sites Intramuscular Injection Sites Cryotherapy I. Indications - Actinic keratoses - Skin tags - Warts - Seborrheic keratoses - Condyloma - Hypertrophic scars - Basal cell CA II. Advantages - Minimal scarring - No anesthesia - No skin preparation - No sutures - Infection is rare III. Disadvantages - Complete healing may take 6-8 weeks - Loss of pigment possible - No tissue to send for pathology - Cannot use in area of poor circulation - Can cause peripheral neuropathy if adjacent nerve is frozen - Sun damaged skin, newborn skin, elderly skin are all more sensitive to freezing IV. Materials - Liquid nitrogen - Oranges (for today’s exercise) V. Procedure - Debride the keratin cover if possible (especially on warts). - Apply water soluble gel over the lesion to help freeze more evenly. - Apply the tip of the liquid nitrogen canister directly on the lesion. - Freeze the tissue until the ice ball extends 2-3mm beyond the benign lesion and 5mm beyond the premalignant or malignant lesion. - It should take 2-3 minutes for a benign lesion to completely thaw and 3-5 min for malignant. - After complete thawing, freeze again. The Pelvic Exam I. Typically consists of external exam, pap smear and bimanual exam II. Indications - Screening - Abdominal pain - Pelvic pain - Abnormal vaginal discharge - Abnormal vaginal bleeding - Genital lesions or rashes III. Preparation - Discuss exam with patient fully clothed o Ask about previous exams – first exam? previous difficulties? o Explain each part of the exam and the equipment o The exam should not be painful! o Some light spotting is normal after a pap smear o Allow her to dress in private, offer tissues if necessary o Explain how she will be notified of results - Materials o Gloves (non-sterile) o Speculum with light (various sizes, warmer?) o Water-soluble lubricant o Large cotton swabs o Spatula and endocervical brush o Culture/swabs for infections if necessary IV. External Exam - The patient should be positioned comfortably all the way at the edge of the table with her feet in stirrups and knees bent and relaxed to the sides. - Vulva– look for any skin changes, erythema, lesions, nodules - Reassure patient if everything looks normal (use the word normal!) V. Bimanual Exam – Typically done after the pap smear - Evaluate for smooth cervix, cervical motion tenderness, smooth uterus, uterine position and size, adnexal tenderness, masses Cervical Cancer Screening I. Typically use ThinPrep method and not Pap smear II. Procedure - Small amount of water soluble lubricant on warmed speculum - Use one hand to gently separate the labia, insert the speculum at an angle, then straighten and aim posteriorly at 45 degrees. - Examine the vaginal walls for lesions, discharge, healthy mucosa - For redundant mucosa – make a speculum sleeve from a glove finger cut at both ends - Visualize the cervix. Check for inflammation, discharge, lesions - Identify cervical landmarks (see appendix) - Attempt to sample the entire transformation zone and endocervical canal using either a spatula and brush or the broom Consider cervical sampling for gonorrhea and chlamydia IUD Insertion I. Indications - Contraception - per American College of Obstetricians and Gynecologists (ACOG) candidates for IUD are . . . - multiparous and nulliparous women at low risk for STIs - women who desire long-term reversible contraception - women with the following medical conditions: diabetes, thromboembolism, menorrhagia/dysmenorrhea, breastfeeding, breast cancer, and liver disease - Menorrhagia/dysmenorrhea II. Contraindications - acute pelvic inflammatory disease (PID) - mucopurulent cervicitis - current high risk sexual behavior (multiple partners, no condoms) - suspected uterine or cervical cancer III. IUD Advantages - High efficacy - Decreases risk of ectopic pregnancy - Long duration of effect - Convenient - Low risk of side effects - Cost effective - Levonorgstrel IUD reduces blood loss with menses and can be used to treat menorrhagia IV. IUD Disadvantages - Menstrual irregularities (heavier menses with copper IUD, irregular bleeding and light spotting with copper or Levonorgstrel IUD are possible) - Cramping at time of insertion - Expulsion - 2-10% are expelled within first year - Perforation at time of insertion. Risk with a skilled operator is less than 1 per 1000 insertions. - Infection - risk is extremely low V. Patient Visit - Discuss risks and benefits of IUD - Consent form - Discuss past medical history - Pelvic exam with bimanual exam and cervical cultures for gonorrhea/chlamydia, Pap if due VI. IUD Insertion - Materials Nonsterile gloves, lubricant, betadine and large swabs Sterile gloves, speculum, tenaculum, uterine sound, IUD, scissors - Procedure Bimanual exam to determine position of uterus Insert speculum and locate cervix Use large swabs and betadine to thoroughly clean cervix 3 times Grasp anterior lip of cervix horizontally with the tenaculum - close slowly to one click Place light tension on tenaculum and insert uterine sound until resistance is felt at the fundus Note the distance in cm on the sounding device - should be 6-9cm. Change to sterile gloves Copper IUD – ParaGard - Use sterile gloves to fold the IUD arms back into the inserter. Insert the rod into the insertion tube from the bottom until it touches the IUD - After sounding the uterus, hold the inserter next to the sound and move the flange to the sounding depth - Hold traction on the tenaculum and insert the IUD until resistance is felt at the fundus - the flange should now be at the external os - Let go of the tenaculum, hold the rod with one hand and withdraw the inserter tube 1/2 inch to release the IUD arms - Gently push the inserter tube to the top of the fundus to ensure fundal placement of the IUD - Hold the inserter tube stable and withdraw the white rod. - Remove the inserter tube - Cut the strings to 2-3 cm - longer is better because you can always cut them shorter! Levonorgstrel IUD – Mirena - After sounding the uterus, use sterile gloves to release the strings on the inserter - The slider should be in the position farthest from you - Align the arms of the IUD so they are horizontal - Pull on the threads to draw the IUD into the insertion tube and fasten the threads tightly in the groove at the end of the tube - Hold the inserter tube next to the uterine sound and move the flange to the sounding depth - Hold traction on the tenaculum and insert the IUD until the flange is 1 1/2 or 2cm from the external os. (note difference from Copper IUD insertion) - Hold the inserter steady and pull the slider back to the mark to release the arms of the IUD - Advance the inserter until the flange is at the external os to ensure fundal placement of IUD - Holding the inserter steady, pull the slider all the way back to release the strings and withdraw the inserter (careful not to pull out the IUD) - Cut the strings to 2-3 cm V. Post Insertion - Schedule visit at 6-8 weeks for string check - Instruct patient on how to check IUD strings - Review signs of infection, expulsion - Remind that spotting can be expected for several months and is normal. Cramping on day of insertion can be treated with NSAIDS Wet Prep/KOH I. Indications - vaginal discharge - vaginal or vulvar pain - abnormal vaginal secretions II. Materials Speculum Normal saline in small test tube Small cotton tipped applicators 10% KOH solution Glass slides and coverslips Microscope pH test tape - results may be invalid if blood, semen or douche solution is present III. Procedure While speculum is in place, obtain a sample of the vaginal secretions by rubbing a cotton-tipped applicator over the vaginal walls and in the fornices. Place the applicator in the test tube with normal saline – keep it there until you are ready to prepare the slides. Remove the speculum Prepare the wet prep in the laboratory using 2 separate slides Place one drop of fluid on one slide and cover with cover slip Place one drop of fluid on the other slide and add a drop of KOH solution, then put the coverslip on top Examine under low and high power IV. Slides - Saline – look for lactobacillus (normal vaginal flora), leukocytes, trichomonads, clue cells (large epithelial cells with indistinct borders and adherent coccobacilli organisms) - KOH – look for hyphae, budding spores, leukocytes vs squamous cells (if WBCs > squamous cells suspect inflammation) Differential Diagnosis for Vaginitis Clinically Normal Bacterial Vaginosis Candidiasis no complaints increased discharge, bad odor that is worse after discharge, intense intercourse, possible itching and burning itching Trichomonas discharge, bad odor, vulvar itching, dysuria white/clear, looks like sometimes increased - increased discharge Discharge typically increased - thin, egg whites during thick, white, 'cottage thin, frothy, (typically) white ovulation cheese like', yellow/green Whiff test (amine odor) none positive (fishy odor) none might be positive pH < 4.5 > 4.5 4-5 > 4.5 (typically > 6) clue cells , no WBC 6. budding yeast on KOH 7. hyphae increased WBC to >10 per high power field, trichomonad organisms Microscope 1. lactobacilli 2. epithelial cell Appendix: Ottawa knee rules In most situations a knee x-ray is not needed for knee injury patients in the absence of the following findings: age 55 or over isolated tenderness of the patella (no bone tenderness of the knee other than the patella) tenderness at the head of the fibula inability to flex to 90 degrees inability to weight bear both immediately and in the office/ED (4 steps - unable to transfer weight twice onto each lower limb regardless of limping). Ottawa ankle and foot rules: Sensitivity of almost 100%, reduces unnecessary Xrays by 30-40% An ankle x-ray is generally required only if there is any pain in malleolar zone and any of these findings: bone tenderness at A bone tenderness at B inability to weight bear both immediately and in the office/ED. A foot x-ray is required if there is any pain in the midfoot zone and any of these findings: bone tenderness at C bone tenderness at D inability to weight bear both immediately and in the office/ED. Vocabulary Bursa – fluid filled sack that helps to decrease friction – e.g. between a tendon and bone Dislocation – complete displacement of a joint Subluxation – partial displacement of a joint Sprain – stretching of a ligament Strain – stretching and damage to a muscle or tendon External rotation – movement away from the center of the body Internal rotation – movement toward the center of the body Eversion – turning outward Inversion – turning inward Abduction – moving away from the midline Adduction – moving toward the midline Valgus – abnormal displacement of a limb or joint away from the midline (valgus stress of the knee is so named because of the direction of the force applied – which is away from the midline) Varus – abnormal displacement of a limb or joint toward the midline