Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
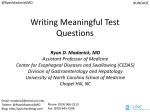
ALIMENTARY SYSTEM WORKSHOP Case I A 44 year-old man was admitted to hospital with haematemesis which was red and contained clots. He had been referred to hospital in the recent past because of epigastric pain and occasional melaena, and was on the waiting list to have investigations regarding this. The patient had a history of significant alcohol intake. He was not on any medication. On examination, he was very obese (weight 177kg). Vital signs were stable. Question 1. Basically what does this patient have? Answer: Question 2. What is the significance of red haematemesis? Answer: Question 3 What is melaena? Answer: Question 4 What does the epigastric pain suggest might be the location and cause of the bleeding? Answer: Question 5 What does the history of excess alcohol suggest could be the cause of the bleeding? Answer: Question 6 Why was it important to elicit a history of medication in this particular case? Answer: Question 7 The patient was very obese. What condition is associated with obesity which could give rise to bleeding? Do you think this obesity could be an adverse factor in his recovery? Answer: Question 8 Now list the causes of acute upper gastrointestinal haemorrhage in order of frequency. Begin with the most common! What do you think this patient had? Answer: The patient underwent emergency oesophago-gastric-duodenoscopyand a large deep chronic ulcer was seen in the first part of the duodenum. At the time of OGD it was not bleeding. The patient was managed conservatively but a further massive haematemesis occurred. The patient’s haemoglobin fell to 2.2 g/dl. Repeat OGD showed the ulcer to be actively bleeding. Sclerotherapy failed to stop the bleeding and a laparotomy was performed to undersew the ulcer. This was an extremely difficult procedure owing to his gross obesity. Shortly after surgery further haemorrhage occurred. A second laparotomy was performed, a gastrojejunostomy done and the patient transferred to a tertiary referral hospital. He was now hypotensive, anuric and markedly hypoxic and acidotic. In total he had been transfused 99 units of r.b.c. and as many units of other blood factors. It was suspected that he had developed disseminated intravascular coagulation (DIC). The patient died a few minutes after arrival in the hospital. At post-mortem examination, a large duodenal ulcer was present with an eroded artery in the base. About 4 litres of blood distended the stomach and there was blood throughout the small intestine and melaena stool in the colon. There was chronic gastritis in the stomach on microscopy. The heart was markedly overweight (670 gram). The lungs were markedly overweight (well over 1000 grams each). Microscopically the kidneys showed acute tubular necrosis and small fibrin thrombi in glomerular capillaries consistent with shock and DIC respectively. Question 9 What is the morphological distinction between an acute ulcer and a chronic ulcer? Answer: Question 10 What is the morphological distinction between a benign and a malignant ulcer? Answer: Question 11 What is the difference between a gastric erosion and a gastric ulcer? Answer: Question 12 Where do most peptic ulcers occur? Question 13: What are the complications of peptic ulcer? Answer: Answer: Question 14: What are the causes of chronic gastritis? What are the likely causes in this patient? Answer: Question 15 What might be the cause of the cardiomegaly? Answer: Question 16 The patient had hypovolaemic shock due to massive gastrointestinal haemorrhage. Renal failure evidenced by anuria and due to acute tribular necrosis was present. What might be the cause of the hypoxia? Answer: Question 17 What is disseminated intravascular coagulation (DIC)? Answer: Case 2 A 72 year-old woman was referred by her G.P. for investigation of iron deficiency anaemic. Apart from lethargy, she had no symptoms, had a normal diet and was not on any medication. Physical examination was normal. Upper gastrointestinal tract endoscopy was normal and a mucosal biopsy of the duodenum was reported as normal by the pathologist. Colonoscopy revealed a fungating, ulcerated tumour in the caecum and a nearby polyp. The pathologists’ report on the resected specimen indicated a moderately differentiated adenocarcinoma invading the full thickness of the wall and extending into the peri-caecal tissues. Four of 16 regional lymph nodes contained metastatic tumour. TNM staging, T3, N2, Mx (Dukes C) Question 1 What do you conclude from: a) The dietary history b) The negative history of medications c) The normal duodenal mucosa? Answer: Question 2 What is the most common cause of iron deficiency anaemia in men and post-menopausal women in the Western world? Answer: Question 3 How does the clinical presentation differ between right-sided and left-sided colonic cancer? Answer: Question 4 Where would you look first for possible blood-borne metastases in this patient? Answer: Answer 1 Acute upper gastrointestinal haemorrhage. This is the most common gastrointestinal emergency. Back Answer 2 This indicates profuse haemorrhage. Shock is likely to develop and may already be present on admission. Mortality is approximately 10% Vomiting of black “coffee grounds” indicates less severe bleeding and time for the digestive action of gastric acid and enzymes to have acted on haemoglobin. Back Answer 3 Melaena is the passage of black tarry stools which contain altered blood due to digestive enzyme and bacterial action on haemoglobin. It is usually due to upper gastrointestinal haemorrhage. Back Answer 4 Epigastric pain raises the possibility of gastroduodenal disease, especially if there is dyspepsia and relationship to food (not elicited in this case), and of the presence of a peptic ulcer. Back Answer 5 Excess alcohol in the short term could cause gastric erosions or vomiting followed by a Mallory-Weiss tear of the oesophagus. In the long term, alcoholic cirrhosis is a cause of oesophageal varices. All thesethose conditions can result in severe haemorrhage. Back Answer 6 Drugs such as NSAIDS are important causes of gastric erosions and peptic ulcer with ensuing haemorrhage. Back Answer 7 Obesity is associated with the development of hiatus hernia and reflux oesophagitis, the latter being a possible cause of acute haemorrhage once ulcerated. Obesity also makes a patient a poor operative risk as will be seen subsequently Back Answer 8 Peptic ulcer Gastric erosions Oesophagitis Oesophageal varices Mallory-Weiss tear Vascular formations Cancer of stomach or oesophagus due to H.pylori or NSAIDS due to alcohol or NSAIDS (usually with hiatus hernia) (liver cirrhosis or portal vein thrombosis) due to retching (35 – 50%) (10- 20%) (10%) (2 – 9%) (5%) (5%) (2%) * Please note that the answer continues for the next three pages. Figure 17-18 Peptic ulcer of the duodenum. Note that the ulcer is small (2 cm) with a sharply punched-out appearance. Unlike cancerous ulcers, the margins are not elevated. The ulcer base is clean. (Courtesy of Robin Foss, University of Florida, Gainesville, FL.) Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 14 November 2005 09:07 PM) © 2005 Elsevier The ulcer at the right is penetrating through the muscularis and approaching an artery. Erosion of the ulcer into the artery will lead to another major complication of ulcers-hemorrhage. This hemorrhage can be life threatening. Chronic blood loss may lead to an iron deficiency anemia. Here are some larger areas of gastric hemorrhage that could best be termed "erosions" because the superficial mucosa is eroded away. Such erosions are typical for the pathologic process termed gastropathy, which describes gastric mucosal injury without significant inflammation. The findings here fit with acute erosive gastropathy, but there are other patterns. Etiologies for the various gastropathies can include: alcohol, drugs such as NSAIDS, stress, uremia, bile reflux, portal hypertension, radiation, and chemotherapy. At the lower end of the esophagus (which has been turned inside out at autopsy) are linear dark blue submucosal dilated veins known as varices. In patients with portal hypertension (usually micronodular cirrhosis from chronic alcoholism), the submucosal esophageal veins become dilated (form varices). These varices are prone to bleed. Gastric neoplasia is not uncommon. Here is a gastric adenocarcinoma. •In the U.S., most gastric cancers are discovered at a late stage when the neoplasm has invaded and/or metastasized. ALL gastric ulcers and ALL gastric masses must be biopsied, because it is not possible to tell from gross appearance alone which are benign and which are malignant. In contrast, virtually all duodenal peptic ulcers are benign. Back Answer 9 The presence of fibrosis in the base of a chronic ulcer Back Answer 10 A benign ulcer appears “punched out” and has not heaped up margins. A malignant ulcer has heaped up margins. Size and location within the stomach do not distinguish a benign from a malignant ulcer. Back Answer 11 An erosion does not penetrate below the muscularis mucosa, an ulcer does. This distinction would apply throughout the gastrointestinal tract. Back Answer 12 At least 98% of ulcers occur in the first part of the duodenum, usually in the anterior wall, or in the antrum of the stomach, usually on the lesser curve. Duodenum: stomach ratio 4:1. Back Answer 13 Bleeding most frequent; occurs in 15% to 20% of patients: accounts for 25% of deaths. Perforation occurs in 5% of patients; accounts for 75% of deaths as a result of peritonitis Penetration this refers to direct erosion of the ulcer into an adjacent organ such as the pancreas Gastric outlet obstruction due to oedema or fibrosis narrowing the pyloric area Back Answer 14 The most common cause of chronic gastritis is H. pylori infection. Almost certainly present in this patient, but cannot be demonstrated histologically in post mortem material Gastritis is often accompanied by infection with Helicobacter pylori. This small curved to spiral rod-shaped bacterium is found in the surface epithelial mucus of most patients with active gastritis. The rods are seen here with a methylene blue stain. Other causes include alcohol (a factor in this patient), cigarette smoking, autoimmune mechanisms (as in pernicious anaemia), post partial gastrectomy (bile reflux), gastric outlet obstruction and uraemia Back Answer 15 Alcoholic cardiomyopathy is a likely cause. Hypertension would be a much more common cause but there was no history of this. The cardiac valvesvalues were normal. Back Answer 16 Adult respiratory distress syndrome (ARDS) or “shock lung” was suspected clinically. No evidence was found at autopsy; i.e. no diffuse alveolar damage or hyaline membranes were seen. There was, however, gross pulmonary oedema which was most likely multifactorial. Back Answer 17 DIC is a thrombohaemorrhagic disorder complicating a variety of diseases. In this case it was due to a combination of tissue injury (sclerotherepy, extensive surgery) and shock. Activation of the coagulation cascades leads to microthrombi throughout the microcirculation with consumption of platelets, fibrin and coagulation factors, and secondarily activation of fibrinolytic mechanisms (hence the term “consumptive coagulopathy”). As a result there is the strange combination of thrombosis and a haemorrhagic disorder. Back: Case 2 Answer 1 a) Dietary deficiency is not the cause of the anaemia. It is, however, an extremely common cause worldwide. b) Drugs such as NSAIDS are not the cause of occult blood loss resulting in anaemia. c) Malabsorption of iron due to cœliac disease is excluded. Back Case 2 Answer 2 Chronic intestinal blood loss. Such patients must be considered to have this until proven otherwise. Testing for faecal occult blood is unhelpful as the test is often negative because bleeding may be intermittent. Back: Case 2 Answer 3 Right-sided carcinomas are usually fungating and the intestinal contents liquid and blood loss rather than obstruction results. Left-sided carcinomas are usually annular encircling tumours and the intestinal contents semi-solid, hence altered bowel habit and crampy left lower quadrant discomfort are presenting symptoms. Carcinomas in both locations can ulcerate and there are no histological differences between them. Figure 17-61 Carcinoma of the cecum. The fungating carcinoma projects into the lumen but has not caused obstruction. © 2005 Elsevier Figure 17-63 Invasive adenocarcinoma of colon, showing malignant glands infiltrating the muscle wall. Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 16 November 2005 05:17 PM) © 2005 Elsevier The encircling mass of firm adenocarcinoma in this colon at the left is typical for adenocarcinomas arising in the descending colon. A change in stool or bowel habits can be created by the mass effect. By colonoscopy, a fungating, ulcerating mass is seen in the views below. Continue below Microscopically, a moderately differentiated adenocarcinoma of colon is seen here. There is still a glandular configuration, but the glands are irregular and very crowded. Many of them have lumens containing bluish mucin. At high magnification, the neoplastic glands of adenocarcinoma have crowded nuclei with hyperchromatism and pleomorphism. No normal goblet cells are seen. This small adenomatous polyp (tubular adenoma) on a small stalk is seen microscopically to have more crowded, disorganized glands than the normal underlying colonic mucosa. Goblet cells are less numerous and the cells lining the glands of the polyp have hyperchromatic nuclei. However, it is still well-differentiated and circumscribed, without invasion of the stalk, and is benign. Two colonoscopic views of a small polyp that proved to be a tubular adenoma is seen below. This adenomatous polyp has a hemorrhagic surface (which is why they may first be detected with stool occult blood screening) and a long narrow stalk. The size of this polyp--above 2 cm--makes the possibility of malignancy more likely, but this polyp proved to be benign. Back: Case 2 Answer 4 The liver, being the most common site for metastases from tumours in the portal venous drainage area. Later metastases may occur to the lungs, bone, brain and other sites. Note the numerous mass lesions that are of variable size. Some of the larger ones demonstrate central necrosis. The masses are metastases to the liver. The obstruction from such masses generally elevates alkaline phosphatase, but not all bile ducts are obstructed, so hyperbilirubinemia is typically not present. Also, the transaminases are usually not greatly elevated. Continue below Here are liver metastases from an adenocarcinoma primary in the colon, one of the most common primary sites for metastatic adenocarcinoma to the liver. Back: