Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
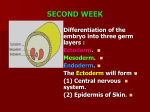
CONGENITAL ANOMALIES OF THE CENTRAL NERVOUS SYSTEM SUBMITTED BY: Nicole Christianne Mae B. Bacayo BSOT-IV SUBMITTED TO: Dr. Gerrard Dennis Uy A. Neural Tube Defects Neural tube defects (NTDs) account for the largest proportion of congenital anomalies of the CNS and result from failure of the neural tube to close spontaneously between the 3rd and 4th wk of in utero development. Precise cause of NTDs remains unknown, but evidence suggests that many factors can adversely affect normal development of the CNS from the time of conception. These include the following: including hyperthermia, drugs (valproic acid), malnutrition, chemicals, maternal obesity or diabetes, and genetic determinants (mutations in folate-responsive or folate- dependent enzyme pathways). In some cases, an abnormal maternal nutritional state or exposure to radiation before conception increases the likelihood of a congenital CNS malformation. The major NTDs include spina bifida occulta, meningocele, myelomeningo-cele, encephalocele, anencephaly, caudal regression syndrome, dermal sinus, tethered cord, syringomyelia, diastematomyelia, and lipoma involving the conus medullaris and/or filum terminale and the rare condition iniencephaly. The human nervous system originates from the primitive ectoderm that also develops into the epidermis. The ectoderm, endoderm, and mesoderm form the three primary germ layers that are developed by the 3rd wk. The endoderm, particularly the notochordal plate and the intraembryonic mesoderm, induces the overlying ectoderm to develop the neural plate in the 3rd week of development. Failure of normal induction is responsible for most of the NTDs, as well as disorders of prosencephalic development. Rapid growth of cells within the neural plate causes further invagination of the neural groove and differentiation of a conglomerate of cells, the neural crest, which migrate laterally on the surface of the neural tube. The notochordal plate becomes the centrally placed notochord, which acts as a foundation around which the vertebral column ultimately develops. With formation of the vertebral column, the notochord undergoes involution and becomes the nucleus pulposus of the intervertebral disks. The neural crest cells differentiate to form the peripheral nervous system, including the spinal and autonomic ganglia and the ganglia of cranial nerves V, VII, VIII, IX, and X. In addition, the neural crest forms the leptomeninges, as well as Schwann cells, which are responsible for myelination of the peripheral nervous system. The dura is thought to arise from the paraxial mesoderm. In the region of the embryo destined to become the head, similar pat-terns exist. In this region, the notocord is replaced by the precordal mesoderm. In the 3rd wk of embryonic development, invagination of the neural groove is completed and the neural tube is formed by separation from the overlying surface ectoderm. Initial closure of the neural tube is accomplished in the area corresponding to the future junction of the spinal cord and medulla and moves rapidly both caudally and rostrally. For a brief period, the neural tube is open at both ends, and the neural canal communicates freely with the amniotic cavity. Failure of closure of the neural tube allows excretion of fetal substances (α-fetoprotein [AFP], acetylcholinesterase) into the amniotic fluid, serving as biochemical markers for a NTD. Prenatal screening of maternal serum for AFP in the 16th-18th wk of gestation is an effective method for identifying pregnancies at risk for fetuses with NTDs in utero. Normally, the rostral end of the neural tube closes on the 23rd day and the caudal neuropore closes by a process of secondary neurulation by the 27th day of development, before the time that many women realize they are pregnant. The embryonic neural tube consists of three zones: ventricular, mantle, and marginal. The ependymal layer consists of pluripotential, pseudostratified, columnar neuroepithelial cells. Specific neuroepithelial cells differentiate into primitive neurons or neuroblasts that form the mantle layer. The marginal zone is formed from cells in the outer layer of the neuroepithelium, which ultimately becomes the white matter. Glioblasts, which act as the primitive supportive cells of the CNS, also arise from the neuroepithelial cells in the ependymal zone. They migrate to the mantle and marginal zones and become future astrocytes and oligodendrocytes. It is likely that microglia originate from mesenchymal cells at a later stage of fetal development when blood vessels begin to penetrate the developing nervous system. 2 Spina Bifida Occulta (Occult Spinal Dysraphism) Spina bifida occulta is a common anomaly consisting of a midline defect of the vertebral bodies without protrusion of the spinal cord or meninges. Most patients are asymptomatic and lack neurologic signs. The condition is usually of no consequence. Spina Bifida Occulta - Merely a posterior vertebral body fusion defect - Does not have an associated spinal cord malformation Occult Spinal Dysraphism - Term used for other clinically more significant form of this closed spinal cord malformation - In most of these cases, there are cutaneous manifestations such as a hemangioma, discoloration of the skin, pit, lump, dermal sinus, or hairy patch. - There is no abnormality of the meninges, spinal cord, or nerve roots. - Is often associated with more significant developmental abnormalities of the spinal cord - Diagnosis: Spine roentgenogram- shows a defect in closure of the posterior vertebral arches and laminae, typically involving L5 and S1 All cases of occult spinal dysraphism are best investigated with MRI. Initial screening in the neonate may include ultrasonography. - A dermoid sinus usually forms a small skin opening, which leads into a narrow duct, sometimes indicated by protruding hairs, a hairy patch, or a vascular nevus. Dermoid sinuses occur in the midline at the lumbosacral region or occiput, respectively. Dermoid sinus tracts can pass through the dura, acting as a conduit for the spread of infection. Recurrent meningitis of occult origin should prompt careful examination for a small sinus tract in the posterior midline region, including the back of the head. Lower back sinuses are usually above the gluteal fold and are directed cephalad. Tethered spinal cord syndrome may also be an associated problem. Diastematomyelia commonly has bony abnormalities that require surgical intervention along with untethering of the spinal cord. Imaging of the spine in cutaneous lesions: CUTANEOUS LESIONS ASSOCIATED WITH OCCULT SPINAL DYSRAPHISM IMAGING INDICATED Subcutaneous mass or lipoma Hairy patch Dermal sinus Atypical dimples (deep, >5 mm, or >25 mm from anal verge) Vascular lesion, eg., hemangioma or telangiectasia Skin appendages pr polypoid lesions, eg., skin tags, tail-like appendages Scarlike lesions IMAGING UNCERTAIN Hyperpigmented patches Deviation of the gluteal fold IMAGING NOT REQUIRED Simple dimples (<25 mm from anal verge) Coccygeal pits Meningocele A meningocele is formed when the meninges herniate through a defect in the posterior vertebral arches or the anterior sacrum. 3 The spinal cord is usually normal and assumes a normal position in the spinal canal, although there may be tethering, syringomyelia, or diastematomyelia. A fluctuant midline mass that might trans-illuminate occurs along the vertebral column, usually in the lower back. Most meningoceles are well covered with skin and pose no immediate threat to the patient. An anterior meningocele projects into the pelvis through a defect in the sacrum. Symptoms of constipation and bladder dysfunction develop due to the increasing size of the lesion. Female patients might have associated anomalies of the genital tract, including a rectovaginal fistula and vaginal septa. Careful neurologic examination is mandatory. Orthopedic and urologic examination should also be considered. Examinations: - plain x-rays, ultrasonography, CT scan and MRI Determine the extent of neural tissue involvement, if any, and associated anomalies, including diastematomyelia, lipoma, and possible clinically significant tethered spinal cord Plain x-rays demonstrate a defect in the sacrum CT scanning or MRI outlines the extent of the meningocele and any associated anomalies. A CT scan or MRI of the head is recommended for children with a meningocele because of the association with hydrocephalus in some cases. - Urologic evaluation, usually including cystometrogram (CMG) Identifies children with neurogenic bladder who are at risk for renal deterioration Treatment: - Patients with leaking cerebrospinal fluid (CSF) or a thin skin covering should undergo immediate surgical treatment to prevent meningitis. - In asymptomatic children with normal neurologic findings and full thickness skin covering the meningocele, surgery may be delayed or sometimes not performed. Myelomenigocele Myelomeningocele represents the most severe form of dysraphism, a so-called aperta or open form, involving the vertebral column and spinal cord. Epidemiology: - Occurs with an incidence of approximately 1/4,000 live births - The risk of recurrence after one affected child is 3-4% and increases to 10% with 2 prior affected children. - Hydrocephalus in association with a type II Chiari malformation develops in at least 80% of patients with myelomeningocele. - Certain drugs, including drugs that antagonize folic acid, such as trimethoprim and the anticonvulsants carbamazepine, phenytoin, phenobarbital, and primidone, increase the risk of myelomeningocele. - The anticonvulsant valproic acid causes NTDs in approximately 1-2% of pregnancies when administered during pregnancy. Etiology: - The cause of myelomeningocele is unknown. - A genetic predisposition exists, as with all neural tube closure defects including anencephaly. - The risk occurrence and the presence of substantial familial aggregation of anencephaly, myelomeningocele, and craniorachischisis indicate heredity, on a polygenic basis, as a significant contributor to the etiology of NTDs. - Nutritional and environmental factors have a role in the etiology of myelomeningocele as well. - Folate is intricately involved in the prevention and etiology of NTDs. Folate functions in single-carbon transfer reactions and exists in many chemical forms. 4 Folic acid (pteroylmonoglutamic acid), which is the most oxidized and stable form of folate, occurs rarely in food but is the form used in vitamin supplements and in fortified food products, particularly flour. Most naturally occurring folates (food folate) are pteroylpolyglutamates, which contain 1-6 additional glutamate molecules joined in a peptide linkage to the γ-carboxyl of glutamate. Folate coenzymes are involved in DNA synthesis, purine synthesis, generation of formate into the formate pool, and amino acid interconversion; the conversion of homocysteine to methionine provides methionine for the synthesis of S-adenosyl-methionine (SAM-e, an agent important for in vivo methylation). Mutations in the genes encoding the enzymes involved in homocysteine metabolism include 5, 10 methylenetetrahydrofolate reductase (MTHFR), cystathio-nine β-synthase, and methionine synthase. An association between a thermolabile variant of MTHFR and mothers of children with NTDs might account for up to 15% of preventable NTDs. Maternal periconceptional use of folic acid supplementation reduces the incidence of NTDs in pregnancies at risk by at least 50%. To be effective, folic acid supplementation should be initiated before conception and continued until at least the 12th wk of gestation, when neurulation is complete. The mechanisms by which folic acid prevents NTDs remain poorly understood. Clinical Features and Manifestations - Myelomeningocele produces dysfunction of many organs and structures, including the skeleton, skin, and gastrointestinal and genitourinary tracts, in addition to the peripheral nervous system and the CNS. - A myelomeningocele may be located anywhere along the neuraxis, but the lumbosacral region accounts for at least 75% of the cases. - .A lesion in the low sacral region causes bowel and bladder incontinence associated with anesthesia in the perineal area but with no impairment of motor function. - Newborns with a defect in the midlumbar or high lumbothoracic region typically have either a saclike cystic structure covered by a thin layer of partially epithelialized tissues or an exposed flat neural placode without overlying tissues. - Examination of the infant shows a flaccid paralysis of the lower extremities, an absence of deep tendon reflexes, and a lack of response to touch and pain, and a high incidence of lower extremity deformities (clubfeet, ankle and/or knee contractures, and subluxation of the hips). - Some children have constant urinary dribbling and a relaxed anal sphincter. Other children do not leak urine and in fact have a high-pressure bladder and sphincter dysynergy. - A myelomeningocele above the midlumbar region tends to produce lower motor neuron signs due to abnormalities and disruption of the conus medullaris and above spinal cord structures. - These infants sometimes have an associated kyphotic gibbus that requires neonatal orthopedic corrections. - Patients with a myelomeningocele in the upper thoracic or cervical region usually have a very minimal neurologic deficit and, in most cases, do not have hydrocephalus but they can have neurogenic bladder and bowel. - The possibility of hydrocephalus developing should always be considered, no matter what the spinal level. - Ventricular enlargement may be indolent and slow growing or may be rapid causing a bulging anterior fontanel, dilated scalp veins, setting-sun appearance of the eyes, irritability, and vomiting associated with an increased head circumference. - About 15% of infants with hydrocephalus and Chiari II malformation develop symptoms of hindbrain dysfunction, including difficulty feeding, choking, stridor, apnea, vocal cord paralysis, pooling of secretions, and spasticity of the upper extremities, which, if untreated, can lead to death. - This Chiari crisis is due to downward herniation of the medulla and cerebellar tonsils through the foramen magnum as well is endogenous malformations in the cerebellum and brainstem. 5 Prevention: - The U.S. Public Health Service has recommended that all women of childbearing age and who are capable of becoming pregnant take 0.4 mg of folic acid daily. - If, however, a pregnancy is planned in high-risk women (previously affected child), supplementation should be started with 4 mg of folic acid daily, beginning 1 mo before the time of the planned conception. - The modern diet provides about half the daily requirement of folic acid. - To increase folic acid intake, fortification of flour, pasta, rice, and cornmeal with 0.15 mg folic acid per 100 g was mandated in the United States and Canada in 1998. - The added folic acid will be insufficient to maximize the prevention of preventable NTDs. - Therefore, informative educational programs and folic acid vitamin supplementation remain essential for women planning a pregnancy and possibly for all women of childbearing age. - In addition, women should also strive to consume food folate from a varied diet. - Certain drugs, including drugs that antagonize folic acid, such as trimethoprim and the anticonvulsants carbamazepine, phenytoin, phenobarbital, and primidone, increase the risk of myelomeningocele. - The anticonvulsant valproic acid causes NTDs in approximately 1-2% of pregnancies when administered during pregnancy. - Some epilepsy clinicians recommend that all female patients of childbearing potential who take anticonvulsant medications also receive folic acid supplements. Treatment: - Management and supervision of a child and family with a myelomeningocele require a multidisciplinary team approach: Surgeons, physicians, and therapists, with one individual (often a pediatrician) acting as the advocate and coordinator of the treatment program. - Surgery is often done within a day or so of birth but can be delayed for several days (except when there is a CSF leak) to allow the parents time to begin to adjust to the shock and to prepare for the multiple procedures and inevitable problems that lie ahead. - Evaluation of other congenital anomalies and renal function can also be initiated before surgery. - After repair of a myelomeningocele, most infants require a shunting procedure for hydrocephalus. If symptoms or signs of hindbrain dysfunction appear, early surgical decompression of the posterior fossa is indicated. - Clubfeet can require taping or casting, and dislocated hips can require operative procedures. - Careful evaluation and reassessment of the genitourinary system are some of the most important components of the management. Regular catheterization of a neurogenic bladder is a crucial step in maintaining a low residual volume and bladder pressure that prevents urinary tract infections and reflux leading to pyelonephritis, hydronephrosis, and bladder damage. Latex-free catheters and gloves must be used to prevent development of latex allergy. Periodic urine cultures and assessment of renal function, including serum electrolytes and creatinine as well as renal scans, vesiculourethrograms (VCUGs), renal ultrasonography, and cystometrograms (CMGs), are obtained according to the risk status and progress of the patient and the results of the physical examination. Some children can become continent with surgical implantation of an artificial urinary sphincter (these are used less often) or bladder augmentation at a later age. Although incontinence of fecal matter is common and is socially unacceptable during the school years, it does not pose the same organ-damaging risks as 6 urinary dysfunction, but occasionally fecal impaction and/or megacolon develop. Many children can be bowel-trained with a regimen of timed enemas or suppositories that allows evacuation at a predetermined time once or twice a day. Special attention to low anorectal tone and enema administration and retention is often required. Appendicostomy for antegrade enemas may also be helpful. - Functional ambulation is the wish of each child and parent and may be possible, depending on the level of the lesion and on intact function of the iliopsoas muscles. Almost every child with a sacral or lumbosacral lesion obtains functional ambulation; approximately half the children with higher defects ambulate with the use of braces, other orthotic devices, and canes. Ambulation is often more difficult as adolescence approaches and body mass increases. Deterioration of ambulatory function, particularly during earlier years, should prompt referral for evaluation of tethered spinal cord and other neurosurgical issues. In utero surgical closure of a spinal lesion has been successful in a few centers. - Preliminary reports suggest a lower incidence of hindbrain abnormalities and hydrocephalus (fewer shunts) as well as improved motor outcomes. This suggests that the defects may be progressive in utero and that prenatal closure might prevent the development of further loss of function. In utero diagnosis is facilitated by maternal serum α-fetoprotein screening and by fetal ultrasonography. Prognosis: - Mortality rate is 10-15% Children with aggressive treatment - Most deaths occur before age 4 yr, although life-threatening complications occur at all ages. - At least 70% of survivors have normal intelligence, but learning problems and seizure disorders are more common than in the general population. - Previous episodes of meningitis or ventriculitis adversely affect intellectual and cognitive function. - Because myelomeningocele is a chronic disabling condition, periodic multidisciplinary follow-up is required for life. - Renal dysfunction is one of the most important determinants of mortality. Encephalocele A cranial meningocele consists of a CSF-filled meningeal sac plus cerebral cortex, cerebellum, or portions of the brainstem. Microscopic examination of the neural tissue within an encephalocele often reveals abnormalities. The cranial defect occurs most commonly in the occipital region at or below the inion, but in certain parts of the world, frontal or naso-frontal encephaloceles are more prominent. These abnormalities are one tenth as common as neural tube closure defects involving the spine. Etiology: - Etiology is presumed to be similar to that for anencephaly and myelomeningocele. - Infants with a cranial encephalocele are at increased risk for developing hydrocephalus due to aqueductal stenosis, Chiari mal-formation, or the DandyWalker syndrome. Examinations and Diagnosis: - Examination might show a small sac with a pedunculated stalk or a large cyst like structure that can exceed the size of the cranium. - Transillumination of the sac can indicate the presence of neural tissue. - A plain x-ray of the skull and cervical spine is indicated to define the anatomy of the vertebrae. - Ultrasonography is most helpful in determining the contents of the sac. - MRI or CT further helps define the spectrum of the lesion. 7 Fetal MRI can help define the extent of associated CNS anomalies and the degree of brain herniated into the encephalocele. - Determination of maternal serum α-fetoprotein levels and ultrasound measurement of the biparietal diameter as well as identification of the encephalocele itself can diagnose encephaloceles in utero. Prognosis: - Patients with an encephalocele are at risk for: vision problems, microcephaly, mental retardation, and seizures - Generally, children with neural tissue within the sac and associated hydrocephalus have the poorest prognosis. - Cranial encephalocele is often part of a syndrome. Meckel-Gruber syndrome is a rare autosomal recessive condition that is characterized by an occipital encephalocele, cleft lip or palate, microcephaly, microphthalmia, abnormal genitalia, polycystic kidneys, and polydactyly. Anencephaly An anencephalic infant presents a distinctive appearance with a large defect of the calvarium, meninges, and scalp associated with a rudimentary brain. Anencephaly results from failure of closure of the rostral neuropore, the opening of the anterior neural tube. The cerebral hemispheres and cerebellum are usually absent, and only a residue of the brainstem can be identified. The pituitary gland is hypoplastic, and the spinal cord pyramidal tracts are missing owing to the absence of the cerebral cortex. Additional anomalies include folding of the ears, cleft palate, and congenital heart defects in 10-20% of cases. Etiology: - Genetics - Low socioeconomic status - Nutritional and vitamin deficiencies - Environmental factors - Toxic factors It is very likely that several noxious stimuli interact on a genetically susceptible host to produce anencephaly. Epidemiology: - The incidence of anencephaly approximates 1/1,000 live births - The greatest incidence is in Ireland, Wales, and Northern China. - The recurrence risk is approximately 4% and increases to 10% if a couple has had two previously affected pregnancies. - The incidence of anencephaly has been decreasing in the past 2 decades. - Approximately 50% of cases of anencephaly have associated polyhydramnios. - Couples who have had an anencephalic infant should have successive pregnancies monitored, including amniocentesis, determination of AFP levels, and ultrasound examination between the 14th and 16th wk of gestation. Course and Prognosis - Most anencephalic infants die within several days of birth. B. Disorders Of Neuronal Migration Disorders of neuronal migration can result in minor abnormalities with little or no clinical consequence (small heterotopia of neurons) or devastating abnormalities of CNS structure and/or function (mental retardation, seizures, lissencephaly, and schizencephaly, particularly the open-lip form). One of the most important mechanisms in the control of neuronal migration is the radial glial fiber system that guides neurons to their proper site. Migrating neurons attach to the radial glial fiber and then disembark at predetermined sites to form, ultimately, the precisely designed six-layered cerebral cortex. Another important mechanism is the tangential migration of progenitor neurons destined to become cortical interneurons. The severity and the extent of the disorder are related to numerous factors, including the timing of a particular insult and a host of environmental and genetic contributors. 8 Lissencephaly Lissencephaly, or agyria, is a rare disorder that is characterized by the absence of cerebral convolutions and a poorly formed sylvian fissure, giving the appearance of a 3-4 mo fetal brain. Etiology: - The condition is probably a result of faulty neuroblast migration during early embryonic life and is usually associated with enlarged lateral ventricles and heterotopias in the white matter. - In some forms, there is a four-layered cortex, rather than the usual six-layered one, with a thin rim of periventricular white matter and numerous gray heterotopias visible by microscopic examination. - Doublecortinis, an X chromosome gene that causes lissencephaly when mutated in males and subcortical band heterotopia when mutated in females. Clinical Features: - These infants present with failure to thrive, microcephaly, marked developmental delay, and a severe seizure disorder. - Ocular abnormalities are common, including hypoplasia of the optic nerve and microphthalmia. - Lissencephaly can occur as an isolated finding, but it is associated with Miller-Dieker syndrome (MDS) in about 15% of cases. These children have characteristic faces, including a prominent forehead, bitemporal hollowing, anteverted nostrils, a prominent upper lip, and micrognathia. About 90% of children with MDS have visible or submicroscopic chromosomal deletions of 17p13.3. The gene LIS-1 (lissencephaly 1) that maps to chromosome region 17p13.3 is deleted in patients with MDS. - Other important forms of lissencephaly include the Walker-Warburg variant and other cobblestone cortical malformations. Examinations: - CT and MRI scans typically show a smooth brain with an absence of sulci. Schizencephaly Schizencephaly is the presence of unilateral or bilateral clefts within the cerebral hemispheres owing to an abnormality of morphogenesis. The cleft may be fused or unfused. There is notable absence of cerebralsulci iand the mal-developed sylvian fissure as associated with enlarged ventricles. Unilateral schizencephaly shown, if unilateral and large, may be confused with a porencephalic cyst. Not infrequently, the borders of the cleft are surrounded by abnormal brain, particularly microgyria. Etiology: - It remains controversial whether genetic causes of schizencephaly exist. Examination tools: - MRI is the study of choice for elucidating schizencephaly and associated malformations. Clinical Features: - Many patients are severely mentally retarded, with seizures that are difficult to control, and microcephalic, with spastic quadriparesis when the clefts are bilateral. - Some cases of bilateral schizencephaly are associated with septo-optic dysplasia and endocrinologic disorders. - Unilateral schizencephaly is a common cause of congenital hemiparesis. 9 Neuronal Heterotopias Subtypes of neuronal heterotopias include: - Periventricular nodular heterotopias - Subcortical heterotopia (including band-type) - Marginal glioneuronal heterotopias Etiology: - Several genes have been identified that are a cause of these conditions. Clinical Features: - Intractable seizures are a common feature. Polymicrogyrias Polymicrogyria is characterized by an augmentation of small convolutions separated by shallow enlarged sulci. Etiology: - Several genes have been identified that cause several of the forms of this condition. Clinical Feature: - Epilepsy, including drug-resistant forms, is a common feature. Focal Cortical Dysplasias Focal cortical dysplasias consist of abnormal cortical lamination in a discrete area of cortex. High-resolution, thin-section MRI can reveal these areas sometimes in the setting of drugresistant epilepsy. Porencephaly Porencephaly is the presence of cysts or cavities within the brain that result from developmental defects or acquired lesions, including infarction of tissue. True porencephalic cysts are most commonly located in the region of the sylvian fissure and typically communicate with the subarachnoid space, the ventricular system, or both. They represent developmental abnormalities of cell migration and are often associated with other malformations of the brain, including microcephaly, abnormal patterns of adjacent gyri, and encephalocele. Pseudoporencephalic cysts characteristically develop during the perinatal or postnatal period and result from abnormalities (infarction, hemorrhage) of arterial or venous circulation. These cysts tend to be unilateral, do not communicate with a fluid-filled cavity, and are not associated with abnormalities of cell migration or CNS malformations. Clinical Features: - Affected infants tend to have many problems, including mental retardation, spastic hemiparesis or quadriparesis, optic atrophy, and seizures. Etiology: - Mutations in the COL4A1gene have been described in cases of familial porencephaly. Risk Factors: - Several risk factors for porencephalic cyst formation have been identified including: hemorrhagic venous infarctions various thrombophilias such as protein C deficiency and factor V Leiden mutations perinatal alloimmune thrombocytopenia von Wille-brand’s disease maternal warfarin use maternal cocaine use congenital infections trauma such as amniocentesis maternal abdominal trauma 10 11