Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
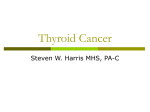
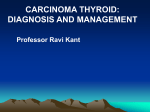
Update in the Management of Thyroid Neoplasms David R. Byrd, MD Department of Surgery University of Washington NCCN - National Comprehensive Cancer Network • yearly update from the NCI-designated comprehensive cancer centers (FHCRC -> FHCRC + UWMC) • Consensus guidelines from the NCCN membership institutions • not focussed on the practice of the community cancer practitioner NCCN - Management of Thyroid Carcinoma -2001 Thyroid Nodule - History Local Sxs Risk factors Function Thyroid nodules • 6-10% adult U.S. population – 5% are malignant • FNA best initial test - 96% PPV • U/S good to follow or document MNG • thyroid scan good if symptoms of hyper- or hypothyroidism or if indeterminate cytology/multinodular goiter • suppression most successful when TSH high FNA Results of Thyroid Nodule Benign --> F/U 6-12 months cyst --> F/U 6-12 months FNA indeterminate --> repeat FNA, I123 scan if same results follicular neoplasm --> I123 scan or surgery suspicious --> surgery carcinoma --> surgery Results of 123 I scan “hot” --> check TFTs I123 scan “euthyroid” --> rarely CA, F/U only “cold”* (still takes up some iodine, though less than normal gland) *NOTE: 1. Nearly all cancers are “cold” 2. However, only about 10-15% of “cold” nodules are cancer Thyroid Carcinoma ©National Comprehensive Cancer Network - Nodule Evaluation Thyroid Carcinoma - Nodule Evaluation ©National Comprehensive Cancer Network Pathology of Thyroid Cancer • differentiated thyroid cancer (DTC): – papillary - commonly spreads to nodes (40-50%), excellent prognosis – mixed - papillary and follicular - acts like papillary, excellent prognosis – follicular - slightly worse than papillary, can spread to bone, less to nodes (15%); Hurthle cell Ca is variant • medullary - sporadic vs. familial (MEN 2A), total thyroidectomy is treatment • anaplastic - aggressive and fatal, surgical role is biopsy only Thyroid Carcinoma - Papillary Carcinoma ©National Comprehensive Cancer Network Rationale for Total Thyroidectomy for DTC • • • • • • improved effectiveness for I131 ablation lowers dose needed forI131 ablation allows f/u w/ thyroglobulin levels decreased recurrence improved survival in high risk pts. decreased risk of pulmonary mets and dedifferentiated CA Rationale Against Total Thyroidectomy for DTC • • • • • increased RLN injury and hypoparathyroidism contralateral disease not clinically relevant survival nearly equivalent for low risk patients I131 ablation not necessary for most patients thyroglobulin levels not necessary for most patients Thyroidectomy for DTC Technique • • • • know the anatomy protect RLN preserve all parathyroids know when to reassess or quit Thyroid Carcinoma - Papillary Carcinoma ©National Comprehensive Cancer Network Lymphadenectomy for Papillary or Mixed Thyroid CA parathyroid RLN Thyroid Carcinoma - Papillary Carcinoma ©National Comprehensive Cancer Network Thyroid Carcinoma - Papillary Carcinoma ©National Comprehensive Cancer Network Thyroid Carcinoma - Papillary Carcinoma ©National Comprehensive Cancer Network Thyroid Carcinoma ©National Comprehensive Cancer Network - Papillary Carcinoma Thyroid Carcinoma - Follicular Carcinoma ©National Comprehensive Cancer Network Thyroid Carcinoma - Follicular Carcinoma ©National Comprehensive Cancer Network Thyroid Carcinoma - Follicular Carcinoma ©National Comprehensive Cancer Network Thyroid Carcinoma - Follicular Carcinoma ©National Comprehensive Cancer Network Thyroid Carcinoma - Follicular Carcinoma ©National Comprehensive Cancer Network ? Residual Thyroid Cancer • 25 y/o woman with papillary thyroid cancer – Capsular penetration – Lymph nodes not sampled • Dx and Post-Rx (200 mCi) I-131 scans show thyroid remnant only – TG off TSH = 110 ng/dL • Dx I-131 scan 1 year later negative – TG off TSH is still 100 ng/dL Thyroid Cancer Post therapy (10/98) Tc-99m markers 2055870 I-131 window Thyroid Cancer Diagnostic Scan (7/99) Tc-99m markers 2055870 I-131 window ? Residual Thyroid Cancer: FDG PET Scan 8/99 L Cervical Lymph Nodes 20558 70 ? Central Lymph Nodes Case 1 • 60F undergoes L thyroid lobectomy for a solitary nodule w/ follicular cells on FNAC. • Final path shows 2cm follicular adenoma and incidental 5mm papillary thyroid CA • ?further management Case 1 - issues Result: the 2 cm nodule is benign and the 0.5cm nodule is an incidental carcinoma of minimal significance • • • • ? Completion thyroidectomy --> NO ? Radioactive iodine therapy --> NO ? Thyroid suppression --> +/? F/u -6 month intervals with H & P Case 2 • 40M w/ solitary 1.5cm L thyroid nodule on exam • h/o neck irradiation for enlarged thymus as child • ?further management Case 2 - Issues This is a setting of higher risk of cancer - male, solitary lesion, and equivocal hx of neck irradiation: minimal operation is thyroid lobectomy + isthmusectomy, proceed to total or subtotal thyroidectomy if bilateral nodules and/or if carcinoma found frozen section is notoriously unable to definitively call carcinoma - therefore permanent pathology usually necessary to confirm carcinoma