Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
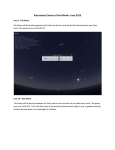
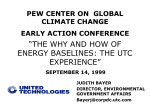
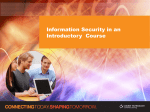
Case report Large tumoral calcinosis and pathological femoral fracture in a hemodialysis patient: A case report ABSTRACT Tumoral calcinosis (TC), is a rare complication of patients with uremia on dialysis(hemodialysis or peritoneal dialysis). We present a case of large tumoral calcinosis and pathological femoral fracture in a 49-year-old woman with uremia and secondary hyperparathyroidism (HPT) on hemodialysis. She was admitted to our hospital because of a swelling mass over her left proximal thigh for 2 years and a decreased range of left hip’s motion for 15 days. After serial examinations, the consultation of the department of thyroid surgery, nephrology and anesthesiology, Excision of the mass and the left proximal erosive femur was performed, associated with partial hip arthroplasty of the proximal femoral endoprosthesis. The pathological examination results revealed tumoral calcinosis. After surgery, she recovered good and then continued to accept hemodialysis regularly. Keywords: Tumoral calcinosis, Pathologic fracture, Hemodialysis , Secondary hyperparathyroidism Background.Tumoral calcinosis (TC) is an uncommon disease, whose formats are the periarticular masses of calcium-phosphate (Ca–P) crystals deposit in the subcutaneous soft tissues around large joints. Uremic tumoral calcinosis (UTC) is the term for TC occurring in uremic patients. Other terms used in the literature for this lesion are metastatic calcifications, tumoral calcification, secondary tumoral calcinosis, tumoral calcinosis-like lesion, pseudotumor calcinosis and nonfamilial tumoral calcinosis.1, 2 The mechanism of UTC is not fully understood, although the most important factors predisposing to UTC are considered to be secondary HPT and an increase of the serum (plasma) Ca–P product. Medical therapy to balance calcium and phosphorus is the cornerstone of treatment. However, surgical excision is indicated when pain or other compression symptoms occur. 3 This case is presented because the lesion with erosion of bone and surrounding soft tissues is easy to be misdiagnosed. Case Report. On January 8,2014, a 49-year-old Chinese woman was admitted to our hospital for evaluation of a swelling mass over her left proximal thigh and treatment of the limitation of her left hip joint movement. Two years ago, she noted a hard mass palpable around her left proximal thigh with painless, and the movement of her left hip joint was normal. Fifteen days ago, her left hip joint could not move and severe pain occurred without obvious precipitating factors. She had a history of chronic renal failure and had received hemodialysis for 12 years during her initial presentation, and she was on dialysis three times weekly for 4 hours per session. In addition, she had no infection, injury and familial TC history. On admission, her body temperature was 36.0 °C. Physical examination revealed a hard mass, about 22×15×11cm in size, located around the left proximal thigh. The patient reported a painful sensation while palpating the mass. It severely limited the movement of her left hip joint. The overlying skin was intact. Before the admission, she only received regular hemodialysis without any medicine. Laboratory findings were as follows: albumin (ALB), 36 g/L (reference range, 40.0 –55.0 g/L); glucose (GLU), 5.61 mmol/L (reference range, 3.9–5.9 mmol/L); totalkaline phosphatase(ALP),726 U/L(reference range,35–100U/L); blood urea nitrogen (BUN), 15.45 mmol/L (reference range, 2.95–7.70 mmol/L), creatinine(CREA),526.0 umol/L (reference range, 37–110.0 umol/L);calcium (Ca), 2.42 mmol/L (reference range, 2.1–2.7 mmol/L); phosphorus (P), 1.74 mmol/L( reference range, 0.81–1.45 mmol/L); parathyroid hormone(PTH), 169.2 pmol/L (reference range,1.60–6.90 pmol /L). Plain radiographs showed a large mass with heterogeneously calcified density and bony destruction around the left proximal femur (Figure 1A). Magnetic resonance imaging (MRI) showed the lesion with hypointense on T1-weighted and T2-weighted images, and the destruction of femoral cortical and medullary cavity with hyperintense on T1-weighted and T2-weighted images (Figure 1B). After serial examinations, and the consultation of the department of thyroid surgery, nephrology, and anesthesiology, a definite diagnosis of UTC, pathological femoral fracture, uremia and secondary HPT was made. It’s recommended that parathroidectomy was first, and the orthopaedic surgery was second. But the patient did not receive parathyroidectomy, so excision of the lesion and the left proximal erosive femur was performed with partial hip arthroplasty of the proximal femoral endoprosthesis on January 21, 2014. Operation findings showed that the large mass around the left proximal thigh eroded femoral bone and surrounding soft tissues (Figure 2A and 2B). At surgery, the lesion was a large, ovoid, focally nodular mass of red soft tissue measuring 15.5× 15× 11 cm. The external surface was variably smooth and intact (Figure 2A). Upon sectioning, the specimen was found to be a cystic lesion containing some yellow-gray chalky material, and the erosion of femoral bone and surrounding soft tissues was found(Figure 2B). The pathological examination results revealed tumoral calcinosis. After surgery, She recovered good and then continued to accept hemodialysis regularly(Figure 3). Discussion. UTC has been reported in patients on dialysis (hemodialysis or peritoneal dialysis). 1, 2 The prevalence of UTC ranges from 0.5% to 3% in hemodialysis patients 4,5 ,while the prevalence in peritoneal dialysis patients is1.6% or 1.9%.1,5 The mean age of onset is 41years (range: 21 –55 years), 5 which is similar to our patient who was 49 years old. Most patients have a low normal body mass index (BMI) (average: 20.85 kg/m2), 5 which is very similar to our patient whose BMI is approximately 20.3. Mean interval from peritoneal dialysis initiation to onset of TC is 45.3 months (range: 17–84 months), 5 while the time in our hemodialysis patients is 12 years. Although the mechanism of the development and progress of UTC is not fully understood, secondary HPT and abnormal vitamin D metabolism are considered to be two proposed mechanisms. In secondary HPT, PTH levels may be significantly increased and are frequently higher than the levels in primary HPT. The secondary HPT is provoked by hypocalcemia, which results from various mechanisms. In response to hypocalcemia, the parathyroid glands may develop hyperplasia and hypertrophy, with an increased secretion of PTH.6 PTH can stimulate bone resorption,6 which leads to osteoporosis and pathologic fracture. In all, secondary HPT is the most frequent cause of the increase in Ca–P product which leads to metastatic calcification. It is noteworthy that the duration of dialysis has been cited as a predisposing factor to the development of UTC, and the risk of occurrence increases with the number of years of hemodialysis, despite normal values of Ca2+× P. 3 This view is consistent with our patient. In chronic renal failure, the elevation of serum phosphate level rises, which depresses the serum calcium level indirectly by inhibiting synthesis of the physiologically active form of 1, 25– hydroxy–vitamin D.6 The lower level of 1, 25 –hydroxy –vitamin D decreases calcium absorption from the intestine.6 This induces hypocalcemia, which increases the secretion of PTH. 7 The most common locations of UTC are the hip, elbow, shoulder, foot and wrists (in descending order).1,3,8 Heterotopic calcification is the main feature, but there also exists heterotopic ossification .3 UTC is often periarticular and large, about 2 to 10 cm in diameter.4 Most masses may be asymptomatic or cause joint pain and motion range limitation or bone pain (related to diaphysitis or bony erosions), compression symptoms have also been reported. 4,6 However, the most diameter of the lesion is 15.5cm in our patient,and there are the erosion of femoral bone and surrounding soft tissues. What’s more serious is that, the left proximal femur fracture is spontaneous and pathologic in our patient. The imaging features of UTC are as follows: On plain radiographs,UTC is an soft-tissue lesion with amorphous massive calcification and it vary infinitely in size and shape.3, 6 On computed tomography (CT), UTC is a dense homogeneous calcified mass with interspersed fibrous septae. On MRI, tumoral calcinosis lesions are distinguished by their hypointensity on both T1- and T2-weighted sequences. Hyperintensity on T2-weighted imaging is occasionally observed due to increased fluid content. 3,6 Whole-body bone scintigraphy showed increased tracer accumulation of Tc-99m MDP in the periarticular soft tissues surrounding the involved joints.5 On ultrasonography, UTC is a dense homogeneous soft tissue mass with calcification.6,9 Although CT images failed to show fluid-filled cystic spaces in the masses due to partial volume averaging effect, ultrasound can show multiloculated cystic spaces within the masses. 9 The masses of TC are thought to originate from bursal calcinations, extendin g with growth to adjacent soft tissues, but rarely causing bone erosion. 6 Bone erosion,even fracture may occur on uremic patients with a long period of dialysis. One report showed that some degree of erosion of the proximal humerus by the UTC mass occurred on a 54-year-old man with clinical history of renal dialysis for 6 years. 6 Another report showed that severe bony erosion around the left distal end of the clavicle by the UTC mass occurred on a 53-year-old man with clinical history of renal dialysis for 20 years. 3 It’s surprising that spontaneous and simultaneous rupture of both Achilles tendons and pathological fracture of the femur neck occurred on a 43-year-old man with clinical history of renal dialysis for 16 years, 7 which is more severe than that on our patient. At surgery, TC lesions are commonly cystic and contain a white-to-pale yellow chalky material identified as calcium hydroxyapatite crystals with amorphous calcium carbonate and calcium phosphate. This is basically identical with our findings in surgery. At histopathologic examination, epithelioid elements and multi-nucleated giant cells surround calcium granules, and multi- nucleated giant cells have osteoclast-like features. These cells are presumed to play a role in the regression of TC. 8-10 It's often misdiagnosed, because many periarticular masses may mimic the presenting pictures of TC, such as osteosarcoma, chondrosarcoma, tophaceous gout, and so on. History, physical examinations, radiographic pictures and laboratory examination results must be accessed carefully before beginning the definite diagnosis. 3 There various treatments on UTC. Medical treatment includes dietary phosphorus restriction, noncalcium phosphate binders, calcimimetics, optimal control of secondary HPT, and intensive hemodialysis with low-calcium dialysate.1,4,5 But the rate of success is variable due to different factors. Surgical treatment includes resection, parathyroidectomy and renal transplantation.Surgical treatments are recommended for persistent or refractory UTC. 3 It’s worth noting that the recurrence of UTC may occur after surgical treatments. 1,4,5 In conclusion, we reported a large UTC and pathological fracture of the left proximal femur in a hemodialysis patient. UTC is an imbalance of calcium and phosphorus metabolism in patients with chronic renal failure and prolonged hemodialysis. Only considering various informations, can make a definite diagnosis. Medical treatment is the foundation. Once severe pain or major functional impairment and other compression symptoms develop, surgical treatment will be applied. After surgery, adjustment of medications, food, and dialysate to balance calcium and phosphorus metabolism is necessary to prevent the recurrence of old lesions as well as occurrence of new lesions. References 1. Shpilberg KA, Blowe SE, Som PM.Mass-like and extensive secondary tumoral calcinosis in the neck and body of a patient on peritoneal dialysis. Clin Imaging 2013; 37:972–975. 2. Olsen KM, Chew FS. Tumoral calcinosis: pearls, polemics, and alternative possibilities. Radiographics 2006; 26:871–985. 3. Jui-Kuo Hung, Ing-Lin Chang, Hui-Mei Chang.Surgical Excision of Tumoral Calcinosis of the Distal End of the Clavicle in a Patient With Uremia. TZU CHI MED J 2009, 21:239–243. 4. Younes M, Belghali S, Zrour-Hassen S, Béjia I, Touzi M, Bergaoui N. Complete reversal of tumoral calcinosis after subtotal parathyroidectomy in a hemodialysis patient. Joint Bone Spine 2008; 75:606– 609. 5. Chu HY, Chu P, Lin YF, Chou HK, Lin SH. Uremic tumoral calcinosis in patients on peritoneal dialysis: clinical, radiologic and laboratory features. Perit Dial Int 2011; 31:430 – 439. 6. Huang YT, Chen CY, Yang CM, Yao MS, Chan WP. Tumoral calcinosis-like metastatic calcification in a patient on renal dialysis. Clin Imaging 2006; 30:66 – 68. 7. Ureten K, Oztürk MA, Ozbek M, Unverdi S. Spontaneous and simultaneous rupture of both Achilles tendons and pathological fracture of the femur neck in a patient receiving long-term hemodialysis. Int Urol Nephrol 2008;40:1103–1106. 8. Hiramatsu R, Ubara Y, Hayami N, Yamanouchi M, Hasegawa E, Sumida K, Suwabe T, Hoshino J, Sawa N, Amizuka N, Takaichi K. Occurrence of new bonelike tissue formation in uremic tumoral calcinosis. Bone 2013;52: 684–688. 9. Barnacle AM, Gower PE, Mitchell AW. Ultrasonography of acute and chronic tumoral calcinosis. Clin Radiol 2002; 57:146–149.10. 10. Yamada S, Taniguchi M, Tokumoto M, Tsuruya K, Iida M. Osteoclast-like multinucleated giant cells in uraemic tumoral calcinosis. NDT Plus 2009; 2:155–157. Figure 1A Antero-posterior radiograph shows multilobulated calcified lesions in the left proximal thigh region. Figure 1B MRI shows a large mass eroded femoral bone and surrounding soft tissues around the left proximal thigh Figure 2A Gross appearance of the mass, which externally measured 15.5 ×15 × 11 cm. Figure 2B Sectioning appearance of the mass, which contained some yellow-gray chalky materials, and the erosion of femoral bone and surrounding soft tissues. Figure 3 Radiograph shows the appearance of the left thigh after surgery.