Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
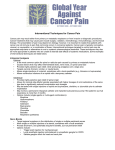
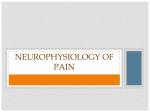
Pain Classification: Nociceptive, Neuropathic, Central and Mixed Rachael Rzasa Lynn, MD Chronic Pain Zoom Webinar 2 December 2015 Definitions • Most basic = neurophysiologic classification – based on presumed mechanism of pain. • Simplified, there are 2 types of pain: – nociceptive pain – non-nociceptive pain • Neuropathic pain • Idiopathic pain – ≠psychogenic pain! Nociceptive Pain • Pain due to continuous tissue injury – actual or threatened damage to non-neural tissue results in activation of peripheral nociceptors • noxious stimulus electrochemical impulses in peripheral nerves spinal cord brain = transduction, transmission, modulation, and perception – Examples: arthritis pain, acute post-traumatic pain – Subdivided into somatic pain and visceral pain Basbaum et al. Cell 2009; 139: 267-284 Nociceptive Pain • Somatic pain – excitation and/or sensitization of nociceptors in tissues such as bone, periarticular soft tissue, joints, and muscles • Well localized • Intermittent or constant • “aching,” “stabbing,” “gnawing,” “throbbing” Nociceptive Pain • Visceral pain – Not produced by all visceral organs • Liver, kidney, most solid viscera, and lung parenchyma are not sensitive to pain. – Not always created by visceral injury – Cutting intestine causes no pain, stretching of the bladder is painful – Diffuse and poorly localized • No separate visceral sensory pathway and low proportion of afferent nerve fibers from viscera • Intermittent or constant • “dull,” “colicky,” “squeezing” – Referrs to other locations. – Accompanied by motor and autonomic reflexes • Eg, nausea, vomiting, muscle tension, etc. Neuropathic Pain • “Pain arising as a direct consequence of a lesion or disease affecting the somatosensory system.” – at any point(s) within the somatosensory pathways – Pain from lesion/disease sustained by aberrant processing in the peripheral and/or central nervous system – typically described as “sharp” or “burning” • This is a clinical description (NOT a diagnosis) – According to IASP, • “this requires a demonstrable lesion or a disease that satisfies established neurological diagnostic criteria.” • “The presence of symptoms or signs (e.g., touch-evoked pain) alone does not justify the use of the term neuropathic.” • “It is common…that diagnostic testing may yield inconclusive or even inconsistent data. In such instances, clinical judgment is required to reduce the totality of findings in a patient into one putative diagnosis or concise group of diagnoses.” Neuropathic Pain • Subsets – Peripherally generated pain: • involves such cervical or lumbar radiculopathy, spinal nerve lesions, and brachial or lumbosacral plexopathies – Centrally generated pain: • involves injury to the central nervous system at the level of the spinal cord or above. – Sympathetically maintained pain: • may be generated peripherally or centrally • characterized by localized autonomic dysregulation – vasomotor or sudomotor changes, edema, sweating, trophic changes including atrophy – Complex Regional Pain Syndrome Central Pain States • Central pain: Pain initiated or caused by a primary lesion or dysfunction in the central nervous system. – Can be produced by an type of vascular, demyelinating, infectious, inflammatory, or traumatic lesion in the brain or spinal cord • Eg, post-stroke pain • Central sensitization: Increase in the excitability of neurons in the spinal cord. – Increased responsiveness of nociceptive neurons in the central nervous system • Increased response to input to which they normally respond • Activation in response to subthreshold input IASP Pain Classification • Multidimensional Classification of Pain – Developed to standardize descriptions of pain syndromes and provide a point of reference – Uses 5 axes to classify chronic pain • Region of the body affected (Axis I), • System whose abnormal functioning could produce the pain (Axis II), • Temporal characteristics of pain and pattern of occurrence (Axis III), • Patient's statement of intensity and time since onset of pain (Axis IV) – Mild, medium or severe, each for ≤1 month, 1-6 months or >6 months duration • Presumed Etiology (Axis V) – Infection, inflammation, neoplasm, toxic, metabolic, etc • Uses the above to create 5-digit code assigned to each chronic pain diagnosis • Limitations: Does not include psychosocial or behavioral data – ALL PAIN HAS A PSYCHOLOGICAL COMPONENT Proposed Taxonomy of Pain Based upon Multifactorial Assessment • Pain Parameters: – Anatomy/System – Duration/Intensity/Quality – Associated Abnormality (physical/psychological) • Underlying Diseases: – Signs/Symptoms • Pain Mechanisms: – NEUROPHYSIOLOGICAL • Primary afferent involvement • CNS involvement – PSYCHOLOGICAL • Cognitive-Affective-Behavioral Involvement – – – – Cognitive appraisal of pain Coping Affect/mood Environment Mixed Pain • Most pain is mixed • Even “nociceptive pain” can lead to central sensitization – Eg, osteoarthritis • fMRI and PET changes – Increased activation in brain areas involved with affect, aversive conditioning and motivation than experimental pain • These patients display hyperalgesia locally and in areas distant from the arthritic joint – After THA, these patients display reduced pain in both areas • ALL pain has a psychological component! Aranda-Villalobos P et al. Arthritis & Rheumatism 2013; 65: 1262-1270. Sofat et al. Rheumatology 2011; 50: 2157-2165 REV I EW S b c Brain S1 Dorsal root ganglion Unmyelinated C- bres Lightly myelinated Aδ- bres Heavily myelinated Aδ- bres ACC PFC IC Thalamus Cortex CeA Dorsal PAG Midbrain LC Pons RVM Medulla Ventral Spinal cord Second-order pain projection neurons Spinal sites a Peripheral terminal Noxious stimuli Thermal Mechanical Chemical In ammation Tissue damage Peripheral tissue Ion channels TRPA TRPM TRPV Nav KCNK ASICs First-order neuron Normal, physiological pain TRP: Transient receptor potential channel (many subtypes) TRPA1=cold (<15°C) in injury (not normal, acute cold), menthol TRPM8=cold(<25°C), menthol TRPV1=heat (>43°C), capsaicin ASICs: Acid-sensing ion channels KCNK: Potassium channel subtypes Nav: Voltage-gated sodium channel isoforms Also Voltage-gated Calcium channels (N- and T-type); α2δ subunit ↑’d after injury Mechanical transduction may occur via TRP, ASIC KCNK channels Figure 1 | Physiological pain processing. a | Nociceptive signals areand/or transmitted from the periphery by nociceptive Nature Reviews | Immunology Grace PM, et al. Nat Rev Immunol. 2014; 14: 217-231 sensory neurons (first-order primary afferent neurons) the peripheral terminals of which are clustered with ion Basbaum et al. Cell 2009; 139: 267-284 Mechanistic Stratification of Medications Used to Treat Neuropathic Pain Fig. 4. Mechanistic stratification of antineuralgic agents. PNS = peripheral nervous system; CBZ = carbamazepine; OXC = oxcarbazepine; PHT = phenytoin; TPM = topiramate; LTG = lamotrigine; TCA = tricyclic antidepressant; NE = norepinephrine; SSRI = selective serotonin re-uptake inhibitor; SNRI = serotonin and norepinephrine re-uptake inhibitor; GBP = gabapentin; LVT = levetiracetam; NMDA = N-methyl-D-aspartate; NSAID = nonsteroidal anti-inflammatory drug. Beydouna & Backonja M. J Pain Symptom Manage. 2003;25:S18-30