Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
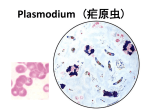
Malaria Endemic in most tropical countries. USE OF ANTIMALARIAL DRUGS The aims of using drugs in relation to malarial infection are: 1. To prevent clinical attack of malaria (private prophylaxis). 2. To treat and completely eradicate the parasite from the patient’s body (Clinical cure). 3. To cutdown human-to-mosquito transmission (public prophylaxis ). The life cycle of malarial parasite in man. Antimalarials that act on erythrocytic schizogony are called erythrocytic (blood) schizontocides Those that act on preerythrocytic as well as exoerythrocytic (P. vivax) stages in liver are called tissue schizontocides Those which kill gametocytes in blood are called gametocides. Comparative properties of antimalarial drugs Private prophylaxis Causal prophylaxis The preerythrocytic phase (in liver) is the target for this purpose. Primaquine is a causal prophylactic for all species of malaria, but has not been used in mass programmes, because of its toxic potential. Proguanil is a causal prophylactic, primarily for P.f., but rapid development of resistance when used alone. A combined formulation of atovaquone (250 mg) + proguanil (100 mg) is commonly used as a prophylactic by Americans and other western travellers visiting malaria endemic areas Private prophylaxis Suppressive prophylaxis The schizontocides which suppress the erythrocytic phase and thus attacks of malarial fever can be used as prophylactics. Though the exoerythrocytic phase in case of vivax and other relapsing malarias continues, clinical disease does not appear. Chloroquine (CQ) In travellers, start one week before and continue till one month after return from endemic area. However, it can be used as a prophylactic only in areas with CQsensitive P.f. (Mexico, Argentina, etc.) Mefloquine- started 1–2 weeks before and taken weekly till 4 weeks after return from CQ-resistant P.f. area, except mefloquine-resistant P.f. areas (Myanmar, Thailand,Cambodia, India). Doxycycline -100 mg daily starting day before travel and taken till 4 weeks after return. Use for short-term (maximum 6 weeks) visitors and those unable to take mefloquine. Chemoprophylaxis of malaria Chemoprophylaxis of malaria should be limited to short-term use in special risk groups, such as : Nonimmune travellers, Nonimmune persons living in endemic areas for fixed periods (army units, labour forces), Infants, children and pregnant women (falciparum malaria has serious consequences in the pregnant). Intermittent preventive therapy in the form of one dose pyrimethamine (75 mg) + sulfadoxine (1500 mg) each is 2nd and 3rd trimester (gap not < 1 month) is recommended by WHO only in areas with high P.f. endemicity (P.f. >30%) for pregnant women. Clinical cure High-efficacy drugs: Low-efficacy drugs: Artemisinin, Proguanil CQ, Pyrimethamine Amodiaquine Sulfonamides Quinine Tetracyclines Mefloquine Clindamycin Halofantrine Lumefantrine Atovaquone. The erythrocytic schizontocides are used to terminate an episode of malarial fever. The erythrocytic schizontocides are radical curatives for falciparum, but not for vivax or ovale malaria. Severe and complicated falciparum malaria Hyperpyrexia Fluid and electrolyte imbalance, Acidosis, hypoglycaemia, 1) Quinine prostration, Quinine + clindamycin 2)Artemisinin-based therapy (ACT): Cardiovascular collapse, Artesunate severe anaemia, Artemether spontaneous bleeding, Arteether pulmonary edema, haemoglobinuria, renal failure Parenteral (i.m./i.v.) drugs have to be used Chloroquine 1) CQ causes rapid fever clearance and disappearance of parasitaemia in patients of malaria caused by all P.ovale and P.malariae, most P.vivax It is the drug of choice for clinical cure of vivax, ovale and malariae malaria. 2) Extraintestinal amoebiasis 3) Rheumatoid arthritis Mefloquine Mefloquine is an effective drug to treat for multi-resistant P. falciparum. To limit the spread of MQ-resistance, current recommendation is to use it only in combination with artesunate For prophylaxis of malaria among travellers to areas with multidrug resistance; It is not recommended for prophylaxis in residents of the endemic area. Quinine Quinine is used orally for uncomplicated CQ-resistant malaria, and i.v. for complicated/cerebral malaria. - Uncomplicated resistant falciparum malaria - Complicated and severe malaria including cerebral malaria Drug of choice for falciparum malaria ARTEMISININ DERIVATIVES Artemisinin is the active substanse of Artemisia annua (wormwood). Active against P.falciparum resistant to all other antimalarial drugs Artemisinin derivatives (Artemisinins): Artemether Artesunate Arteether Arterolane Use: Uncomplicated falciparum malaria Severe and complicated falciparum malaria Proguanil (Chloroguanide) It is a relatively slow-acting erythrocytic schizontocide for both P.f. and P.v. Its combination with atovaquone is commonly used in Thailand, USA and some other countries as a fast-acting erythrocytic schizontocide for treatment of multidrug resistant falciparum malaria. Atovaquone-proguanil is also used by western travellers as a causal prophylactic while visiting CQresistant/multidrugresistant P.f. endemic areas. Sulfonamides-pyrimethamine Sulfadoxine 500mg + pyrimethamine 25mg tab: FANCIDAR The major importance of this combination is due to its efficacy against CQ-resistant P.falciparum. Primaquine Active against the preerythrocytic stage of P. falciparum Marked effect on primary as well as secondary hepatic phases of the malarial parasite. It is highly active against gametocytes and hypnozoites. Tetracycline and Doxycycline These antibiotics have weak erythrocytic schizontocidal action against all plasmodial species including CQ, MQ and S/P resistant P. falciparum. Tetracyclines are never used alone to treat malaria, but only in combination with quinine or artesunate to treat mefloquine/chloroquine/S/P-resistant falciparum malaria 100 mg/day is used as a 2nd line prophylactic for shortterm travellers to CQ-resistant P. falciparum areas. Tetracyclines are not to be given to children and pregnant women