Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
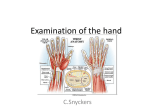
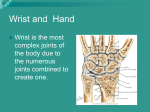
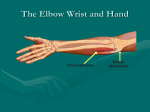
Wrist Anatomy Bones Quiz - What bones comprise the wrist? Joints Quiz - What joints comprise the wrist? Carpal Bones and Articulations Proximal Row Where can you palpate these? Scaphoid Lunate Triquetrum Pisiform Radiocarpal joint Distal Row Ulnocarpal joint Intercarpal joints Where can you palpate these? Trapezium Trapezoid Capitate Hamate Intercarpal joints Carpometacarpal joints (related to hand) Articulations and ROM Distal Radioulnar joint Supination and Pronation – 80-90o Ulna moves posteriorly and laterally with pronation Radiocarpal joint (and Ulnocarpal joint) Flexion (80-90o) and Extension (75-85o) Radial (20o) and Ulnar (35o) Deviation Intercarpal joints Gliding Soft tissue of Wrist Ligaments Covered by a fibrous capsule Radial and ulnar collateral limit ulnar and radial deviation; collectively limits flexion and extension Intercarpal and Carpometacarpal Soft tissue of Wrist Ligaments Dorsal – limits flexion Dorsal Radiocarpal Palmar - limit extension Transverse carpal ligament Palmar radiocarpal Multiple divisions Palmar ulnocarpal ligament Multiple divisions Soft tissue of Wrist Cartilage Triangular Fibrocartilage Complex – TFCC “Meniscus” between ulna and triquetrum Ulnar collateral ligament and palmar ulnocarpal ligaments have attachments Compressed with Pronation and Extension Compressed with Ulnar deviation Muscle Tissue of Wrist Extensor muscles Extensor Retinaculum What’s its function? Muscles innervated by radial nerve There are 8 Name them… Flexor Muscles Flexor retinaculum (aka transverse carpal ligament) Two compartments Superficial – 4 Deep – 3 Name them… Innervated by median and ulnar nerve EXTENSORS FLEXORS Wrist and Hand Anatomy Nerves/Vessels Radial & ulnar artery and veins Radial, ulnar, & median nerves Carpal Tunnel Flexor Tendons - 9 Median Nerve Wrist Injuries Strains Onset usually acute – FOOSH or Overexertion S/S: Active ROM limited Wrist Ganglion Herniation of the joint capsule or synovial sheath of a tendon. Tx: Bible Therapy Wrist Injuries deQuervain’s Disease - thumb/wrist stenosing tenosynovitis of the extensor pollicis brevis and abductor pollicis longus. S/S: crepitation, tenderness, strength loss. Special Test: = Finkelstein’s test Tx: RICE, NSAIDs Wrist Injuries Sprains Onset is usually acute – FOOSH or overexertion Often diagnosed when other injuries are ruled out S/S: Laxity, pain, swelling, limited ROM Both active and passive ROM are effected Pain is usually with overstretching Special Tests: Varus/Valgus, Carpal Glide PRICE, Rehabilitation, Taping for prevention Wrist Injuries Triangular Fibrocartilage Injuries - TFCC Onset is usually acute MOI: Forced hyperextension of wrist with loading S/S: Pain with pronation/extension and/or ulnar deviation; Pain with loading; Point tenderness; Swelling; Altered joint mechanics Special Test: Valgus test elicits pain but no laxity and Varus test compresses and causes pain Immobilization and Surgery are often necessary Neural Injuries Carpal Tunnel Syndrome Compression of median nerve Fibrosis of the synovium of flexor tendons secondary to tenosynovitis MOI: Insidious onset with repetitive wrist movement (and finger movement); Acute onset with trauma; Progressive degeneration S/S: numbness palmar thumb, index, middle fingers, dull ache, weak finger flexion (grip). May worsen with sleep. Poor posture may predispose. Special Tests: Tinel’s sign and Phalen’s Tx: Conservative (PRICE, NSAIDs) and Surgical Neural Injuries Biker’s Palsy Ulnar nerve compression Ulnar nerve passes through tunnel of Guyon between pisiform and hamate. MOI: repetitive jarring or pressure, repetitive flx/ext/ulnar deviation Tx: Padding (Gloves), Ice, NSAIDs Drop Wrist Syndrome Radial nerve compression at elbow Inability to extend wrist and fingers Wrist Injuries Wrist Fractures Distal Radius/Ulna and Forearm Fractures Onset is acute MOI: Hyperextension or hyperflexion combined with rotatory motion – FOOSH S/S: Deformity felt and observed; Crepitus Evaluated Neurovascular status Tx: Splint, Ice, Referral Wrist Injuries Wrist Fractures Distal Radius/Ulna Colles’ Fracture MOI: hyperextension-fall on outstretched S/S: “silver fork deformity” - radius & ulna posteriorly Smith’s Fracture (Reverse Colles) MOI: hyperflexed S/S: “garden spade deformity” - radius & ulna anteriorly Wrist Injuries Wrist Fractures Scaphoid - most common carpal MOI: fall on outstretched hand S/S: wrist aches, pain in anatomical snuff box, painful handshake or with overpressure Tx: Splint, Referral, Ice Plain X-rays may not be enough Immobilization (long and/or short) – 12 weeks Risk: aseptic necrosis and nonunion fractures Preiser’s Disease Surgery may be necessary Wrist Injuries Wrist Dislocations Radius or Ulna Lunate is very common MOI: force hyperextension Dorsal displacement = perilunate dislocation Palmar displacement (total rupture) = lunate dislocation S/S: Deformity, 3rd Knuckle is lower (Murphy’s sign), Paresthesia of middle finger, weak finger flexion Risk: Untreated or repeated trauma Kienbock’s Disease Decreased grip, pain with ulnar deviation, weak extension, pain with passive 3rd finger extension Immobilization – 6-8 weeks; Surgery may be necessary Wrist Injury Prevention Good technique! But…these help Flexor tendon arrangement Lumbricals Palmar Interossei Dorsal Interossei 4 3 2 1 Extensor Hood, Long extensor tendon, and lateral bands Finger flexor tendons Unique finger Look at pulley system Observation Relaxed position of hand Fingers slightly flexed Relative shortness of finger flexors Skin and Nail health Discoloration, texture, hair patterns Finger alignment Tips of fingers should align with finger flexion Hand abnormalities Finger and metacarpal positioning Muscle atrophy Range of motion Range of Motion Carpometacarpal Flexion (70-80o)/Extension Abduction (70-80o)/Adduction Opposition Metacarpophalangeal Flexion (85-105o)/Extension (20-35o) Abduction/Adduction (20-25o) Interphangeal joints Thumb flexion (80-90o) PIP flexion (110-120o) DIP flexion (80-90o) Palpation Metacarpals and joints Collateral ligaments of MCPs Phalanges and joints Collateral ligaments of PIPs and DIPs Thenar compartment muscles Thenar webspace muscles Central compartment Palmar fascia and muscles Hypothenar compartment muscles Pathology Tendon pathology Trigger Finger/Thumb Mallet Finger Boutonniere Deformity Jersey Finger Dupuytren’s Contracture Swan Neck Deformity Dupuytren’s Contracture Joint pathology Sprains Bony pathology Fractures Dislocations Swan Neck Deformity Tendon pathology Trigger Finger or Thumb Etiology Repeated motion of fingers may cause irritation, producing tenosynovitis Inflammation of tendon sheath (flexor tendons of wrist, fingers and thumb, abductor pollicis) Signs and Symptoms Thickening forming a nodule that does not slide easily Resistance to re-extension, produces snapping that is palpable, audible and painful Palpation produces pain and lump can be felt w/in tendon sheath Management Immobilization, rest, cryotherapy and NSAID’s Ultrasound and ice are also beneficial Injection Tendon pathology Mallet Finger (baseball or basketball finger) Etiology Signs and Symptoms Caused by a blow that contacts tip of finger avulsing extensor tendon from insertion Avulses extensor digitorum at distal phalanx Unable to extend distal end of finger (carrying at 30 degree angle) Point tenderness at sight of injury X-ray shows avulsed bone on dorsal proximal distal phalanx Management RICE and splinting in hyperextension for 6-8 weeks Tendon pathology Boutonniere Deformity Etiology Signs and Symptoms Rupture of extensor tendon dorsal to the middle phalanx – bone passes through central slip Forces DIP joint into extension and PIP into flexion Severe pain, obvious deformity and inability to extend DIP joint Swelling, point tenderness Management Cold application, followed by splinting in PIP extension and DIP flexion Splinting must be continued for 5-8 weeks Tendon pathology Jersey Finger Etiology Signs and Symptoms Rupture of flexor digitorum profundus tendon from insertion on distal phalanx Often occurs w/ ring finger when athlete tries to grab a jersey DIP can not be flexed, finger remains extended Pain and point tenderness over distal phalanx Management Must be surgically repaired Rehab requires 12 weeks and there is often poor gliding of tendon, w/ possibility of re-rupture Tendon pathology Dupuytren’s Contracture Etiology Nodules develop in palmer aponeurosis, limiting finger extension - ultimately causing flexion deformity Signs and Symptoms Dupuytren’s Contracture Often develops in 4th or 5th finger (flexion deformity) Management Tissue nodules must be removed as they can ultimately interfere w/ normal hand function Tendon pathology Swan Neck Deformity Etiology Distal tear of volar plate or finger trauma may cause Swan Neck deformity Signs and Symptoms Flexed MCP, extended PIP, and flexed DIP Pain, swelling w/ varying degrees of hyperextension Tenderness over volar plate of PIP Indication of volar plate tear = passive hyperextension Management RICE and analgesics Splint in PIP 20-30 degrees of flexion/DIP extension for 3 weeks; followed by buddy taping Joint pathology Sprains Phalanges Etiology Phalanges are prone to sprains caused by direct blows or twisting Signs and Symptoms Recognition primarily occurs through history Sprain symptoms - pain, severe swelling and hemorrhaging Joint pathology Gamekeeper’s Thumb Etiology Signs and Symptoms Sprain of UCL of MCP joint of the thumb Mechanism is forceful abduction of proximal phalanx occasionally combined w/ hyperextension Pain over UCL in addition to weak and painful pinch Management Immediate follow-up must occur If instability exists, athlete should be referred to orthopedist If stable, X-ray should be performed to rule out fracture Thumb splint should be applied for protection for 3 weeks or until pain free Splint should extend from wrist to end of thumb in neutral position Thumb spica should be used following splinting for support Joint pathology Sprains of Interphalangeal Joints of Fingers Etiology Signs and Symptoms Can include collateral ligament, volar plate, extensor slip tears Occurs w/ axial loading or valgus/varus stresses Pain, swelling, point tenderness, instability Valgus and varus tests may be possible Management RICE, X-ray examination and possible splinting Splint at 30-40 degrees of flexion for 10 days If sprain is to the DIP, splinting for a few days in full extension may assist healing process Taping can be used for support Joint pathology PIP Dorsal Dislocation Etiology Treated w/ RICE, splinting and analgesics followed by reduction After reduction, finger is splinted at 20-30 degrees of flexion for 3 weeks -followed by buddy taping Caused by twist while it is semiflexed Signs and Symptoms Pain and swelling over PIP Obvious deformity, disability and possible avulsion Management Etiology Signs and Symptoms Hyperextension that disrupts volar plate at middle phalanx PIP Palmar Dislocation Pain and swelling over PIP; point tenderness over dorsal side Finger displays angular or rotational deformity Management Treat w/ RICE, splinting and analgesics followed by reduction Splint in full extension for 4-5 weeks after which it is protected for 6-8 weeks during activity Open Dislocation Joint pathology MCP Dislocation Etiology Caused by twisting or shearing force Signs and Symptoms Pain, swelling and stiffness at MCP joint Proximal phalanx is angulated at 60-90 degrees Management RICE, following reduction splinting in slight flexion (3 weeks) Buddy taping following splinting Bony Pathology Metacarpal Fracture Etiology Signs and Symptoms Direct axial force or compressive force Fractures of the 5th metacarpal = Boxer’s Fracture Pain and swelling; possible angular or rotational deformity Management RICE, analgesics are given followed by X-ray examinations Deformity is reduced, followed by splinting - 4 weeks of splinting after which therapy starts Bony pathology Bennett’s Fracture Etiology Signs and Symptoms Occurs at carpometacarpal joint of the thumb as a result of an axial and abduction force to the thumb CMC may appeared to be deformed - X-ray will indicate fracture Athlete will complain of pain and swelling over the base of the thumb Management Structurally unstable and must be referred to an orthopedic surgeon Surgery and immobilization – season ending Bony pathology Distal Phalangeal Fracture Etiology Crushing force Signs and Symptoms Complaint of pain and swelling of distal phalanx Subungual hematoma is often seen in this condition Management RICE and analgesics are given Protective splint is applied as a means for pain relief Bony pathology Middle Phalangeal Fracture Etiology Signs and Symptoms Occurs from direct trauma or twist Pain and swelling w/ tenderness over middle phalanx Possible deformity; X-ray will show bone displacement Management RICE and analgesics No deformity - buddy tape w/ splint for activity Deformity - immobilization for 3-4 weeks and a Bony pathology Proximal Phalangeal Fracture Etiology May be spiral or angular Signs and Symptoms Complaint of pain, swelling, deformity Inspection reveals varying degrees of deformity Management RICE and analgesics are given as needed Fracture stability is maintained by immobilization of the wrist in slight extension, MCP in 70 degrees of flexion and buddy taping Lacerations Superficial location of tendons and nerves predisposes athletes to damage form shallow lacerations. Any laceration to the fascia below the cutaneous layer should receive a referral R/O trauma to tendons and nerves Prevent infection Suture to ensure minimal scarring Finger Nail Pathology Subungual Hematoma MOI: finger caught between two surfaces Presents with bleeding under nail bed Draining – Drill or Cauterize Paronychia Infection around fingernail beds S/S: Redness, pain, drainage Warm soaks (Betadine), Antibiotic, Referral Changes in normal appearance - indicative of a number of different diseases Scaling or ridging = psoriasis Ridging and poor development = hyperthyroidism Clubbing and cyanosis = congenital heart disorders or chronic respiratory disease Spooning or depression = chronic alcoholism or vitamin deficiency Prevention of Hand Injuries Protection Gloves, Grips, Braces Proper Technique Sport and Ergonomics Physical Conditioning Reps and Sets for muscles of Hand Theraputty, Wrist curls/extensions, Fist pumps Problem Solving Putting it together with Case studies History What is the cause of pain? Mechanism of injury? Previous history? Location, duration and intensity of pain? Creptitus, numbness, distortion in temperature? Sounds or sensations? Technique changes? Weakness or fatigue? What provides relief? Observation Functional Evaluation Range of motion in all movements of wrist should be assessed Wrist “attitude” How do the carpals and metacarpals align with the distal radius and ulna? Is there symmetry? How are those tendons looking? Active, resistive and passive motions should be assessed and compared bilaterally Wrist - flexion, extension, radial and ulnar deviation Is there a palmaris longus? - 10% of population it is absent Become a “palm reader”? Palpation Bony and Soft Tissue Palpation Are they where they should be? Do they feel like they should feel? Circulatory and Neurological Evaluation Hands should be felt for temperature Cold hands indicate decreased circulation Take pulse – radial artery Pinching fingernails can also help detect circulatory problems (capillary refill) Hand’s neurological functioning should also be tested (sensation and motor functioning) Is it nerve? What other test is common for nerve injury? How else can you detect a neural injury? What test is this? Is it the ligaments or joints? Which tests are these? What are some distinguishing characteristics of a ligament or joint injury? Is it muscle or tendon? How do you assess the function of a muscle? What are some distinguishing characteristics of a muscle injury? What test assesses these structures? Is it bone? What is are distinguishing signs of a potential fractures? Case study #1 A 28 year old woman complains of pain in the right hand over the last 3 months. She reports numerous FOOSH incidents and currently works as a cashier at a grocery store. The pain awakens her at night and is relieved only by vigorous rubbing of her hand and motion of the fingers and wrist. There is some tingling in the index and middle fingers. What is your assessment plan? Case study #2 A 18 year old boy reports with wrist pain and swelling on the dorsum of his wrist and hand. He notes the pain is more near the base of the thumb. He is an active weightlifter. He says he tripped and experienced a FOOSH while playing recreational football. He states that after the injury the wrist hurt, he rested 2 days and iced, the pain decreased, but then with weightlifting the swelling has developed the last 5 days. Now it is very swollen and painful. What is your assessment plan? Case study #3 A 22 year old golfer comes to you with pain along his right medial wrist. He reports that while on spring break he went skiing and had a FOOSH. The wrist was achy but didn’t bother after a few hours especially since he put snow on it for 20 minutes. Now that he has returned to school and golf practice he is having trouble controlling his drives and long iron shots because of pain in his wrist at the top of the swing. What is your assessment plan?