Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
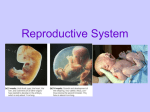
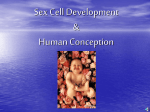
Biology 30 Unit B – Reproduction and Development General Outcome B1: Students will explain how survival of the human species is ensured through reproduction Reproductive System • sexual reproduction involves the union of 2 gametes to form a zygote • the male gamete is the sperm • the female gamete is the egg or ovum • both gametes are haploid (n) - contain half the regular number of chromosomes 23 • all other body cells - somatic cells are diploid (2n) - contain 46 chromosomes • sexual reproduction is the preferred method of reproduction in living organisms because it is continually mixing up the genetic information which results in NO two individuals being genetically identical Male Reproductive System Provide labels for the following diagrams. (Note: Some labels appear twice.) 1. 2. 3. 4. 5. 6. 7. Provide labels for the following diagrams. 8. 9. 10. 11. 12. 13. 14. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. • the male gamete or sperm cell is produced in the testes • the testes are located outside the core of the body in the scrotum • sperm cells need to be produced at a few degrees cooler than the body temperature to be healthy • shortly before birth the testes which form in the abdominal cavity descend into the scrotum • if the testes do not descend it must be corrected by surgery prior to puberty or the male will be sterile • the testes are composed of small tubules called seminiferous tubules (250 m) within which the sperm cells are produced • Spermatogenisis, the formation of sperm cells, takes about 65-75 days in the human male. • Diploid cells that begin the process are located near the outer wall of the tubules called spermatogonia • These cells multiply constantly by mitosis into primary spermatocytes, the cells that will then undergo meiosis in two stages. • Meiosis I of a primary spermatocyte produces two secondary spermatocytes, each with the haploid number of chromosomes (n), 23 in humans. • The chromosomes are still in their duplicated state, each consisting of two identical chromotids. • Meiosis II then form four cells, each with the haploid number of single chromatid chromosomes called spermatids • A sperm cell develops by differentiation of each of these four haploid cells and is gradually pushed toward the centre of the epididymis tubule, where it matures and become motile. • Sperm are stored in the epididymis until ejaculation • sertoli cells nourish the developing sperm cells • interstitial cells located in between the seminiferous tubules produce testosterone • during sexual intercourse the sperm cells move along the vas deferens to the urethra • three glands add fluid in with the sperm cells 1. seminal vesicle 2. prostate gland 3. Cowpers gland • this fluid has the following functions 1. fluid for the sperm cells to swim in 2. chemical protection 3. nourishment – contains fructose 4. alkaline – to neutralize the acid of the urethra and the vagina • the combination of sperm and fluid is called semen • 3 - 4 mL of semen contain about 400 000 000 sperm cells General Outcome B2: Students will explain how human reproduction is regulated by chemical control systems Male Hormones • Testosterone – produced in the interstitial cells (in between seminiferous tubules) o Stimulates the maturation of the testes, penis and spermatogenesis o Secondary sex characteristics • Gonadotropic hormones – regulate the functions of the testes. o FSH – stimulates sperm cells in seminiferous tubules o LH – testosterone production in the interstitial cells o GnRH (gonadotropic Releasing Hormone) – beginning at puberty, released by the hypothalamus LH o Inhibin – secreted by sertoli cells inhibits FSH roduction and reduces GnRH production Understanding the Regulation of Male Sex Hormones An experiment was performed in which the circulatory systems of two male mice (A and B) with compatible blood types were joined (Figure 7). The data analysis from the experiment is shown in Table 4. (Note that + indicates “found,” – indicates “not found.”) Blood vessels connecting mice A Pituitary gland Testes removed B Pituitary gland removed Testes present Figure 7 Circulatory systems of two mice are joined. Table 4 Presence of Hormones and Sperm in Joined Mice Animal A B Testosterone + + LH + + FSH + + Sperm in Urethra + (a) State the purpose of the experiment (b) Write a hypothesis for the experiment. (c) Write a design statement for the experiment. In your statement, identify one manipulated variable and one responding variable. Evaluation (d) Why were the circulatory systems joined? (e) If LH and FSH are produced in the pituitary gland, explain how it is possible to find these hormones in mouse B. (f) Explain why testosterone is found in both mice. (g) Why is sperm found in the urethra of mouse B but not in the urethra of mouse A? Table 5 Presence of Hormones and Sperm in Two Mice Animal A B Testosterone - LH + - FSH + - Sperm in Urethra - Synthesis (h) In another experiment, the circulatory systems of the two mice were not joined and the data in Table 5 were collected. Predict which glands and organs are present or absent from each animal. Give reasons for your prediction. Thought Lab 14.2: Testosterone and Male Development Procedure 1. Examine the data in the table below. Graph these data using the type of graph you think is most appropriate. 2. Normal Blood Testosterone Levels in Males Age (years) 1 to 7.9 8 to 10.9 11 to 11.9 12 to 13.9 14 to 17.9 18 to 29 Blood testosterone level (ng/dL) 40 42 260 420 1000 1100 3. Based on the data, at what age does puberty begin? Mark this on your graph. 4. Use print or Internet resources to research the physiological changes that take place during male puberty. Write a brief description of the changes that are associated with changing levels of testosterone. Identify which of these changes are directly related to reproductive function. Analysis 1. Is it possible to use blood hormone data to identify the end of puberty? Explain your answer. 2. In young men, the growth of facial hair begins at the same time as blood testosterone levels start to increase. a) From this evidence, can you conclude that testosterone causes facial hair growth? Justify your answer. b) Design an experiment to test the hypothesis that testosterone causes facial hair growth in men. Female Reproductive System Provide labels for the following diagrams. Note that some labels appear more than once. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. • the female gonads are the ovaries • the ovary is loosely attached by ligaments to the uterus and abdominal cavity • each ovary contains about 400 000 follicles each follicle contains a primary oocyte • Follicle - structure in the ovary that contains the oocyte • Oocyte – immature ovum (egg cell) • only about 400 of these will mature over the females life span • a primary oocyte originated from an oogonium cell • primary oocytes have started to undergo meiosis but stopped part way until maturity • by 20 weeks the female as produced all the oocytes for their entire life • starting at puberty one follicle matures every 28 days • the follicular cells left behind develop into the corpus luteum • the corpus luteum a yellowish mass of cells produce progesterone • the corpus luteum degenerates if no pregnancy occurs • fimbrae waving draws the ovum into the fallopian tube (oviduct) • the ovum moves along the fallopian tube by cilia waving and by peristalsis • the ovum is viable for about 24 hours • fertilization normally occurs in the first third of the tube • the uterus is about the size and shape of a pear • its upper end is free-floating, lower end is embedded in the pelvis wall • it is supported by suspensory ligaments • rests on top of the urinary bladder • the uterus is made of three layers of tissues 1. peritoneum - outer layer -connective tissue 2. myometrium - middle layer -smooth muscle 3. endometrium - inner layer • this layer changes throughout the menstrual cycle • the cervix is the opening into the uterus from the vagina • the cervix is susceptible to cancer (reason for pap smears) Female Hormones 1. FSH - from the pituitary gland • stimulates primary follicle to develop into a secondary follicle • indirectly causes estrogen to be produced 2. Estrogen - produced by developing follicular • at puberty is responsible for secondary sexual characteristics a) body hair b) breast development d) deposition of fat • during the menstrual cycle it stimulates the growth and development of endometrium 3. LH - from the pituitary gland • stimulates ovulation • causes the old follicle cells to develop into corpus luteum • indirectly causes progesterone to be produced 4. Progesterone - produced by corpus luteum • influences maintenance of endometrial lining • inhibits contraction of smooth muscles of uterus • inhibits development of new follicle • influences slight enlargement of mammary glands ** if fertilization and implantation occurs progesterone will be produced and secreted for two to three months *** if fertilization does not occur the corpus luteum shrinks after 10 days 5. Oxytocin - initiates contractions of the uterus at the end of pregnancy • causes milk secretion after birth 6. Prolactin - causes milk production 7. Relaxin - causes ligaments of pelvis to stretch to allow for birth 8. HCG - Human Chorionic Gonadotropin • tells the corpus luteum to keep producing progesterone • shows up in urine 14 days after fertilization • gives positive pregnancy test Menstrual Cycle • means of preparing the uterus each month for possible implantation of a blastocyst • starts up at puberty when the pituitary secretes FSH • lasts until menopause (around 45-55) • normally averages 28 days • stress, health, drugs may interrupt the cycle • four distinct phases: 1. Menstrual Period – Flow Phase • lasts for 5 days (day 1 to day 5) • is the shedding of the old endometrium • blood loss means loss of iron which must be replaced • this starts the development of a follicle in one ovary • the follicle begins to produce estrogen 2. Follicular Phase • lasts from day 6 to day 13 • estrogen causes the endometrium to start building up again • an ovum matures inside the follicle and the follicle swells • this phase ends with ovulation • just prior to ovulation, the body temp. takes a drop followed by a rise • LH starts to be released 3. Ovulatory Phase Day 14 oocyte ruptures from the ovary 4. Luteal Phase • lasts from day 15 to day 28 • the ovum travels down the fallopian tubes waiting to be fertilized • the follicle transforms into the corpus luteum • the corpus luteum secretes estrogen and progesterone • high levels of progesterone maintains the endometrium and inhibits smooth muscle contraction of the uterus • normally the ovum is not fertilized and it degenerates - so no gonadotropic hormones are produced • the corpus luteum stops functioning - progesterone and estrogen levels drop • low progesterone levels - endometrium starts to come off uterus - menstruation • rapidly dropping progesterone levels cause uterus contractions - menstrual cramps • the cycle starts over Procedure 1. Study the graphs, and observe how the levels of hormones affect each other as well as the follicle and endometrium. 2. Use the Analysis questions to analyze and interpret the graphs. Analysis 1. During which days of the menstrual cycle does the level of FSH increase? What happens to the follicle during this time? 2. On which day is the level of LH in the bloodstream at its highest? What event occurs immediately after this peak? 3. What event is associated with the decline of LH in the blood? 4. During which days of the cycle does the level of estrogen in the blood increase most rapidly? What happens in the uterus during this time? 5. During which days of the cycle does the level of progesterone in the blood increase most rapidly? What happens in the uterus during this time? 6. During which days of the cycle are the levels of estrogen and progesterone at their lowest? What happens in the uterus during this time? Conclusions 7. How do increased levels of estrogen and progesterone appear to affect the level of FSH in the blood? 8. Do the names of the hormones FSH and LH correspond to their functions? Explain your answer. 9. Select and use an appropriate mode of representation to compare and contrast the functions of estrogen and progesterone in the menstrual cycle. General Outcome 3: Students will explain how cell differentiation and development in the human organism are regulated by a combination of genetic, endocrine and environmental factors. Fertilization and Pregnancy Provide labels for the structures represented by 1-12. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. • 2 events must happen for pregnancy to occur o the ovum must be fertilized by a sperm while in the first third of the fallopian tube forming a zygote (diploid) o the fertilized egg must implant itself in the endometrium • as the zygote moves along the fallopian tube it begins to undergo mitosis over and over • the sperm cells must travel from the vagina, through the cervix and into the uterus. • Only a few hundred reach the fallopian tubes • The zygote requires 3-5 days to travel from the fallopian tube to the uterus Label the following diagram. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. • Through its journey through the fallopian tube, cleavage occurs: equal cell division of the cells of the zygote without any increase in size – cells become progressively smaller • by the time it reaches the uterus it is a blastocyst – an early stage of embryo development - a fluid filled structure • implantation occurs – zygote embeds in the endometrium approximately 8-9 days after ovulation • 4 days after fertilization the zygote is referred to as an embryo • Once implantation occurs the endometrium must be maintained • For this to occur ovarian hormones (progesterone & estrogen) levels must be maintained but they have a negative feedback effect on gonadotropic hormones (LH &FSH) • LH is needed to sustain the corpus luteum which sustains progesterone and estrogen levels and therefore preventing uterine contractions and the shedding of the endometrium. • blastocyst hormones replace LH • the outer layer of the blastocyst contains two extraembryonic structures chorion produce hCG - human chorionic gonadotropic hormone o maintains the corpus luteum for the first three months o pregnancy tests identify hCG levels in the urine o chorion will contribute to the development of the placenta amnion - fluid-filled extraembryonic structure o between the amnion and the embryo is the amnionic cavity – a fluid filled sac that insulates the embryo/fetus o protecting it from • yolk sac - temporary function producing blood cells for embryonic circulatory system, later contributes to the primitive digestive tract Label the following diagram. 1. 2. 3. 4. 5. 6. 7. 8. Placenta • large mass of tissue • develops from cells of the embryo in contact with the endometrium • at the 4th month it will produce estrogen and progesterone • high levels of progesterone will prevent further ovulation • chorionic villi – vascular projections of the chorion that provide a barrier between mothers blood and fetal blood • contains blood vessels of the mother on one side and the fetus on the other • allows exchange of gases, wastes, nutrients, hormones and antibodies • mother’s blood and baby’s blood should never come in direct contact • allantois - provides umbilical vessels for placenta • umbilical cord attaches the fetus to the placenta umbilical cord o 1 vein - oxygen, nutrients o 2 arteries - CO , wastes Nourishing the Embryo In the placenta, chorionic villi that extend from the embryo are in contact with pools of blood from the mother. Nutrients and oxygen pass by diffusion from the maternal blood to the embryo, and wastes diffuse in the opposite direction • Morphogenesis – development of an organism or part of it • Two parts: o Growth o differentiation (cell specialization) First Trimester – fertilization to end of week 13 • Period of very rapid cell division and specialization • Gastrulation – formation of a three layered structure (gatrula) from the two layered blastoycst • Three main layers of cells give rise to the various tissues of the body • Ectoderm – outer layer o Nervous, salivary gland, pituitary, skin, hair, nails • Mesoderm – middle layer o Connective tissue, bone, muscles, blood, kidney, reproductive organ • Endoderm – inner layer o digestive tract, lungs, liver, pancreas, thyroid, parathyroid, bladder, lining of digestive tract and respiratory tract. Gastrulation The changes that are illustrated in these diagrams take place over a period of about one week. Gastrulation—the formation of the three primary germ layers—is a pivotal event in embryonic development. All future tissues, organs, and organ systems of the body will develop from the cells of the germ layers. Organ Formation from the Primary Germ Layers o At the end of 8 weeks – 3.5 cm long o Begins to form the first bone cells- yolk sac no longer needed During the first eight weeks (56 days) after ovulation, the appearance of various internal and external features may be used to describe the development of the embryo. The eight weeks are divided into 23 embryonic stages, also known as Carnegie stages. Embryologists use the Carnegie stages to make statements about development that are more specific than reference to size or age allow, since the moment of conception cannot be determined precisely. • Main organ and systems developed o Heart has formed o Brain taking shape o Limb buds with tiny toes and fingers visible – arms and legs begin to move, sucking reflex evident o By 9th week is referred to as a fetus 6 weeks 9 weeks Second Trimester – 14th to 27th week • All organs formed, but not fully developed • Development continues and fetus size increases • 6th month eyelids and eyelashes evident • Bone cells form from cartilage • If labour is induced at the end of the second trimester there is a chance the fetus will survive 14 weeks 20 weeks Third Trimester – 28th week to 40th week • Rapid growth • Organ systems established • Body mass increase as organs enlarge and finish development Hormone Levels During Pregnancy Effects of Environmental Agents on Embryonic Development Fetal Alcohol Spectrum Disorder The placenta is a selective barrier that prevents the mother’s blood cells from entering the circulatory system of the fetus. Smaller molecules, however, can move across the membrane. Unfortunately, some harmful agents, such as alcohol, are smallenough to cross the placenta. When a mother takes in alcohol, it crosses the placenta and enters the blood of the fetus (Figure 8). As the mother drinks, the fetus absorbs alcohol. The effects on the fetus are the same as those on the mother: alcohol impairs the functioning of the nervous system and it is a depressant. It is also a poisonous substance. Like other poisons, it is broken down by the liver. Unfortunately, the liver of a fetus is not fully developed until the very final stages of pregnancy, and alcohol cannot be broken down quickly. This means that alcohol remains in its most harmful form much longer in the fetus than it does in the mother. Not only can alcohol kill many of the cells of the fetus, but it has also been linked to changing a cell’s genetic information. Fetal alcohol spectrum disorder (FASD) is a host of birth defects associated with excessive alcohol consumption. Dr. Matthew Hicks, who researches FASD at the University of Calgary, indicates that although FASD is preventable, it is one of the most common birth defects in Canada. FASD crosses all cultural and ethnic boundaries, but occurs only in children born to mothers who consumed alcohol during pregnancy. Children with FASD may have physical abnormalities such as a low body weight, slowed development, deformed organs, a poorly formed rib cage, limited joint movement, and missing digits, as well as distinctive facial features such as a small head, thin upper lip, and small jaw bone. Symptoms of FASD can also include abnormalities of the nervous system, which can cause learning disabilities, poor hand and finger coordination, irritability in infancy, and hyperactivity in childhood. Approximately 60 % to 70 % of women who are alcoholics give birth to babies with FASD. What may be most disturbing is that evidence suggests that the problem may be getting worse. A 1997 study indicated that four times as many pregnant women admitted to “frequent” drinking in 1995 as compared with a similar 1991 poll. Among 1,313 pregnant women, 3.5 % said they drank an average of seven or more drinks a week or had consumed five or more drinks on at least one occasion in the previous month. Understanding the Issue 1. What is FASD? 2. Why are scientists concerned with decreasing the number of women who drink? 3. What are some symptoms of an FASD baby? Statement Pregnant women should be required to have blood tests on a regular basis to monitor drinking problems. • In your group, discuss the statement and the points and counterpoints in Table 4. Write down additional points and counterpoints that your group considered. • Decide whether your group agrees or disagrees with the statement. • Conduct research for information on FASD and other preventable birth defects. Table 4 Perspectives on Requiring Pregnant Women to Have Blood Tests Point Counterpoint FASD is the third most common reason for babies being born with mental retardation in Canada and the United States. Alcohol consumption affects mother and baby. Heart defects and defects of the nervous system are most common. The idea of suspending the rights of pregnant women is unbelievable. All people would hope that mothers would recognize their responsibility, but legislation is not the answer. Changes in attitudes are accomplished best through education. Despite a growing awareness that avoiding alcohol prevents the disorder, about one-fifth of pregnant women continue to drink even after they learn they are pregnant. Most birth defects occur in the period between two weeks and three months of development, when the organs are forming. Does this mean that women should be monitored to ensure that they have a wellbalanced diet? Many factors have been linked to birth problems by scientific studies. Parturition – act of giving birth (labour) • Signaled by uterine contractions • Cervix thins and begins to dilate • Amnion is forced into birth canal and burst (provides lubrication for the canal) – breaking of the water • Uterine contractions move the baby through the birth canal • Followed by the placenta • Relaxin – produced by the placenta prior to labour, causes ligaments within pelvis to loosen and the cervix to soften • Oxytocin – produced by the pituitary gland cause strong uterine contractions • Decreased levels of progesterone is believed to be crucial to the onset of labour • Prostaglandins trigger strong uterine contractions Positive Feedback Mechanisms Controlling Parturition Label the following diagram. 1. 2. 3. 4. 5. 6. The Three Stages of Parturition Lactation • During pregnancy estrogen and progesterone prepare the breasts for milk production • There are about 20 lobes of glandular tissue per breast • Each lobe has a small duct that carries fluid toward the nipple • Prolactin stimulate the breast to produce fluids • Estrogen has positive feedback on prolactin during pregnancy • However milk production is inhibited before birth as high levels of progesterone inhibits the action of prolactin • After birth estrogen and progesterone levels drop rapidly causing o Decreased amounts of prolactin o Increase in prolactin activity • Causes initially production of colostrum o Contains milk sugar and milk proteins o Lacks milk fat • Few days after birth prolactin stimulates the production of milk • Milk/colostrum supply vital antibodies for the baby • Milk release o Suckling action of the newborn stimulates a series of events to take place y gland cause the release of oxytocin Oxytocin will stimulate weak contractions of smooth muscle within the breasts forcing milk into the ducts oxytocin stimulates weak contractions in the smooth muscle of the uterus allowing it to return to prepregnancy size and shape • Milk production places a huge metabolic drain on the mother o Production of up to 1.5 L per day o Loss of 50 g – 100 g of lactose sugar o The mother would need to replace 2-3 g of calcium phosphate per day arathyroid gland enlargement Thought Lab 15.1: Folic Acid and Neural Tube Defects Abstract Objectives: To determine the diffusion of information about preventing neural tube defects (NTDs) through folic acid consumption by examining whether mothers of Canadian children born with spina bifida, who had become pregnant at least a year after evidence of the preventive effect of folic acid had been published, had taken sufficient amounts of folic acid in the periconceptional period [that is, the first few weeks of pregnancy] and were aware of this important new information. Design: Validated food-frequency questionnaire to assess folate intake. Setting: The Hospital for Sick Children in Toronto between Jan. 4 and Aug. 16, 1994. Participants: Thirty mothers whose infants were being treated for spina bifida. Main outcome measures: The mothers’ mean folate intake and knowledge about the protective effect of folic acid; demographic and health information. Results: The mothers’ mean folate intake was 0.182 mg/d (standard deviation 0.076 mg/d, range 0.02 to 0.53 mg/d), less than half the protective dose. Only 4 (13%) of the mothers had been aware of the relation between nutritional folate and NTDs when they conceived, but even they did not supplement their diets with sufficient folic acid. The medical data showed that, in addition to the failure of primary prevention of NTDs, secondary prevention through diagnostic tests during pregnancy were also inadequate. Conclusions: Our study, one of the first to be conducted after the role of folate in preventing NTDs was confirmed, reveals that, in one of the most advanced countries in the world, this new information has had no effect on patients’ folate intake. Unless food is fortified with folate, the estimated 400 to 800 annual cases of NTDs in Canada will not be prevented. Procedure 1. Read the abstract, which was published in Clinical and Investigative Medicine in 1996. You may need to look some words up in a print or electronic dictionary. Even if you do not understand every word or some of the sentences, you should still be able to “pick out” the general meaning or significance of what the authors of the journal article are saying. 2. Using print or electronic resources, conduct further research on neural tube defects to find out the following. what kind of defects can occur, how often they occur statistically in Alberta and/or Canada, their characteristics/symptoms, and what, if any, treatments are available for them why Canada’s health agency was reluctant to advise fortifying foods with folic acid, and the current status of folic-acid fortification actions taken on the part of Health Canada to inform the public about folic acid and NTDs Analysis 1. What is the recommended daily amount of folic acid for women who could become pregnant? 2. When should women who could become pregnant start taking folic acid? 3. Why is dietary (unsupplemented) intake of folic acid considered to be inadequate to prevent NTDs? 4. What other risk factors are involved in having a baby with an NTD? Birth Control Pill • contains estrogen and progesterone • interferes with pituitary hormones by keeping estrogen levels high – no progesterone produced or FSH (NFB) • stops ovary from developing egg • less endometrium builds up so less will be sloughed off • 21 pills with 7 blanks Morning After Pill • initiates the ‘period’ • contains high estrogen and progesterone • interferes with endometrium • prevents implantation of a blastocyst • interferes with development of corpus luteum • progesterone levels drop • must take within 3 days of unprotected sex • 2 pills + 2 more within 12 hours. Rates of STI Infection in Alberta Examine the graphs shown below. Beside each graph, write an interpretation of the data presented. 1. 2. 3. 4. 5. Thought Lab 14.1: STI’s: What to Know and How to Know It Procedure 1. In your group, choose one STI that will be the focus of our education program. 2. Use print and Internet resources to learn about the STI you chose. In particular, find out what effects the STI can have on the male and female reproductive systems. ICT 3. Organize your findings in a written report. Your report should include the following information: the cause of the STI the effects of the STI on the human body and, in particular, the male and female reproductive systems why young adults are the age group at greatest risk for acquiring an STI the issues and challenges involved in preventing and controlling the transmission of the STI 4. Using the information in your report, develop an education program aimed at young people. Decide on the two or three most important messages. Then decide how you will deliver these messages. For example, you could create print advertisements for a magazine, produce a music video, or write and perform a play. Deliver your presentation to your class. Analysis 1. Which STIs are most likely to disrupt the function of the human reproductive system? 2. Which STIs are most likely to cause permanent damage to the human reproductive system? 3. Which education program do you think was the most effective? What made it effective? 4. What do you think are the most serious challenges for health practitioners who want to reach young people in Canada? What could be done to meet these challenges? Thought Lab 15.2: Evaluating Reproductive Technologies: Safety and Effectiveness Procedure 1. Working in small groups, select at least three of the technologies from each column of the following table. (Therefore, you will select a minimum of six technologies.) Selected Technologies for Enhancing Conception • artificial insemination (AI) • assisted hatching (also called laser assisted hatching) • gamete intrafallopian transfer (GIFT) • in vitro fertilization (IVF) • intracytoplasmic sperm injection (ICSI) • surrogacy • tubal embryo transfer (TET) • zygote intrafallopian transfer (ZIFT) Selected Technologies for Preventing Conception • condoms • fertility awareness methods • intrauterine device (IUD) • lactational amenorrhea (LAM) • oral contraceptives (pills containing both estrogen and progestin (synthetic progesterone)) • progestin-only contraceptives • spermicides • tubal ligation • vasectomy 2. With the members of your group, discuss the meanings of the terms “safety” and “effectiveness” as they apply to reproductive technologies. Develop preliminary definitions for these terms. 3. Conduct research to find data or information about the safety and effectiveness of each of the technologies you have selected. 4. In the course of your research, you may find that your definitions of the terms “safety” and “effectiveness” require modification or replacement. Redefine these terms with the members of your group. Then consult with other groups to compare definitions. As a class, develop definitions that everyone can agree to use. 5. Reexamine the information and data you have gathered in light of the class definitions of safety and effectiveness. As necessary, conduct additional research to refine your findings. 6. Consult with other groups to prepare a master chart that summarizes findings for all the technologies investigated. Analysis 1. Based on your research, what key factors influenced your definitions of “safety” and “effectiveness”? List them in order of priority. What seems to be considered an acceptable risk to take to conceive or prevent conception of a child? 2. Based on your research and the summary in the master chart, decide which conception-enhancing and which conception-preventing technology is the most safe and effective technology. Use clear and logical arguments to justify your opinion. (You may answer this question as a group, as an individual, or both.) Extension 3. List three other factors that you think would affect a person’s or a couple’s determination of the best course of action for enhancing or preventing conception. Extension Some strategies to control the spread of STIs raise social and ethical issues. For example, some people argue that people should be able to test themselves for STIs in the privacy of their own homes. Other people believe that tests should always be conducted in a health clinic so that the results can be recorded. Working with a partner, choose an ethical issue associated with STIs. Prepare a short debate to argue both sides of the issue. What did you conclude?