Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
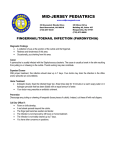
BUKOVINIAN STATE MEDICAL UNIVERSITY DEPARTMENT OF PATIENTS CARE AND HIGHER NURSE EDUCATION “APPROVED” on the methodical conference of department of patients’ care and higher nurse education “ ” ________ 200_ protocol N __ Chief of department, associate professor I.A. Plesh METHODICAL INSTRUCTION FOR SELF-PREPARATION OF STUDENTS TO PRACTICAL CLASS №12 SURGICAL INFECTION. Discipline: nursing in surgery for 3nd year students of medical faculty №4, specialty "nurse business'' Methodical instruction was prepared by: Assistant Riabyi S.I. Chernivtsi - 2010 1. Topic: SURGICAL INFECTION. (Classification of surgical infection. Protective reaction of organism against surgical infection. General and local signs. Phases of purulent diseases. General principals of treatment of purulent diseases. General notions about main purulent diseases. General notions about main diseases, witch caused anaerobic infection. The main peculiarities of individual care of patients’ with anaerobic infection. Care of patients’ with AIDS, peculiarities of doing nurse’ manipulation, dressing etc.). 2. Duration of the class: 2 academic hour. 3. Study aim: 3.1. The student should know: Definition, classification of a panaritium, a phlegmon of hand; A clinical picture of a panaritium, a phlegmon of a hand; Diagnostics and treatment of a panaritium, a phlegmon of a hand. An etiology, a pathogeny acute hematogenous osteomyelitis; Diagnostics and medical tactics of purulent diseases of bones; Kinds of operative treatment;Chronic forms of osteomyelitis, their treatments; An etiology, a pathogenesis, methods of diagnostics, the basic clinical attributes of a tetanus, antrax, diphtherias of wounds; Methods of specific prophylaxis and treatment of an acute specific surgical infection. 3.2. The student should be able: to collect an anamnesis; to lead objective inspection of the patient; to distinguish the basic clinical attributes of purulent diseases of fingers and hands; to lead diagnostics of an acute purulent pathology of fingers and hands on their kind and localization; to prove the plan of individual treatment (conservative and surgical); to give the reference on an aftertreatment of patients. 3.3. The student should master practical skills: 4. first aid in case of surgical infection; dressing patients with purulent wounds; dressing patients with anaerobic infection; dressing patients with AIDS; assistance during cutting of boils; Advice for students: HAND INFECTIONS Paronychia. This condition starts as a subcuticular or intracutaneous infection, with exudate developing in a localized area, which eventually spreads around under the base of the fingernail, elevating it from the nail matrix and eventually the nail bed (Fig. 1). Fig. 1 Paronychia:. 1. The pus collections near the nail; 2. The pus spreading under nail If a small collection of purulent material cannot be localised "and expressed, complete drainage is indicated as early as possible by an incision that allows the lateral and proximal folds of the nail to be exposed. This may be done under digital block anaesthesia without the use of epinephrine in the anaesthetic. A pointed knife blade is inserted between the skin and the nail in order to incise the eponychium from within outward, on either side of the base of the nail. This allows the skin flap to be turned upward for adequate drainage. Wet dressings, petrolatum gauze, antibiotic ointments, and regular reopening of the drainage area will prevent the skin from adhering until infection has been controlled. If more extensive drainage is needed for a deeper abscess, the incisions are extended proximally.in the skin fold, the skin edges are raised upward along with the dorsal skin over the nail bed, and the proximal end of the fingernail is excised. A small segment of nail, rather than the entire fingernail, can be removed. The infection, if chronic and severe, may be sufficient to destroy the nail matrix, the nail bed, and ultimately the phalanx. Thus, in order to avoid loss of bone and even the phalanx, treatment should be complete, aggressive, and early. Incisions adjacent to the eponychium should be avoided, as the remaining skin flaps may necrose. Also, the incisions over the extensor tendons should be avoided, since these may cause direct extension of the inflammatory process. The nail matrix should not be damaged while the fingernail is being removed. When the new nail forms it may be somewhat irregular, and several months will elapse before a smooth nail regenerates. Chronic paronychia, particularly in the female, may be due to Candida or Manilla. Local treatment by ointments should be initiated; however, appropriate cultures should be obtained prior to extensive antibiotic therapy, if local treatment appears to be unsuccessful. Infection of the terminal pulp space (syn. Felon). Felon (Latin, fel-gali). An abscess near the nail. Pulp-space infection is the second most frequent infection of the hand (about 25 per cent of all cases). The index finger and the thumb are affected most often. The origin of the infection is usually a prick. Surgical anatomy. The deep fascia, which is attached to the thin skin of the distal flexion crease, fuses with the periosteum just distal to the insertion of the deep flexor tendon, thereby closing the terminal pulp compartment at its proximal end. Through the space, which is filled with compact fat, feebly partitioned by fibrous septa, run the terminal branches of the digital arterv. Thrombosis of these vessels accounts for the frequency with which osteomyelitis complicates infection of this closed space. The basal plate of the epiphysis is rarely involved. Clinical features. Dull pain, worse when the hand is dependent, and swelling are the first symptoms. Forty-eight hours later there are severe noctual exacerbations of throbbing pain, interfering with sleep. Light pressure over the affected pulp increases the pain. Frequently, the corresponding regional lymph node is enlarged and tender. If the pulp is indurated and has lost its normal resilience, pus is present. Untreated, the abscess tends to point towards the centre of the pulp beneath a patch of devitalised skin. A collar stud abscess then occurs; if still untreated, the abscess bursts. Neglected cases suffer serious loss of pulp tissue leading to a markedly scarred finger tip. In the early stages when there is no localisation, large doses of flucloxacillin may bring about resolution. Once pus is present, operation without delay is the rule. A short incision is made through the skin at the point of greatest tenderness. The beginner is warned not to be beguiled by entering only the superficial loculus of a collar stud abscess. Removal of slouch, which is frequently present, is most desirable, but great care must be taken not to traumatise the periosteum. Osteomyelitis of the terminal phalanx may be a sequel of terminal pulp-space infection. That part of the bone without blood supply will become a sequestrum and separate some weeks after the abscess has been opened, in which event the wound continues to discharge. Repealed radiographs and probing (revealing rough bone) will indicate when the sequestrum has separated. Only then must it be removed, after which healing will proceed apace. In the case of a child, regeneration of the diaphysis is possible, provided the periosteum is relatively undamaged. In the adult, no regeneration occurs, and the patient is left with a shortened phalanx covered by an ugly, curved nail. Subcutaneous infections and abscesses can occur on the dorsal and volar surfaces at various levels. The volar surface of the hands of manual workers is often covered with greatly thickened epithelium. Especially in such individuals, a subcutaneous abscess may burst through the dermis and extend in the layers of the epidermis, in which event it is impossible to differentiate it from a purulent blister until the deeper loculus has been discovered at operation. Treatment. The abscess is opened (Fig. 2). The resulting undermined flaps are cut away with scissors. The unroofed cavity is swabbed free from pus, which is examined by culture for the identification Of the bacteria and for tests of their sensitivity to various antibiotics. Then it is explored for a sinus leading to a deep loculus. If one is found, the communicating channel is stretched by inserting and opening the jaws of a small haemostat. Fig. 2. Incisions for drainage of an abscess of the distal closed space. 1. Hockey - slick incision, which can he employed when the abscess is demonstrated definitely to lie in the lateral side of the space; 2. Fish-mouth or horseshoe incision, which gives the most adequate drainage. 3. Through -and- through type of incision for drainage of the distal closed space Pyogenic arthritis of the finger This type of infection occurs from extension of infection from soft tissues around the joint like infection of the middle or proximal segment of the finger or suppurative tenosynovitis (Fig. 3). Only very rarely pyogenic arthritis of the finger may occur from perforating wound of the finger. The infection is first localised in the synovial membrane and in this stage if treatment is done, disability may be avoided. But unfortunately enough the articular cartilages and capsular ligaments are very quickly involved resulting in stiffness of the finger, if not properly treated. Fig. 3. Pyogenic arthritis of the finger: pus Pyogenic arthritis of a finger is suspected, when following a wound, the region of the knuckle becomes very painful and movement of the joint increases the intensity of pain. Crepitus is a late sign. When this condition is not associated with an external wound, one must estimate the blood sugar level to exclude diabetes mellitus. When an external wound is present to show the cause of pyogenic arthritis, immediate exploration should be carried out under antibiotic cover. The extensor expansion on either side is transversely incised and a clear view of the joint should be obtained by mobilising the tendon towards the opposite side. The pus is drained and a search should be made for any loculated collection of pus within the joint as is always done to drain any abscess cavity. Loose fragments of cartilage and necrotic tissues are removed. The joint is irrigated with first normal saline and then with antibiotic solution. The capsule and the extensor expansion are repaired with fine sutures of nylon or polypropylene. The skin wound is closed. It should be left open if the wound is more than 6 hours old and the wound is very much contaminated. The hand is immobilised in optimum position till the infection has completely subsided. When pyogenic arthritis is not associated with an external wound, conservative treatment should always be tried first. An intensive antibiotic therapy should be started immediately and the fingers and the hand are immobilised in the optimum position. In most of the cases, the infection subsides with this treatment. But in some cases operative drainage may be required. Suppurative tenosynovitis Surgical anatomy. The synovial sheaths of all the fingers extend up to the distal interphalangeal joints. Proximally, the sheaths of the index, middle and ring fingers end in a cul-de-sac at the distal palmar crease. The sheath of the thumb is continuous with the radial bursa, which surrounds the tendon of the flexor pollicis longus and extends proximally to a point about I inch above the crease at the wrist (Fig. 4 ). The synovial sheath, covering the flexor tendon of the little finger, sometimes has direct communication with the ulnar bursa or common palmar sheath, which surrounds all the flexor tendons to the four fingers. The ulnar bursa also extends proximally up to 1 inch proximal to the crease at the wrist. At times, the radial and ulnar bursae intercommunicate each other, while they lie in the carpal tunnel, flexor tendons to the four fingers. The ulnar bursa also extends proximally up to 1 inch proximal to the crease at the wrist. At times, the radial and ulnar bursae intercommunicate each other, while they lie in the carpal tunnel. These sheaths are often infected from a puncture wound in one of the digits. There will be swelling of the Finger concerned, but this swelling will be much less than what is found in infection of the middle or the proximal volar space of the finger. The digit will be held in semiflexed position and will be rigid. This rigidity in flexion may disappear due to spontaneous rupture of the sheath. Passive extension will lead to acute pain. Tenderness will be present all throughout the extent of the sheath, but will be maximum over the flexor creases and over the proximal cul-de-sac of the sheath. When the synovial sheaths of the flexor tendons become infected with pyogenic organism and ultimately pus forms within these sheaths, the condition is called suppurative tenosynovitis. Fig. 4. Suppurative tenosynovitis: collection of pus at the tendon sheath Aetiology. This condition occurs: a) directly from a puncture wound e.g. a pin-prick, a needle prick or sharp object penetrating the tendon sheath; b) indirectly, due to spread from neglected subcutaneous infections (middle or terminal or proximal volar space) or injudicious incision for drainage of such abscesses. Pathology. The infecting organism is usually Staphylococcus aureus or Streptococcus pyogenes. As soon as the infection enters the sheath, a reactive effusion occurs which spread for the whole extent of the sheath. Gradually pus forms within the sheath. The sheath gets swollen. Pressure within the sheath along with virulent infection will cause damage to the flexor tendon inside the sheath. Ultimately stiffness of the finger will ensue. Clinical features. This is an infection of the flexor tendon sheath. The infection is mainly a direct one from a prick of a needle, a thorn or a dorsal fin of a fish. The prick is obviously through the skin overlying the tendon sheath, mostly through a digital flexion crease as at this part the skin surface is remarkably nearer to the sheath. Sometimes this condition may develop from injudicious incision for drainage of the distal pulp space or from spread of infection from the middle and proximal volar spaces. The whole sheath is rapidly involved. The patient feels throbbing pain in the affected digit, the finger becomes red and swollen and the patient's temperature rises. Infection of the thumb or little finger spreads up to the palm to involve the radial or ulnar bursa respectively. The cardinal features of this condition are: 1. Uniform swelling of the whole finger except the terminal segment where there is no tendon sheath, 2. Typically the finger is held in flexed position which is classically known as "Hook" sign. This is an early sign. 3. Tenderness over the anatomical disposition of the sheath. To determine the area of tenderness the end of a match stick serves the purpose admirably. Accurate localisation of tenderness is not possible with the examiner's finger tip which covers too wide an area. Usually the tenderness is most marked at the proximal ends of the sheaths in case of the index, middle and ring fingers. In case of ulnar bursa, a point of maximum tenderness is obtained over the part of the bursa lying between the two transverse palmar creases — Kanavel' s sign. 4. The patient is asked to move the fingers. Slight movement of the metacarpophalangeal joint by contraction of the lumbrical and interosseous muscles may be possible but movement of the interphalangeal joints is completely restricted. 5. Any attempt to straighten the finger actively or passively causes exquisite pain. Spesific infection Tetanus It has been estimated that, every year, between 300 000 and 500 000 cases of tetanus occur worldwide with an overall mortality of 40 -15% In the UK, 200 cases occur annually, and the condition is also relatively uncommon elsewhere in Europe, in the USSR and in North America. The burden of this agonising infection falls on those in the other countries of the world, particularly on the children, the neonates, and on the eldery. Education programme to have universal active immunisation can and will lead to a reduction of the number of cases and, significantly, the mortality. Tetanus toxoid (now known as tetanus vaccine) practically eliminated tetanus in the armies during World War II. Today, if active immunity is properly initiated and maintained in an individual, death is unlikely even in the presence of clinical tetanus. Closlridiumi tetanic the causal organism, is a Gram-positive anaerobic rod with terminal spores. Found in manure and soil (notably in market garden areas), it will invade any wound. It multiplies and produces a powerful toxin in any deep, contused wound in the presence of dead tissue, foreign bodies and other bacteria. Penetrating injury from the hoof of an animal can be associated'with this infeclion, while the prick of a rose thorn in a well-manured rose garden can be the sting of death of an elderly assiduous horticulturalist. The exotoxin produced in the inoculation site inhibits the cholinesterase at the motor endplates. resulting in an excess of acetylcholine locally and, therefore, a sustained state of ionic muscle spasm. The exotoxin also travels along the nerves to the central nervous system and causes extreme hyperexcitability of motor neurones in the anterior horn cells, thereby evoking explosive and widespread reflex spasms of muscle in response to sensory stimuli. Once fixed in the nerve tissue, the toxin can no longer be neutralised by antitoxin. Period of onset. The shorter the interval between the first symptom and the first reflex spasm the poorer is the prognosis. If the interval is less than 48 hours, death is likely. It should be remembered that wounds containing tetanus organisms may have healed and been forgotten for months or years before some (unknown) change produces the right conditions for the organism to multiply and produce toxin (latent tetanus). Symptoms and signs. Dysphagia, jaw stiffness and severe pains in the neck, back and abdomen precede the tonic muscle spasms. The sardonic smile (risus sardonicus) if tetanus is evidence of the onset of tonic muscle spasm. Respiration and swallowing become progressively more difficult, and reflex convulsions occur affecting all muscles and causing great pain, opisthotonus (spasm of the extensors of the neck, back and legs to form a backward curvature) and even muscle rupture. The spasms are spontaneous, but can be induced by trivial stimuli such as noise or movement and, when severe, will prevent respiration and produce cyanosis. Between the reflex convulsions, the tonic muscular spasm remains, thus distinguishing tetanus from strychnine poisoning. The temperature is elevated, the pulse is rapid, and respiratory failure and death during a cyanotic attack will usually follow if treatment is not initiated. At an early stage, the symptoms and signs of tetanus might be mistaken with tonsillitis, flu. backstrain, or an acute upper abdominal condition, therefore, careful examination of the patient for a wound is of paramount importance. Treatment. Isolation, quietness and comfort, drainage of pus and wound toilet will be needed, tinman antitetanus globulin (e.g. Humotef) is given i.m. to limit the effects of free toxin and should be used in doses of 250-500 units to give cover throughout the period of establishing active immunity by giving toxoid (tetanus vaccine, adsorbed) i.m. Equine tetanus antiserum has been used but about 20 % of patients develop serum sickness and occasional anaphylactic reactions occur. Antibiotics, including penicillin and metronidazole, are indicated along with measures to protect the lungs. Stage 1. A mild case, where there is tonic rigidity alone, will require initial sedation, relaxation by drugs such as promazine up to 200 mg i.m. and a barbiturate or diazepam (5 -50 mg i.v.). These drugs will be needed approximately 4 times during any 24-hour period. Stage 2. A seriously ill patient, with dysphagia and reflex spasm, will need to have a nasogastric lube passed and sedation continued. The diet, the need for intravenous nutrition, (lie maintenance of balanced protein intake, and of renal function and cardiac function will be priorities. A tracheostomy should be considered if the patient find any difficulty in breathing. The meticulous care of the tracheostomy tube includes suction of mucus. Stage 3. In dangerously ill patients, a major cyanotic convulsion will require curarisation, e.g. up to 40 mg tubocurarine i.v. initially and afterwards i.m. to maintain relaxation. It should be remembered that the curarised patient, though unresponsive, is conscious and sensitive and can hear everything that is being said. Intermittent positive-pressure respiration should be provided, and intensive nursing care with increas-ing sedation would be needed because it has been estimated that a patient at this stage will require at least 350 individual acts of nursing each day. The objective is to reduce the risk of death from spasms or pneumonia wherever possible, while realising that a lethal amount of toxin has already caused severe damage to the motor neurones and the brain with concomitant myocarditis and vascular failure. If recovery takes place, the patient can be weaned from the ventilator (after about 14 days so long as convulsions do not recur when the effects of the relaxants wear off). Results. With the proper attention to nursing care, prophylactic antibiotic therapy, active and passive immunisation against tetanus and, where indicated, tracheostomy, curansalior, and assisted respiration, the death rate can be reduced to approximately 15 %. The results in the very veiling and very old nevertherless are still poor. The tetanospasmin produced by the infection is insufficient to generate immune response so a course of immunisation is recommended on recovery. Gas gangrene Wounds allowing the patient's own faecal flora clostridial spores in the soil, to enter the tissues give rise to anaerobic gas-producing infections. Surgery around the hip joint and leg amputations are at one risk from this postoperative complication, as are wounds of warfare. Clostridium perfringens is usually the cause in about 80 %, other Clostridia, including CI. uede mat ions, CI. histolyticum, CI. septicum, may be causal. The Clostridia produce numerous toxins, including an a-toxin believed to be important in the pathogenesis of gas gangrene. Clostridial invasion of a traumatised muscle of the whole of that muscle from origin to the insertion produces a foul-smelling necrosis of the bun which losecontfactibility and become dull red. or black in appearance. If septicaemia occurs, gas produced in many organs, notably the liver (which necropsy drips with frothy blood - the foaming liver). Subcutaneous tissues alone can be infected; the smelling necrosis, often spreading extensively, begin in the margin of an abdominal or thoracic wound. Clinical features. The wound is under tension between the sutures and the pouting edges exudating brownish and foul-smelling fluid. The skin becomes coloured - a khaki colour - due to associated haemol. Crepitus can usually be detected. (Crepitus, to examining hand, feels like an old hair mattress, radiograph will show the gas in the muscles or in the skin. The patient, although toxic and pale, raised pulse, misleadingly appears mentally clear. Treatment, to be effective, requires immediate actions: 1. Maximum doses of penicillin (up to 2 g 4-hourly) js traditionally the treatment of choice, although there is a better outcome with clindamycin metronidazole: 2. blood transfusion; 3. either exposure of all the affected muscle groups by long incisions or in the subcutaneous infection multiple subcutaneous drainage and slough extraction by incisions into the subcutaneous tissue; 4. hyperbaric oxygen where this is available is said to be helpful in the postoperative period. The use of antigangrene serum: CI. Perfringens 10000UN, CI. Septicum 10000UN, CI. Oedematiens 10000UN. depleted and there has been little interest in resuming production. Tuberculosis Mycobacterium tuberculosis, discovered by Robert Koch in 1882, while he was working in the Imperial Health Office, Berlin, Germany. This acid-fast bacillus is spread bv airborn infection (or from infected cows fn the case of bovine tuberculosis). There are three types of primary infection: a) direct spread to lungs b) from tonsils to the lymph nodes where an abscess may form and track round the sternomastoid muscle, producing a collar abscess; c) from lower ileal infection to the lymph node, the ileocaecal angle. The bacterium, which produces no pigment, grows well at 37°C and may be seen, if there are very many organisms, in the Ziehl-Neelsen stained smear. Growth of the bacteria takes 6 weeks; thus sensitivities to antituberculous drugs will be delayed. Guidelines for treatment. Nutrition and hygienic living conditions are still crucially important in preventing the spread of this infection. Treatment with triple therapy consisting of rifampicin 600 mg, isoniazid 300 mg and pyrazinamide 1500 mg per day given orally for at least 2-3 months is standard chemotherapy at present, followed by months of double therapy by rifampicin plus isonia. Sensitivity testing is usually available at the end of first period of triple therapy and if the source of infection is with an organism that is resistant to these drugs, appropriate changes can then be made. Ethambutol may be of use in resistant cases. In case of pulmonary tuberculosis, the sputum should be examined to assess progress every month until smears are negative, but should the number bacilli increases or the cultures remain positive, development of resistance or noncompliance of patient with treatment should be considered. Genitourinary and orthopaedic tuberculosis is effectively treated by the standard 9-month course. The use of pyrazinamide with rifampicin and isoniazid may be required. All these antituberculous drugs have side-effects which may require repeated careful assement and control; isoniazid causes a peripheral neuritis, ethambutol produces visual impairment, rifampicin is hepatotoxic. Pyrazinamide should be avoided in patients with gout. It should be remembered that it is impossible to eradicate every tubercle bacillus from the body. Dormant and enveloped in fibrous tissue, any remaining bacilli are still able to cause a flare-up of disease, particularly after trauma, after gastrointestinal operations resulting in nutritional deficiency, in old age, immune deficiency or long-term use of steroids. Tuberculous peritonitis Acute tuberculous peritonitis. Tuberculous peritonitis sometimes has an onset that resembles so closely acute peritonitis that the abdomen is opened. Straw-coloured fluid escapes, and tubercles are seen scattered over the peritoneum and greater omentum. Early tubercles are greyish and translucent. They soon undergo caseation, and appear white or yellow, and are then less difficult to distinguish from carcinoma. Tubercles occasionally simulate fat necrosis or the nodules of peritoneal carcinomatosis. On opening the abdomen and finding tuberculous peritonitis, the fluid is evacuated, some being retained for bacteriological study. A portion of the diseased omentum is removed for histological confirmation of the diagnosis, and the wound closed without drainage. At other times, although acute abdominal symptoms arise, the presence of ascites makes the diagnosis ofucule tuberculous peritonitis reasonably evident. Chronic tuberculous peritonitis. Although the incidence of turberculous peritonitis has declined in Britain, in many parts of the world where measures for eradicating tuberculosis (especially the disease in cows) are enforced less strictly, the condition still occurs. Presentation. Abdominal pain is present in 90 %, fever in 60%, loss of weight in 60 %, ascites in 60 %, night sweats in 37%, and abdominal mass in 26%. Origin of the infection. Infection originates from: a) tuberculous mesenteric lymph nodes; b) tuberculosis of the ileocaecal region; c) a tuberculous pyosalpinx; d) blood-home infection from pulmonary tuberculosis, usually the "miliary" but occasionally the "cavitating" form. There are four varieties of tuberculous peritonitis: ascitic, encysted, fibrous and purulent. 5. Study questions: 1. 2. 3. 4. 5. 6. Definition, classification of a panaritium, a phlegmon of hand; A clinical picture of a panaritium, a phlegmon of a hand; Diagnostics and treatment of a panaritium, a phlegmon of a hand. An etiology, a pathogeny acute hematogenous osteomyelitis; Diagnostics and medical tactics of purulent diseases of bones; Kinds of operative treatment;- 7. Chronic forms of osteomyelitis, their treatments; 8. An etiology, a pathogenesis, methods of diagnostics, the basic clinical attributes of a tetanus, antrax, diphtherias of wounds; 9. Methods of specific prophylaxis and treatment of an acute specific surgical infection. 6. The literature: 6.1. Basic : 1. Textbook of basic nursing / Caroline Bunker Rosdahl. – J. B.Lippincott Company. Philadelphia. - 6th ed. –1995.– 1518 p. 2. Fundamentals of nursing /Taylor Mary Carol, Mary Carol, Lillis Carol– J. B.Lippincott Company. Philadelphia. - 1989.– 1356 p. 6.2. Аdditional: 1. Gostishev V.K. "Guidance to practical employments on general surgery". M., "Medicine" - 1987. 2. P. of Brown. Operating block. Operating brigade. – Kharkov, 1997. – with. 1-32. Methodical instruction was prepared by Assistant A review is positive, associate professor Riabyi S.I. Chomko O.J. Materials of control of base level of preparation of students: tests. Multiple Choices. Choose the correct answer/statement: 1. Patient A., 22 years old, has addressed for medical aid with complaints to a pain of constant character in a site of the right palm which amplifies at movements by fingers, the general delicacy, subfebrile temperature. Objectively: at the basis of the third finger of the right hand on a palmar surface it is marked callosity skins around of which the edema and hyperemia of skin are observed. Through epidermis the purulent exudation is visible. A palpation of a place of defeat morbid, violation of function of fingers and brushes. It is possible to think of what pathology? A. A hypodermic panaritium of the basic phalanx IIIrd finger of the right hand. B. A dermal panaritium of the basic phalanx IIIrd finger of the right hand. C. A phlegmon of median checkered space of the right hand. D. Subcallosal abscess. E. 2. Articular panaritium of the IIIrd finger of the right palm. Patient G., 28 years old, has addressed for medical aid with complaints to a pain of constant character in a region of IInd finger of the left hand, infringement of function of a finger. Objectively: on a dorsum of the basic phalanx of the IInd a finger of the left brush the inflammatory infiltrate 1,5×2 сm with a necrotic hinge in center is determined . What disease takes place in the patient? A. A skin panaritium. B. A subskin panaritium. C. A carbuncle. D. A furuncle. E. 3. Erizipelid. Patient A., 26 years old has received a microtrauma (puncture) of a nail phalanx of the IInd finger of the left hand. 5 days later has addressed in a polyclinic where the diagnosis was exposed: a hypodermic panaritium of nail phalanx of the IInd finger of the left hand. Under what anesthesia it is expedient to execute disclosing of a panaritium? A. Local infiltrative anaesthesia. B. An intravenous narcosis. C. Intraosseous anaesthesia. D. A conduction anaesthesia by Oberst-Lukachevitch. E. 4. Intubation narcosis. Patient M., 60 years old, admit in surgical department 10 days later from the beginning of disease with complaints to pains in a region of the IInd finger of the left hand, infringement of function of a finger, the general delicacy, a fervescence up to 38°С. Objectively: a condition of the patient satisfactory, pulse 90 per 1 minutes, arterial pressure - 120/80 mm Hg., a body temperature 38°С, IInd finger of the left hand dwarfed, deformed, a skin hydropic, cyanotic. In the field of an average phalanx on a palmar surface - is a fistula up to 0,3 sm with purulent discharges. Flexion contracture of finger. Active movements are absent. On a roentgenogram a destruction of a bone of middlephalanx is determined. What disease at the patient? A. A bone panaritium. B. A pandactylitis. C. Tendovaginitis. D. A subskin panaritium as "cuff link". E. A thecal whitlow. Real-life situations to be solved: 5. Patient E., 35 years old, was treated during 3 days concerning a thecal whitlow of the fifth finger of the left hand. On given time of the complaint for a pain in a hand, infringements of a flexion of the Ist and Vth fingers. Objectively: expressed edema and morbidity in the field of the Ist and Vth fingers, rise in temperature up to 38°C. What complication was developed in the patient? 6. Patient K., 18 years old, has addressed in surgical department with complaints to a throbbing pain in the field of the thumb of the right hand. From an anamnesis it is known, that 2 days later has received insignificant wound in time of nails paring. Objectively: nails platen is swollen in lateral side, hyperemia is observed. From under it is allocated insignificant quantity of white pus. Diagnose. Your tactics. Answers to the Self-Assessment: D; D; D; B; U-like phlegmon of the left hand. Diagnosis: paronychia of the thumb of the right hand. Tactics: to raise with the help of a scalpel the nail platen for pus discharge.