Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
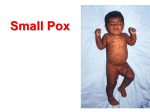
SMALLPOX Melissa Mattison, M.D. October 22, 2002 SMALLPOX A highly infectious disease Period of oral lesions and rash most infectious Spread via droplet nuclei, aerosols and direct contact Even bed-sheets of patients with the disease can transmit it HISTORY Responsible for many deaths over the course of history and used to account for 10% of deaths worldwide The disease decimated the Native American population Germ warfare was used by Lord Jeffery from England during the French and Indian War in the 1700’s, by dispensing blankets of victims of smallpox to the unsuspecting Native American population 1796 – Edward Jenner noticed that dairymaids infected with cowpox gained immunity to smallpox and the the first vaccination program began 1967 – WHO began a program to globally eradicate smallpox 1972 – USA stopped vaccinating against smallpox 1977 – The last case of documented smallpox was seen in Somalia 1980 – All countries supposedly destroyed their stocks of smallpox with virus remaining in only the USSR, Great Britain and the CDC in Atlanta EPIDEMIOLOGY Incidence is highest in Spring and Winter Variola Major -the classic description of smallpox -30% mortality rate -4 major varieties – Ordinary (most common), Modified (in previously immunized patients), Hemorrhagic (uniformly fatal), Malignant (usually fatal) Variola Minor (alastrim) -1% mortality rate MICROBIOLOGY A DNA virus Part of the genus orthopoxvirus. Other viruses in this genus include: monkeypox, vaccinia and cowpox Highly infectious with only a few virons required PATHOGENESIS/CLINICAL PRESENTATION Inoculation (12-14 days) -via inhalation, spreads to regional lymph nodes where replication occurs. Asymptomatic viremia develops on day 4, followed by multiplication of the virus in the spleen, bone marrow, and lymphatic system. By day 8, a second viremia develops along with fever and toxemia. -the virus then localizes in small blood vessels in the dermis and beneath the oral and pharyngeal mucosa Prodrome/Initial Symptoms (2-4 days) -fever and malaise -too sick to carry on normal activities Days 1-4, The Rash -first seen on tongue and in o/p. When these sores break, the virus is released in massive quantities in the saliva and the patient is most contagious. -Within 24 hours, the rash develops on the skin, first starting on the face and then the arms, legs and later hands and feet. -On day 3, the rash becomes raised bumps and by day 4 they are filled with opaque fluid with a depression in the center. Days 5-10 -Rash becomes pustular and firm to touch Days 11-14 -Most of the pustules will scab over Days 15-21 -Scabs fall off, leaving pitted scars, most pronounced on the face -The person is contagious until all the scabs have fallen off Beth Israel Deaconess Medical Center Residents’ Report PRE-EXPOSURE PROPHYLAXIS Vaccination – once and then in theory, every 10 years. Use a specialized bifurcated needle, a small but exact amount of inoculum. 15 repeated punctures into the deltoid or thigh at right angle to the skin. Vaccination + VIG (Vaccinia immune globulin) – to minimize vaccination side effects, only when absolutely necessary. VIG is in very short supply and some say right now the rate limiting effect to widespread vaccination in the USA. The Vaccine- made of live vaccinia, another “pox” type virus. Vaccination site must be cared for meticulously to prevent infection from spreading to others. The vaccine cannot give you smallpox, but it can make you sick, especially if you have skin conditions or are immunocompromised. 1-2 deaths/million vaccinated are expected and usually arise from post-vaccination encephalitis or vaccinia gangrenosa (when the localized inflammation at the site of vaccination spreads through the body, causing widespread dermal necrosis with involvement of the bone and adjacent tissues). 15/million vaccinated with have life-threatening complications and 100s/million will have skin infections and rashes from the vaccine (non-life-threatening complications). Do not vaccinate people who have HIV, are immunocompromised due to cancer or immunosuppressant medications (i.e., post-transplant), pregnant women, or people with children < 1 yo at home. POST-EXPOSURE PROPHYLAXIS -Vaccinate ASAP (up to 4 days after exposure can help) -No antiviral agents are currently available -Isolate the people suspected of having the disease Do not admit to the hospital Or – dedicated one hospital per region to victims Vaccinate anyone who works in the hospital (or morgue) or anyone with face-to-face contact with victim If victims die, cremation is preferred DIAGNOSIS -Notify public health authorities immediately after any suspicion develops -Characteristic Rash Most dense in face and extremities All lesions are at the same stage of development (in each region of the body) -Obtain pustular/vesicular fluid collected by person already vaccinate put on cotton swab, into vacutainer tube, sealed with adhesive tape at juncture of stopper and the tube and place in a second, durable, watertight container. -Send to a BL-4 facility (capable of handling highly contagious fluid) -Electron microscopy of the fluid will show brick-shaped virons -PCR of the fluid will be positive for smallpox References: JAMA 281, 22: 2127-2137 JAMA 287, 9:1104 Mandell, Principles and Practice of Infectious Disease www.cdc.gov Of other potential interest: Live satellite broadcast 11/6 12:45-3 pm, Smallpox: Recognition and Response, Sherman Auditorium Beth Israel Deaconess Medical Center Residents’ Report