Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Appendix C
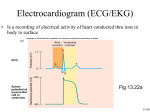
Electrocardiogram
EKG or ECG
Electrical Stimulation of the Heart:
The electrical stimulus that is required before every heart beat causes
sodium , potassium, and other ions to move in or out of every cell in
the heart. This exchange of ions produces an electrical current that has
three distinct phases:
Electrical Phases in the Heart
Polarization - ("ready phase") state of cellular rest when all ions are in
their correct places and ready for stimulus
Depolarization - state of cellular stimulation which precedes
contraction
Repolarization - ("recovery phase") state of cellular recovery which
follows each contraction
P wave
The P wave represents the depolarization of the atria (atrial
depolarization)
The P wave contour is usually smooth
entirely positive (Leads I, II, III, aVF, and V4 to V6)
negative (aVR) (monophasic) in all leads except V1
The P wave duration is normally less than 0.12 sec.
The P wave amplitude is normally less than 0.25 mV in all leads
The P wave normally appears entirely upright
PR Interval
The PR interval measures the time required for the impulse to travel
from the atria myocardium adjacent to the SA node to the ventricular
myocardium adjacent to the fibers of the Purkinke network (atrial
and ventricular depolarization)
The PR interval is measured from the beginning of the P wave to the
beginning of the QRS complex.
Normal PR interval duration range is from 0.12 sec - 0.20 sec
QRS Complex
represents depolarization of the ventricles (ventricular
depolarization)
If the first deflection from the isoelectric line is negative it is a Q
wave (not always present)
The first positive deflection from the isoelectric line is an R wave
The negative deflection following an R wave is an S wave
Normal QRS interval range is from 0.04 sec - 0.12 sec
Measured from the first deflection from the isoelectric line to the Jpoint
(J-point is where the QRS complex ends and the ST segment begins)
ST Segment
represents the plateau (phase 2) of the action potential (ventricles in
active state following depolarization, but NO electrical activity occurs
at this time.
Is normally isoelectric - no difference exists in electrical potential
among the action potentials of the heart
No current flow occurs because all cells are at zero potential
T wave
represents phase 3 of the action potential, when the ventricles are
being rapidly repolarized (ventricular repolarization)
Is normally rounded, slightly asymmetric, and the same polarity as the
QRS complex
The effective refractory period is present during the beginning of the
T wave.
QT interval
represents the entire duration of ventricular depolarization and
repolarization (ventricular refractory period is the time necessary
for the ventricle to depolarize, then repolarize)
The normal QT varies with age, gender, and heart rate
Cardiac Rhythms
SA node
Normal Sinus or Regular Sinus Rhythm (NSR or RSR)
P wave present and regular.
Atrial rate (P waves) between 60 and 100 beats/min
Each P wave is followed by a QRS complex
Sinus Bradycardia
P wave present and regular
Atrial rate (P waves) < 60 beats/min
Each P wave is followed by a QRS complex
RX:
May require no treatment
Atropine IV
May require temporary pacemaker or permanent pacemaker
Sinus Tachycardia
P wave present and regular
Atrial rate (P waves) > 100 beats/min
Each P wave is followed by a QRS complex
RX:
treat underlying cause
Sinus Arrhythmia
P wave present
P-P interval - phasic shortening then lengthening of P-P interval,
usually with respirations
Impulse initation by SA node
RX:
usually none
Common Arrhythmias Originating from Atria:
Premature Atrial Contractions (PAC)
initiated by ectopic focus in the atria
premature P wave with a contour different from a sinus P wave
(location of ectopic focus determines its shape)
QRS may or may not be normal
PAC is followed by a pause ~ equal to the sinus cycle
(measured R to R)
Premature Atrial Contractions (PAC)
associated with use of caffeine, stress, or use of tobacco
may be a precursor to developing uncontrolled AF
RX:
may require no treatment
sedation
quinidine
Atrial Flutter
rapid sawtooth P waves
ventricular rate regular
associated with CAD, pulmonary embolism, mitral valve disease, and
thoracic surgical procedures.
atria depolarize at a rate of 250 to 350 beats/min
Atrial Fibrillation
rapid irregular P waves > 350/min
ventricular rate irregularly irregular
ventricular rate varies, may increase to greater than 150 if untreated
if rate > 100 beats/min referred to as uncontrolled AF
if rate < 100 beats/min referred to as controlled AF
Sick Sinus Syndrome (SSS)
term to describe several disorders of the SA node
tachycardia-bradycardia syndrome is the most common type of SSS
complication associated with SSS is CHF and CVA resulting from
thromboembolisms
RX:
stabilization of heart with perm pacemaker
Atrial Tachycardia
rate 150 to 250 beats/min
P wave present but may be hidden
QRS is generally normal
ventricular rate is regular
RX:
usually none
prolonged episodes may require carotid sinus pressure, vagal
stimulation, verapmil, digitalis, or beta blocks
Impulse Conduction Deficits
A-V Blocks
First Degree AV Block
PR interval prolonged - > 0.20 sec
May warn of impaired conduction
Second Degree AV Block
Mobitz I (Wenckebach)
PR interval progressively lengthens until a P wave is not followed by
a QRS complex
Ratio of P waves to QRS complexes varies, i.e. can be 5:1, 4:1, 3:1, or
2:1
more often is a transient event
seen with patients post Inferior MI, Digitalis toxicity, or postoperative
Mobitz II
more serious that Mobitz I
less common than Mobitz I
characterized by nonconducted sinus impulses despite constant PR
intervals
usually the QRS are widened because of a BBB, the dropped beat
represents a form of intermittent blockage of both bundle branches
the defect is found in either the bundle branches of the bundle of HIS
occur more frequently with patients with acute anterior septal wall
MIs
often progress to CHB
Third Degree AV Block (Complete Heart Block)
atria and ventricles beat independently
P waves have no relation to QRS
ventricular rate may be as low as 20-40 beats/min
Bundle Branch Block (BBB)
same as normal sinus except QRS complex is > 0.12 sec
depending on site of defect is labeled RBBB or LBBB - the LBBB has
two main devision the anterior and posterior fascicles
seen with severe CAD, acute anterior wall MI, hypertensive pts
Ventricular Arrhythmias
Premature Ventricular Contractions
arise from an ectopic focus in the ventricles
wide bizarre QRS greater than 0.12 sec
no associated P wave
T wave is in the opposite direction from the main QRS deflection
~ 50% of PVCS are followed by a compensatory pause (the interval
from the beat preceding to the beat following the PVC is equal to two
sinus cycles)
Premature Ventricular Contractions
the remaining 50% PVCs result in retrograde conduction to the atria
causing the next sinus P wave to be early and a compensatory pause
occurs
associated with CHF, digitalis toxicity, electrolyte imbalances, and
excessive caffeine intake
Ventricular Tachycardia
no P wave before QRS
QRS wide and bizarre
ventricular rate > 100 beats/min (usually 140-240)
Ventricular Fibrillation
chaotic electrical activity
no recognizable QRS complex
associated with MI, drug toxicity, electrocution, freshwater drowning
no CO
absent pulse or respirations -- CARDIAC ARREST