Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
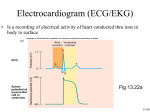
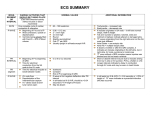
Electrocardiography 1. Describe the P, QRS, ST, T, and U waves in a general way and the measurement of the heart rate, the PR interval, the QRS width, the QT interval, and their normal values in detail. P wave The P wave, which represents atrial depolarization, is a small deflection before the QRS complex. The normal values for P wave amplitude and width are described in PR Interval The PR interval is measured from the beginning of the P wave to the beginning of the QRS complex. The PR interval may vary slightly in different leads, and the shortest PR interval should be noted. The PR interval represents the time it takes for the stimulus to spread through the atria and to pass through the AV junction. (This physiologic delay allows the ventricles to fill fully with blood before ventricular depolarization occurs.) in adults the normal PR interval is between 0.12 and 0.2 second (three to five small boxes). When conduction through the AV junction is impaired, the PR interval may become prolonged. Prolongation of the PR interval above 0.2 second is called first-degree heart block. QRS Nomenclature One of the most confusing aspects of electrocardiography for the beginning student is the nomenclature of the QRS complex. The QRS complex, as noted previously, represents the spread of a stimulus through the ventricles. However, not every QRS complex contains a Q wave, an R wave, and an S wave; hence the confusion. This bothersome but unavoidable nomenclature becomes understandable if you remember the following: if the initial deflection of the QRS complex is negative (below the baseline), it is called a Q wave. The first positive deflection in the QS complex is called an R wave. A negative deflection following the R wave is called an S wave. Thus this QRS complex contains a Q wave, an R wave, and an S wave. If the entire QRS complex is positive, it is simply called an R wave. However, if the entire complex is negative, it is termed a QS wave (not just a Q wave as you might expect). Occasionally the QRS complex will contain more than two or three deflections, and in such cases the extra waves are called R’ (R prime) waves if they are negative. Shows the various possible QRS complexes and the nomenclature of the respective waves. Note that the capital letters (QRS) are used to designate waves of relatively large amplitude while small letters (qrs) are used to label relatively small waves. This nomenclature is confusing at first, but it allows you to describe any QRS complex over the phone and to evoke in the mind of the trained listener an exact mental picture of the complex named. For example, in describing an ECG you might say that lead V1 showed an rS complex (“small r, capital S”) while lead aVF showed a QS wave. QRS Width (Interval) 1 The QRS width represents the time required for a stimulus to spread through the ventricles (ventricular depolarization) and is normally 0.1 second or less. If the spread of stimulus through the ventricles is slowed, for example, by a block in one of the bundle branches, the QRS width will be prolonged. ST Segment The ST segment is the portion of the ECG cycle from the end of the QRS complex to the beginning of the T wave. It represents the beginning of ventricular repolarization. The normal ST segment is usually isoelectric (that is, flat on the baseline, neither positive nor negative), but it may be slightly elevated or depressed normally (usually by less than 1 mm). Some pathologic conditions, such as myocardial infarction, produce characteristic abnormal deviations of the ST segment. The very beginning of the ST segment (actually the junction between the end of the QRS complex and the beginning of the ST segment) is sometimes called the J point. T Wave The T wave represents part of ventricular repolarization. A normal T wave has an asymmetric shape; that is, its peak is closer to the end of the wave than to the beginning. When the T wave is positive, it normally rises slowly and then abruptly returns to the baseline. When the T wave is negative, it descends slowly and abruptly rises to the baseline. The asymmetry of the normal T wave contrasts with the symmetry of T waves in certain abnormal conditions, such as myocardial infarction , and high serum potassium (hyperkalemia). QT Interval The QT interval is measured from the beginning of the QRS complex to the end of the T wave. The QT interval primarily represents the return of the stimulated ventricles to their resting state (ventricular repolarization). The normal values for the QT interval depend on the heart rate. As the heart rate increases (RR interval shortens), the QT interval normally shortens; as the heart rate decreases (RR interval lengthens), the QT interval lengthens. You should measure several QT intervals and use the average value. The QT interval is often difficult to measure when it is long because the end of the T wave may merge imperceptibly with the U wave. As a result you may be measuring the QU interval rather than the QT interval. Because of this problem, another index of the QT has been devised. It is the rate-corrected QT is obtained by dividing the QT that you actually measure by the square root of the RR interval: QR / RR . Normally the QTc is less than 0.44 sec. There are a number of factors that can abnormally prolong the QT interval. For example, certain drugs, such as quinidine and procainamide (Pronestyl, procan SR), and electrolyte disturbances, such as a low serum potassium (hypocalcemia), can prolong the QT interval. The QT interval may also be prolonged with myocardial ischemia and infarction and with subarachnoid hemorrhage. QT prolongation may predispose patients to potentially lethal ventricular arrhythmias. The QT interval may also be shortened, for example, by digitalis in therapeutic doses or by hypercalcemia (high serum calcium concentration). The lower limits of normal for the QT interval have not been well defined. 2 U wave The U wave is a small rounded deflection sometimes seen after the T wave. As noted previously, the exact significance of the U wave is not known. Functionally U waves represent the last phase of ventricular repolarization. Prominent U waves are characteristic of hypokalemia (low serum potassium). Very prominent U waves may also be seen in other settings, for example, in patients taking drugs such as quinidine or one of the phenothiazine, or sometimes after cerebrovascular accidents. The appearance of very prominent U waves in such settings, with or without actual QT prolongation, may also predispose patients to ventricular arrhythmias. Normally the direction of the U wave is the same as the direction of the T wave. Negative U waves sometimes appear with positive T waves. This is abnormal and has been noted in left ventricular hypertrophy and myocardial ischemia. 2. What are the two simple methods for measuring the heart rate (number of heartbeats per minute) from the ECG? There are two simple methods for measuring the heart rate (number of heartbeats per minute) from the ECG. 1. The easier way, when the heart rate is regular, is to count the number of large (0.2 sec) boxes between two successive QRS complexes and divide the constant (300) by this. (the number of large time boxes is divided into 300, because 300 x 0.2 = 60 and we are calculating the heart rate in beats per minute or 60 seconds.) For example, the heart rate is 100 beats/min, since there are three large time boxes between two successive R waves (300 ÷ 3 =100). Similarly, if there are two large time boxes between two successive R waves, the heart rate is 150 beats/min. if there are five intervening large time boxes, the heart rate is 60 beats/min. 2. If the heart rate is irregular, the first method will not be accurate since the intervals between QRS complexes will vary from beat to beat. In such cases an average rate can be determined simply by counting the number of cardiac cycles every 6 seconds and multiplying this number by 10. (A cardiac cycles is the interval between two successive R waves.) Counting the number of cardiac cycles every 6 seconds can be easily done because the top of the ECG paper is generally scored with vertical marks every 3 seconds. By definition, a heart rate exceeding 100 beats/min is termed “tachycardia” (tachys, Greek, swift) while one slower than 60 beats/min is called “bradycardia” (bradys, slow). Thus, during exercise you probably develop a sinus tachycardia but during sleep or relaxation your pulse rate may drop into the 50s, or even lower, indication a sinus bradycardia. 3. Try to make the diagnoses of following EFG? 3 right atrial enlargement sinus bradycardia 4 right ventricular hypertrophy evolving anterior wall infarction 5 right bundle branch block (RBBB); 6 acute anterior wall infarction 7 premature atrial contractions (PACS) Multiple infarcts (anterior and inferior wall) 8 Left ventricular hypertrophy Second-degree AV block Mobitz type 1 9 sinus tachycardia 10 Acute inferior wall infarction premature ventricular contractions (PVCs) 11 atrial flutter WPW(type A ) pattern 12 left atrial enlargemen ventricular flutter 13 Ventricular fibrillation Second-degree AV block Mobitz type 2 14 atrial fibrillation left bundle branch block (LBBB); 15 WPW(type B ) pattern Hyperkalemia 16 17