Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
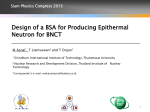
Boron Neutron Capture Therapy for Cancer Treatments by: Junjie Huang A dissertation submitted to the Department of Physics, University of Surrey, in partial fulfillment of the degree of Master of Radiation and Environmental Protection Department of Physics Faculty of Electronics & Physical Sciences University of surrey July 2009 © Junjie Huang 2009 1 Table of Contents Glossary of Terms…………………………………………..P3-5 Abstract...……………………………..…...…………………..P6 1. Introduction………………………….………………..…P7-9 2. Three Major Factors of BNCT…………….……...…..P10-14 2.1 Boron 10-Delivery Agent……..…….….....………..…P10-12 2.2 Neutron Sources……………………..………………...P12-14 2.3 Dose Calculating and Treatment Planning by using Monte Carlo....………..……..…..…………………………....P14 3. Clinical Studies for Cancer Treatments by BNCT…….P15-21 3.1 BNCT Trials for Brain Tumors…………………..…...P15-19 3.2 BNCT Trials for Other Tumors….……..……….…….P19-21 4. Recent Development of BNCT….…………..………...P22-23 5. Conclusion…...……………………………………..…P24-25 Bibliography………………………………………….… P26-27 References………...……………………………………...P28-37 2 Glossary of Terms BBB: blood-brain barrier-is a separation of circulating blood and cerebrospinal fluid (CSF) maintained by the choroid plexus in the central nervous system (CNS) (Wikipedia 1, 2009). BGRR: Brookhaven Graphite Research Reactor in BNL, USA BMRR: The Brookhaven Medical Research Reactor, USA BNCT: boron neutron capture therapy BNL: Brookhaven National Laboratory, USA BPA: 4-dihydroxy-borylphenylalanine-is considered to be the representative of the first generation boron 10-delivery agent for BNCT BSH: sulfahydryl borane-is considered to be the representative of the second generation boron 10-delivery agent for BNCT CT: computed tomography-a medical imaging method employing tomography created by computer processing; digital geometry processing is used to generate a three-dimensional image of the inside of an object from a large series of two-dimensional X-ray images taken around a single axis of rotation (Wikipedia 2, 2009). EORTCR: European Organisation for Research and Treatment of Cancer Reactor FR: folate receptor 3 GBM: glioblasoma multiforme-a type of malignant brain tumors HFR: High Flux Reactor in Petten, Holland HTR: Hitachi Training Reactor in Japan IMRT: intensity modulated radiation therapy JAEA: Japan Atomic Energy Agency JRR: Japan Atomic Energy Research Institute Reactor KERMA: kinetic energy released in matter-is the sum of the initial kinetic energies of all the charged particles liberated by uncharged ionizing radiation (i.e., indirectly ionizing radiation such as photons and neutrons) in a sample of matter, divided by the mass of the sample (Wikipedia 3, 2009). KUR: Kyoto University Reactor in Japan KURRI: Kyoto University Research Reactor Institute in Japan LET: linear energy transfer-is a measure of the energy transferred to material as an ionizing particle travels through it. Typically, this measure is used to quantify the effects of ionizing radiation on biological specimens or electronic devices (Wikipedia 4, 2009). MIT: Massachusetts Institute of Technology, USA MITR: Massachusetts Institute of Technology Reactor in MIT, USA 4 MRI: magnetic resonance imaging-is primarily a medical imaging technique most commonly used in radiology to visualize the internal structure and function of the body (Wikipedia 5, 2009). MuITR: Musashi Institute of Technology Reactor in Japan NRI: Nuclear Research Institute in Rez, Czech Republic 5 Abstract Boron neutron capture therapy (BNCT) is an ideal technique to kill cancer cells selectively without harming healthy cells nearby, which is based on the reaction of boron-10 nuclei capturing neutrons to yield high-LET alpha particles, recoiling lithium-7 nuclei and gamma rays (Barth et al, 2006). BNCT was initially proposed to treat the patients with GBMs. Although BNCT is reported to be at least equivalent or more effective to treat GBM, when compare it with the other standard therapies. To date, it has not revealed significant superiority to replace the others yet. However, BNCT has started to shown its ability to treat other types of primary or recurrent cancers such as melanomas, head and neck cancers, liver cancers and thyroid cancers since the mid 1980s. 6 1. Introduction The most well-known radiation types applied to radiotherapy are gamma ray (γ) and X-ray. They kill not only cancer cells but also normal cells. As appearance of gamma knife, conformal radiation therapy and intensity modulated radiation therapy (IMRT) (NCI, 2009), radiation dose can be increased to a higher level to the patients at the same time as minimizing healthy tissue destruction, such as the treatment for nasopharyngeal carcinoma (nose & throat cancer) and mastocarcinoma (breast cancer). However, at present, many cancers such as malignant brain tumors can not be treated effectively by conventional therapy (surgery, chemotherapy and radiotherapy). Boron neutron capture therapy (BNCT) has been born to aim at these tricky cancers. Chadwick who was from the Cavendish Lab of the University of Cambridge, United Kingdom discovered the neutron in 1932. Three years later, in 1935, Taylor, Burcham and Chadwick showed that boron-10 (10B) has the ability to capture slow neutron to release lithium-7, alpha particles and gamma rays. That is called the boron-10 neutron-capture reaction. A year after, in 1936, the first person who proposed that this reaction can be utilised to treat cancer was Locher. (Sweet, 1997) Boron neutron capture therapy (BNCT) is an ideal treatment to kill cancer cells selectively without harming healthy cells nearby. It is a targeted chemo-radiotherapy which utilises boron-10 that is attached to a suitable tumor-seeking drug (Stable isotope - boron 10 is used because of its high neutron capture cross-section (approx 4000 barns) which means that it is capable to capture slow neutron easily.) (Walker, 1998). First of all, a boron 10-carrying drug is injected into the blood. Then, a tumor accumulates the drug through the blood transportation system. Thereafter, the tumor is irradiated by a thermal neutron (E ≈ 0.025eV)) or an epithermal neutron (1eV < E < 10keV) source (At present, neutron beams are extracted from the uranium-235 fission reaction within a nuclear reactor (Walker, 1998). Finally, the boron-10 atoms inside the tumor capture the neutrons to produce highly energetic helium 4 (4He) nuclei (i.e., alpha (α) particles) 7 and recoiling Lithium 7 (7Li) ions to kill the tumor cells (Figure 1 illustrates the sequence of nuclear events.) (MIT, 2008). Figure 2 shows the formula for the reaction. Figure 1: Schematic of Boron-10 Neutron Interaction (MIT, 2008) Figure 2: Boron neutron capture reaction formula (Walker, 1998) The range of the two particles - 4He and 7Li within a tumor cell are ~9μm and ~5μm 8 (approx the diameter of a tumor cell) respectively. They each have high linear energy transfer (LET) values as well. Thus, all high energy is released in a tumor cell. As a result, the reactions bring the tumor cells high lethal probability, while normal cells outside the tumor survive. Figure 3 shows the schematic concept of BNCT. (MIT, 2008) Figure 3: Schematic Depicting Concept of BNCT (MIT, 2008) BNCT has been experimentally tested to treat malignant brain tumors called glioblasoma multiforme (GBM) and other tumors. There are a number of reports of successful trial examples, but these have not shown to be outstanding to other conventional therapies yet. Thus, BNCT is still at trial stage. (Wikipedia, 2008) 9 2. Three Major Factors of BNCT 2.1 Boron 10-Delivery Agents The primary factor for successful BNCT relies on the boron 10-delivery agents. These are the types of tumor cell-finding boron 10-containing agent which are injected into the human body, which then accumulates in the tumor through blood transportation system within a period of time. There are seven aspects should be considered for a useful boron 10-delivery agent: (1) the most important aspect is strong selectively accumulative ability to achieve high ratios of (concentration of boron-10 in tumor cells)/(concentration of boron-10 in normal cells) (the ratios should be greater than 3-4); (2) low or even none systemic toxicity; (3) to achieve at least ~20μg 10 B/g of tumor boron-10; (4) rapid clearance from blood and normal tissues and persistence in tumor during BNCT; (5) chemical stability; (6) water solubility; (7) lipophilicity (Yamamoto et al., 2008; Barth et al., 2005). Failed to achieve high ratios will result in unnecessary damage to the surrounding normal tissues. For example, use BNCT to treat a patient with a brain tumor. The scalp is rich in capillaries. If the ratio is too low, this means that the boron-10 concentration of the blood in the vessels is relatively high. While irradiating the tumor with a dose of thermal neutron or epithermal neutron beam, the scalp is receiving substantially unnecessary damage. As a result, the neutrons have been wasted in damaging normal cells, and then less damage is made to the tumor. Finally, the treatment is failed. However, there is no universal agent. Various agents should be developed to aim different kinds of malignancies. At the beginning of BNCT usage, sodium borate and boric acid and its derivatives were utilized in the 1950s, but boron concentrations in the tumor were not satisfactory (Farr et al., 1954). Then, BPA (4-dihydroxy-borylphenylalanine) was made (Snyder et al., 1958). The compound was shown to give much higher ratios of (concentration of 10 boron-10 in tumor cells)/(concentration of boron-10 in normal cells) than the other compounds. In 1980s, it was reported to have a greater potential to treat melanomas (Ichihashi et al., 1982). Later on, it was indicated to be applied in BNCT for treatments of malignant brain tumors (Coderre et al., 1990). BPA can be considered to be the representative of the first generation of boron 10-compound as a type of boron 10-delivery agent for BNCT. Polyhedral boranes [B10H10]-2 and [Bl2H12]-2 were discovered with cage structures which have very impressive properties of hydrolytic and chemical stabilities (Hawthorne & Pitochelli, 1959). Later on, sodium decahydrodecaborate Na2Bl0H10 was indicated to be a promising boron 10-delivery agent (Soloway et al., 1961). It was observed to show high ratios of (concentration of boron-10 in brain tumor cells)/(concentration of boron-10 in normal cells). Unluckily, the drug was slightly toxic to the human body. Finally, BSH (sulfahydryl borane, Na2B12H11SH) with lower toxicity was developed (Soloway et al., 1967). Afterward, BSH had been applied to most of the clinical trials in the USA, Europe and Japan, and then adequate results were obtained. Therefore, BSH can be considered to be the representative of the second generation of boron 10-compound as a type of boron 10-delivery agent for BNCT. The development of the third generation of the boron 10-delivery agents is the most crucial factor to directly affect the destiny of BNCT. The third generation of delivery agents has been developing due to unsatisfactory clinical results by using BPA or BSH for BNCT. There is a major difference between the third generation agents and the previous two. The third generation agents adopt third party agents to deliver boron-10 compounds. They mainly consist of a stable boron group or cluster attached via a hydrolytically stable linkage to a tumor targeting moiety (Barth et al., 2005). There are a few strategies for targeting the third generation agents to the tumor cells, such as conjugating to recognition factors, entrapping in vesicles or incorporation in vital compounds (Azab et al., 2006). So far, there are a number of third generation agents 11 have been investigated, such as monoclonal antibodies (Olsson et al., 1998), biochemical precursors (Tjarks, 2001), polyamines (El-Zaria et al., 2002), DNA-binding agents (Tietze et al., 2002), peptides (Ivanov et al., 2002), antisense agents (Olejiniczak et al., 2002), polyhedral borane (Surewein et al., 2002), porphyrins (Isaac & Kahl, 2003), carbohydrates (Tietze et al., 2003), amino acids (Kabalka & Yao, 2003) and liposomes (Carlsson et al., 2003; Justus et al., 2007). Organelles in the tumor cells such as golgi bodies, endoplasmic reticulums, lysosomes, mitochondrion and nuclei are suitable for targeting; thereinto, nuclei are particularly good for targeting, because less boron-10 nuclei will be needed to kill a tumor cell if the boron-10 nuclei are located at/near the tumor cell centers (Cell nuclei are usually at/near the centers of the cells.) (Gabel et al., 1987). A useful boron 10-delivery agent must be soluble in water, which is to be systemically administered; also, lipophilicity enables it to cross the blood-brain barrier (BBB) and diffuse into the tumor (Barth et al., 2005). 2.2 Neutron Sources The neutron beam source is another key to the success of BNCT. BNCT neutron sources have been exclusive to nuclear reactors since the BNCT idea was proposed. This is another reason why BNCT has not entered routine clinical application yet. As BNCT technique is on the way to be mature, an attempt has been made to build an advanced accelerator-based BNCT centre in a hospital to have a more flexible neutron source than a research reactor (Matsumoto, 2007). Besides the accelerators, compact medical research reactors are the other option, such as the operating one in Beijing, China. Thermal neutrons with energies of approximately 0.025eV are used in BNCT. They are well below the threshold of ionizing tissue components (Zamenhof et al., 1994). However, thermal neutron beam can not penetrate into deep tumors due to only 2.5cm 12 penetration range of them within the tissue’s surface (Sweet et al., 1960). Thus, thermal neutrons are suitable for superficial tumor treatments, such as BNCT treatment for melanoma which is a type of skin cancer (Mishima & Ichihashi et al., 1989; Mishima & Honda et al., 1989). However, substantial amount Japanese patients of malignant brain tumor have been treated with surgery of opening crania, followed by BNCT (Nakagawa & Hatanaka, 1997). In order to effectively treat the tumors deep inside the brain without opening crania, epithermal neutrons have been used to treat these tumors instead of thermal neutrons. Epithermal neutron (1 – 10,000eV) beams can deeply penetrate the tissue 3-6cm below the surface (Soloway et al., 1998). When an epithermal neutron enters a human body, it decelerates to a thermal neutron enabling easier boron neutron capture. In order to prevent the normal cells of patients from being irradiated by too much unwanted background radiation such as gamma rays and fast neutrons from the epithermal neutron beam port, patients must be irradiated with enough efficient doses and positioned as close to the beam port as possible within a period of time as short as possible (Walker, 1998). Hence, there are some requirements for the quality and intensity of the epithermal neutron beams. Within a shortening irradiation time, the degree of discomfort is also decreased. On the other hand, errors made by subtle movements from the patients can also be reduced with a shorter period of exposure. The quality of epithermal neutron beams can be measured by an Epithermal Neutron Flux Rate (n/cm2/s) to Unwanted Back Ground Radiation Flux Rate (n/cm2/s) ratio from the beam sources. The higher ratio it is, the higher the quality of the neutron beam. The accuracy of beam direction is also important. The patient’s head must be positioned flush against the beam port. The more accurate the beam direction is, the less damage is made to the surrounding normal tissues. Although thermal neutron beams were used clinically in Japan, epithermal beams with better abilities of penetration were used in the clinical trials in the United States and Europe in 1990s (Diaz, 2003; Barth et al., 2005). There are a number of reactors which produce beams that contain high percentages of neutrons with energies 13 between 1 and 10,000eV. For example, the beam at BMRR (The Brookhaven Medical Research Reactor, USA) has been evaluated, and its purity and intensity have showed that it is good enough for clinical use (Fairchild et al., 1989; Harling et al., 1990). 2.3 Dose Calculating and Treatment Planning by using Monte Carlo There are 4 main doses that contribute to BNCT: (1) the "boron dose"-dose from boron neutron capture reaction, Db; (2) the proton dose from nitrogen capture reaction, Dp; (3) the neutron dose, Dn; (4) the gamma dose, Dr (Chen, 2002). There are 2 ways for calculating BNCT doses by using Monte Carlo. “(1) The patient with low spatial resolution from MRI (Magnetic Resonance Imaging), CT (Computed Tomography) or etc, typically with a mesh size of 5-10 mm resolution, and calculates the neutron and gamma fluxes within these mesh regions. Thereafter, these fluxes are converted to doses using flux-to-kerma (kinetic energy released in matter) rate conversion factors. Assuming kerma is equal to absorbed dose to be true for the gamma component, the mesh size should not be less than 5 mm in size. (2) The patient with quite high spatial resolution from MRI (Magnetic Resonance Imaging), CT (Computed Tomography) or etc. The Monte Carlo calculation based on such a model directly tallies energy depositions within the various tissues from which dose is then derived. This is usually a long time-consuming and direct calculation procedure of a computer. The first way is applied to BNCT planning systems at Harvard-MIT and BNL for BNCT clinical trials. Two computer codes have been applied to clinical BNCT treatment planning, which are Harvard-MIT’s MacNCTPLAN and the Idaho National Energy and Engineering Laboratory’s SERA.” (IAEA, 2001) Both systems were designed specially for BNCT by using the Monte Carlo method. 14 3. Clinical Studies for Cancer Treatments by BNCT 3.1 BNCT Trials for Brain Tumors The treatment for glioblastomas and anaplastic astrocytomas by standard therapy such as conventional radiation therapy, surgery, and chemotherapy has had only few successful cases and the median survival time of treated patients today is similar to 30 years ago (Barth, 2003). BNCT was initially proposed to deal with these brain cancers such as glioblastoma multiforme (GBM). In 1951, the first clinical trial of BNCT for glioblastoma multiforme (GBM) patients was started at Brookhaven Graphite Research Reactor (BGRR) from Brookhaven National Laboratory (BNL) in the USA (Farr et al., 1954). From 1959 to 1961,a group of patients with brain tumours were treated by BNCT at the Brookhaven Medical Research Reactor (BMRR) (IAEA, 2001). During the same period, 18 malignant glioma patients were treated at the Massachusetts Institute of Technology Reactor (MITR). The results from the BNL and MIT were unsatisfactory due to insufficient penetration of the thermal neutron beams, inadequate accumulation of boron-carrying drug in the tumour (poor tumour-to-blood concentration ratios of boron-10 - less than 1) and excessive damage to healthy tissues including the scalp and the brain vasculature (Farr et al., 1954; Asbury et al., 1972; Sweet, 1997; Diaz et al., 2000; IAEA, 2001; Barth et al., 2005). As a result, all clinical trials in the USA had been stopped before 1994. Clinical trials of a group of 149 patients with various brain tumors were recovered by Hatanaka at the Hitachi Training Reactor (HTR) in Japan from 1968 to 1985 following Sweet’s research by using craniotomy with BNCT. Thermal neutron beams (whole-brain average equivalent doses: 9.5-15.6Gy(w) and Sulfhydryl 15 borane-Na2B12H11SH (BSH) (dose: 30-50mg/Kg) were applied to the BNCT processes within the trials. (Nakagawa & Hatanaka, 1997) (In 1967, the chemist-Soloway developed BSH as a boron-carrying drug at the Massachusetts General Hospital (Soloway et al., 1967). Hatanaka’s trial had 3 processes. First of all, the tumor was removed as much as possible by surgery. Then, BSH was slowly infused into the residual tumor. Half a day later, the residual tumor was finally irradiated by a thermal neutron beam at a nuclear reactor. (Hatanaka, 1991; Hatanaka & Nakagawa, 1994) Hatanaka and Nakagawa showed that 2 years survival rate was 11.4%, 5 years survival rate was 10.4%, and 10 years survival rate was 5.7% among the treated grade-4 GBM patients, which was superior to the conventionaly treatment (Nakagawa & Hatanaka, 1997; Nakagawa et al., 2003). As an adjuvant to surgery, Hatanaka’s results were impressive. However, the results were indicated to be exaggerated. Laramore et al. identified that Hatanaka had treated 14 USA GBM patients from 1987 to 1994. But only 12 patients' data were available. They pointed out that the median survival rate of the 12 patients was only 10.5 months, which there were no difference in survival time compare with the conventionally treated patients. (Laramore et al., 1994) Apart from this, from 1990 to 1996, a group of 44 grade-4 GBM patients were treated at the Kyoto University Reactor (KUR), 31 patients from the group had 11 months median survival time which was similar to Laramore et al.’s report (Kojo, 1997). From 1968 to 1997, Nakagawa et al. treated 130 grade-4 GBM patients by using similar processes to Hatanaka at Musashi Institute of Technology Reactor (MuITR) and Japan Atomic Energy Research Institute Reactor (JRR); they reported the results of 21 months median survival time of patients after the treatment, which was better than Hatanaka's results (Nakagawa & Hatanaka, 1997; Nakagawa et al., 2003). Although the early Japanese’s results seemed to be exaggerated, they still encouraged the USA and Europe restarting efforts to the BNCT research. Also, in the late 1980s, improvements in boron-carrying drug and neutron beams stimulated reconsideration of BNCT. Because of these two reasons, in 1994, new clinical trial started at BNL and 16 MIT in the USA. The treatments were given to sealed cranias by replacing thermal neutron beams to epithermal neutron beams. Epithermal neutron beams are capable to penetrate deeper to get over the superficial tissues of the scalp and cranias to reach the brain tumor without craniotomy (Diaz et al., 2000; IAEA, 2001). The beams can also reach the deeper situated brain tumors than the thermal neutron beams. The advantages of utilizing epithermal neutrons are outstanding. Because of these, they have been applied to most BNCT clinical trials for brain tumors since 1990s. In the USA, from September 1994 to May 1999, 53 GBM patients were treated by using epithermal neutron beams (whole-brain average equivalent doses: less than 5.5Gy(w) and BPA (4-Dihydroxyborylphenylalanine) (Snyder et al., 1958) (doses: 250-330mg/Kg) at BNL; they showed the results of 13.4 months median survival time of patients after the treatment (Diaz, 2003). From 1996 to 1999, 20 GBM patients were treated by using epithermal neutron beams (whole-brain average equivalent doses: less than 5.5Gy(w) and BPA (doses: 250-330mg/Kg) at Harvard-MIT; the results of 12 months median survival time of patients after the treatment were reported (Diaz, 2003). In 1997, the first European trial started in Holland. Since 1997, 26 GBM patients have been treated by using BSH (dose: 100mg/Kg) and epithermal neutron beams (whole-brain average equivalent doses: 8.6-11.4Gy(w) at the High Flux Reactor (HFR) in Petten. The median survival time of 13.2 months for the group of 26 patients was reported. So far, the trial is still continuing. (Surewein et al., 2002) In Germany, from October 1997 to July 2002, 24 GBM patients were treated by using epithermal neutron beams and BSH (doses: 100mg/Kg) at the European Organisation for Research and Treatment of Cancer Reactor (EORTCR); except the methodology, no other data was given (Vos et al., 2005). In Japan, from 1998 to 2004, the Japan Atomic Energy Agency (JAEA) treated 7 17 GBM patients. They used BSH (dose: 100mg/Kg, 1 hour infusion) and epithermal neutron beams (whole-brain average equivalent doses: 2.3-8.1Gy(w) for the treatments at the Japan Atomic Energy Research Institute Reactor-4 (JRR-4). The median survival time of 20.7 months for the group was reported (Yamamoto et al., 2004). Since 2005, the same group has carried out new trials. 8 GBM patients have been treated by using the combination of BPA (doses: 250mg/Kg, 1 hour infusion) and BSH (doses: 100mg/Kg) as boron 10-carrying drugs and epithermal neutron beams (whole-brain peak equivalent doses: approx. 13Gy(w). The trials are still continuing. Therefore, the results have not been reported yet. (Yamamoto et al., 2008) In Finland, from May 1999 to December 2001, 18 GBM patients were treated by using epithermal neutron beams (whole-brain average equivalent doses: 3-6Gy(w) and BPA (doses: 290-400mg/Kg) at Helsinki University Central Hospital and VTT (Technical Research Center); 61% of the treated patients had 12 months survival time (Joensuu et al., 2003). In Japan, from October 1999 to July 2002, only 5 GBM patients were treated by using a mixture of thermal and epithermal neutron beams and BSH (doses: 100mg/Kg); the marvelous results of 23.2 months median survival time of patients after the treatment were reported by Yamamoto et al. in 2004. In Sweden, from March 2001 to March 2005, Swedish researchers carried out clinical trials by using BPA (doses: 900mg/Kg, over 6 hours infusion) and epithermal neutron beams (whole-brain average equivalent doses: 3-6Gy(w) to treat 52 GBM patients at the Studsvik Medical AB Reactor; the median survival time of patients after the treatment were 14.2 months (H-Stenstam et al., 2006). In Rez, Czech Republic, since 2001, 5 GBM patients have been treated by using BSH (doses: 100mg/Kg) and epithermal neutron beams (whole-brain average equivalent doses: approx. 2Gy(w) at the Nuclear Research Institute (NRI) LVR-15 reactor. As 18 this series of trials are still being carried out, no results have been available yet. (Surewein et al., 2002) In Japan, since 2002, in Kyoto University Research Reactor Institute (KURRI), 27 GBM patients have been treated by using the combination of BPA (doses: 250-700mg/Kg, 1-6 hours infusion) and BSH (doses: 100mg/Kg, 1 hour infusion) as boron 10-carrying drugs and epithermal neutron beams (whole-brain peak equivalent doses: approx. 15Gy(w) at the Kyoto University Reactor (KUR). The results will be reported by the research team. (Miyatake et al., 2005) According to the cases shown above, BNCT seems to be at least equivalent or more effective to treat GBM compare with the conventional standard photon irradiation therapy. (The median survival time for the patients who have been treated by conventional photon irradiation therapy is between 10 to 12 months.) 3.2 BNCT Trials for Other Tumors Monte Carlo simulation of depth-dose distributions for cancers of liver, lung, pancreatic, prostate osteosarcoma etc. suggest that BNCT has the potential to be applied for treating those cancers under certain conditions (Matsumoto, 2007). A type of liver tumor that was recently treated by BNCT was metastasized adenocarcinoma of the colon (Surewein et al., 2002). There were a substaintial amount of patients who developed hepatic caner from colon adenocarcinoma. Here were the processes for the trial. At the beginning, the patients was infused BPA fructose (dose: 300mg/kg) for 2 hours. Then, hepatectomy was operated to the patient (Surewein et al., 2002). Thereafter, the liver was irradiated by a thermal neutron beam at the University of Pavia Laboratory Reactor. Finally, the treated liver was re-implanted inside the patient’s body. 2 years after the treatment, no tumor recurrence 19 happened to the patient and the tumor cells were almost vanished (Pinelli, 2004). Again, the trial showed that BNCT had the possibility to deracinate the root of an organ tumor. In September 2003, one patient with a recurrent papillary thyroid cancer who had previously been treated by convention therapies was treated by BNCT in Japan. So far, no recurrence and side effects have been observed to the patient who is still alive. (Hiratsuka et al., 2006) The results show that BNCT has the potential to cure primary or recurrent thyroid cancer. Head and neck recurrent tumors were another group of cancers that were recently treated by BNCT. Kato et al. reported that they have treated a group of 26 patients (1 had a 4 salivary gland carcinomas, 3 had sarcomas, and 19 had squamous cell carcinomas) with BNCT since 2001 (Kato et al., 2009). The whole group of patients had been treated by conventional therapy (chemotherapy, surgery and radiotherapy), and then developed recurrent tumors. During the trials, all of them were irradiated by epithermal neutron beams, and were injected with both BSH (doses: 5g) and BPA (doses: 250mg/kg). All patients survived 1-72 months after the treatments. The mean survival times were 13.6 months. Thereinto, 6 patients survived up to 6 years. (Kato et al., 2009) The results indicated that BNCT had the potential to be applied to the tumors which recurred after the treatments of conventional therapies, such as head and neck recurrent cancers. Besides GBMs, Cutaneous melanomas are another big cancer group which has been treated by BNCT since 1980s. Mishima et al. treated animals with either transplantable or primary melanomas by applying BPA as the boron-10 carrying drug to the experiments (Hiratsuka et al., 1989; Mishima & Ichihashi et al., 1989). Mishima’s experiments obviously initiated other investigators’ interests in BNCT researches by using BPA as a boron-10 carrying drug. In 1985, Mishima treated his first patient. He injected a total dose of 200mg BPA to the patient's tumor. About 20 45Gy(w) equivalent dose from the thermal neutron beam was given to the patient's melanoma. The patient's melanoma cell was totally disappeared by 9 months time. (Mishima & Ichihashi et al., 1989; Mishima & Honda et al., 1989) The success of the case proved that BNCT had the protential to treat radio-resistant tumors. Thereafter, more than 18 melanoma patients were treated by Mishima et al. (Larsson et al., 1997). Busse et al. treated a few patients with either cerebral metastases or cutaneous of melanoma by using a boron-10 carrying agent which was called BPA fructose (Coderre et al., 2003; Busse et al., 1999). The most outstanding case is the treatment of a patient who had an unresected cerebral metastasis in the occipital lobe (Barth et al., 2005). The tumor on the patient was given an equivalent dose of 24Gy(w) thermal neutron beam radiation. Magnetic Resonance Imaging (MRI) studies revealed that the tumor was completely regressed by 4 months (Busse et al., 1999). All the results showed that BNCT seemed to be more suitable to treat cerebral metastases or cutaneous of melanoma rather than glioblastoma multiforme (GBM). 21 4. Recent Development of BNCT It was recently found that BNCT with 'Bio-shuttled'-BPA and thermal neutrons was effective to kill some radio-resistant carcinoma cells. 'Bio-shuttled'-BPA was infused to radio-resistant HeLa-S cervix carcinoma cells, and then irradiated by a thermal neutron beam, which resulting no carcinoma cells were alive after 3 days (Braun et al., 2003). Carborane nucleotides were found to be a boron-10 delivery agent for BNCT which might be suitable for treatment of prostate tumor. It was showed that similar nucleoside bases may have different tissue-favorable characteristics, which could be selected as a BNCT boron-10 delivery agent for treatment of different kinds of cancer. 5-o-Carboranyluracil was recently discovered to be the most suitable boron 10-carrying drug for future investigations of prostate cancer treatment (Schinazi et al., 2004). Animal trial was carried out for lung cancer treatment by using BNCT. The folate receptor (FR) targeted liposomes were selected as indirect boron-10 delivery agent for Na3B20H17NH3 for the treatment of murine lung carcinoma in mice by using BNCT. The results showed that FR targeting was not significantly superior to the others in terms of tumor localization, but changing the boron 10-carrying drug may improve the outcome. (Pan et al., 2002) BNCT was considered to treat oral cancers. Because they could be easily exposed to the neutron beams. BNCT studies for oral cancer of hamsters were carried out. Human oral mucosa tumors were transplanted in the hamsters. BPA was proven to be a. effective boron-carrying agent for oral cancer (Kreimann & Dagrosa et al., 2001). The animals were treated by using thermal neutron beams and BPA. Complete regression with 78% of the tumor was observed 15 days after the treatment, and there 22 was no damage to the healthy oral tissue (Kreimann & Longhino et al, 2001). The possibility of applying BNCT to treat liver tumors was investigated by using normal liver cells in mice. BNCT with the use of boron-lipiodol was evaluated to have the potential to treat VX2 liver tumor. Some time after infusing boron-lipiodol into the liver, the researchers determined that the ratio of boron concentrations of the tumor to the healthy liver tissue was around 8. (Lin et al., 2002; Suzuki et al., 2004) According to the investigations shown above, BNCT still has the potential to be expanded for other cancer treatments. 23 5. Conclusion The elegant BNCT concept is based on the Boron-10 Neutron Capture Reaction to release alpha particles, recoiling lithium-7 nuclei and gamma rays with high linear energy transfer (LET) to kill tumor cell without the influence of the surrounding normal tissues. But there are a few critical problems that have to be solved for BNCT becoming another type of standard therapy in the future. Successful BNCT mainly rely on boron-10 delivery agents, neutron beams, dosimetry and experts in each related areas. Developing more effective and selective boron-10 delivery agents is the primary issue of BNCT. The agents should be able to deliver adequate amounts of boron-10 to the tumor cells, in order to achieve high ratio of (concentration of boron-10 in tumor cells)/(concentration of boron-10 in normal cells). Second, Up to date, only few clinical trials on BNCT have been carried out all over the world, one major reason is the limitation to the neutron sources from which are expensive nuclear reactors. These reactors are commonly located distant from the BNCT research centers of the cities/towns, because they are unwelcomed by the public due to safety issues. Therefore, there is a need for advanced accelerators and compact medical research reactors such as the operating one in the capital of China-Beijing. Apart from this, high quality neutron beam sources should be developed and applied to BNCT. Third, dosimetry of BNCT mainly includes two parts, which are boron-10 uptake (boron-10 dose) and neutron irradiation (neutron dose). It is necessary to find a way for real-time determination and monitoring for both doses, in order to optimize dose distributions around the tumor. So far, there are not any existing common/international standards for BNCT dosimetry. Finally, BNCT refers to a wide range of disciplines. Thus, it requires a wide range of experts in all BNCT related areas including administrators. The future of BNCT is promising. It has got the high potential to fill the gap of the treatment for the tough recurrent or primary malignancies before the coming age of 24 tissue regeneration, gene-modification, clone, nano robot or even 'matrix'. BNCT was initially proposed for malignant brain tumor such as glioblastoma multiforme (GBM). Although BNCT has been reported to be at least equivalent or more effective to treat GBM compare with the other conventional standard therapies. Up till now, it has not shown significant superiority to replace the others yet. Nevertheless, since the mid 1980s, BNCT has started to shown its great potential to treat other types of primary or recurrent cancers such as a kind of malignant skin cancers which are called melanomas, head and neck cancers, liver cancers and thyroid cancers. I believe that the BNCT will have a bright future if the researchers focus on studying and developing better tumor cell-seeking agents (boron-10 delivery agents). 25 Bibliography Azab A.K., Abu Ali H. and Srebnik M., 2006, Chapter 5: Boron Neutron Capture Therapy, Studies in Inorganic Chemistry, 22, 337-366 Barth R.F., M.D. 1 *, Soloway A.H., Ph.D. 2, Fairchild R.G., Ph.D. 3, Brugger R.M. and Ph.D. 3, 1992, Boron neutron capture therapy for cancer: Realities and prospects, Cancer, Dec 15, 70, 12. Barth R.F., Coderre J.A., Vicente M.G. and Blue T.E., 2005, Boron neutron capture therapy of cancer: current status and future prospects, Clin Cancer Res. Jun 1, 11, 3987. Barth R.F. and Joensuu H., 2007, Boron neutron capture therapy for the treatment of glioblastomas and extracranial tumours: As effective, more effective or less effective than photon irradiation? Radiotherapy and Oncology, 82, 2, February, 119-122. Barth R.F., 2009, Boron neutron capture therapy at the crossroads: Challenges and opportunities, Applied Radiation and Isotopes, 67, S3–S6. IAEA, 2001, Current status of neutron capture therapy, IAEA-TECDOC-1223. Linz U., 2008, Boron neutron capture therapy for glioblastoma: is it worth pursuing? Technol Cancer Res Treat., Feb, 7(1), 83-8. Luo Q.Y. and Zhu R.S., 2004, Boron neutron capture therapy, Journal of Isotopes, Aug, 17, 3. Pisarev M.A., Dagrosa M.A. and Juvenal G.J., 2007, Boron neutron capture therapy in 26 cancer: past, present and future, Arq Bras Endocrinol Metabol., Jul, 51(5), 852-6. Surewein W., Moss R. and Wittig A., (Eds.), 2002, Research and Development in Neutron Capture Therapy, Monduzzi Editore, Bologna. Walker S.J., 1998, Boron Neutron Capture Therapy: Principles and Prospects, Radiography, Volume 4, Issue 3, August 1998, 211-219. Yamamoto T., Nakai K. and Y. Matsumura A., 2008, Boron neutron capture therapy for glioblastoma, Cancer Letters, 262, 143. 27 References Asbury A.K., Ojemann R.G., Nielsen S.L. and Sweet W.H., 1972, Neuropathologic study of fourteen cases of malignant brain tumor treated by boron-10 slow neutron capture radiation, J. Neuropathol Exp Neurol, 31, 278-303. Azab A.K., Abu Ali H. and Srebnik M., 2006, Chapter 5: Boron Neutron Capture Therapy, Studies in Inorganic Chemistry, 22, 337-366 Barth R.F., 2003, A critical assessment of boron neutron capture therapy: an overview, J. Neurooncol., 62, 1. Barth R.F., Coderre J.A., Vicente M.G.H. and Blue T.E., 2005, Boron neutron capture therapy of cancer: current status and future prospects, Clin Cancer Res. Jun 1, 11, 3987. Barth R.F., Coderre J.A., Vicente M.G.H. and Blue T.E., 2006, Boron Neutron Capture Therapy, Encyclopedia of Medical Devices and Instrumentation, John Wiley and Sons. Braun K., Wolber G., Waldeck W., Pipkom R., Jenne J., Rastert R., Ehemann V., Eisenmenger A., Corban-Wilhelm H., Braun I., Heckl S. and Debus J., 2003, The enhancement of neutron irradiation of HeLa-S cervix carcinoma cells by cell-nucleus-addressed deca-p-boronophenylalanine, Eur. J. Med. Chem., 38, 587. Busse P.M., Zamenhof R.G., Harling O.K., et al., 1999, The Harvard-MIT BNCT Program: overview of the clinical trials and translational research. Proceedings of the 11th International Congress of Radiation Research, Jul 18-23, Dublin, Ireland, 2, 702. 28 Carlsson J., Kullberg E.B., Capala J., et al., 2003, Ligand liposomes and boron neutron capture therapy, J. Neurooncol., 62, 47. Chen D., 2003, Advance in Boron Neutron Capture Therapy for Malignant Tumors, Bull Med Res, Apirl, 32, 4. Coderre J.A., Glass J.D., Packer S., Micca P. and Greenberg D., 1990, Experimental boron neutron capture therapy for melanoma: systemic delivery of boron to melanotic and amelanotic melanoma, Pigment Cell Res., 3, 310. Coderre J.A., Turcotte J.C., Riley K.J., Binns P.J., Harling O.K. and Kiger III W.S., 2003, Boron neutron capture therapy: cellular targeting of high linear energy transfer radiation, Technol Cancer Res Treat, 2, 1. Diaz A.Z., Coderre J.A., Chanana A.D. and Ma R., 2000, Boron neutron capture therapy for malignant gliomas, Annals of Medicine, 32, 1, 81-85. Diaz A.Z., 2003, Assessment of the results from the phase I/II boron neutron capture therapy trials at the Brookhaven National Laboratory from a clinician's point of view, J. Neurooncol, 62, 101. El-Zaria M.E., Doerfler U. and Gabel D., 2002, Synthesis of [(aminoalkylamine)-n-aminoalkyl] azanonaborane(11) derivatives for boron neutron capture therapy, J. Med. Chem., 45, 5817. Fairchild R.G., Kalef-Ezra J.A., Fiarman S., Wielopolski L., Hanz J., Mussolino S., et al, 1989, Optimization of an epithermal beam for NCT at the Brookhaven Medical Research Reactor (BMRR), Stralenther und Onkol, 165, 84-6. Farr L.E., Sweet W.H., Locksley H.B. and Robertson J.S., 1954, Neutron capture 29 therapy of gliomas using boron, Trans. Am. Neurol. Assoc, 13, 110. Gabel D., Foster S. and Fairchild R.G., 1987, The Monte Carlo simulation of the biological effect of the 10B(n,a)7L reaction in cells and tissue and its implication for boron neutron capture therapy, Radiat. Res., 111, 14. H-Stenstam B., Pellettieri L., Skold K., et al., 2006, Neuropathological post-mortem evaluation of GBM patients treated by BNCT, In: 12th international congress on neutron capture therapy, Takamatsu, Japan, October 9–12, p34. Harling O.K., Bernard J.A. and Zamenhof R.G., 1990, Neutron beam design, development and performance for neutron capture therapy, New York, Plenum Press, 169-183 and 185-9 Hawthorne M.F. and Pitochelli A.R., 1959, The Isolation of the Icosahedral B12 H12-2 Ion, J. Am. Chem. Soc., 81, 5519. Hatanaka H., 1991, Boron neutron capture therapy for brain tumors, In: Karin ABMF, Laws E, editors, Glioma.Berlin: Springer-Verlag, 233. Hatanaka H. and Nakagawa Y., 1994, Clinical results of long-surviving brain tumor patients who underwent boron neutron capture therapy. Int. J. Radiat. Oncol. Biol. Phys, 28, 1061. Hiratsuka J., Kono, Mishima Y., 1989, RBEs of thermal neutron capture therapy and 10B(n,a)7Li reaction on melanoma-bearing hamsters, Pigment Cell Res, 2, 352. Hiratsuka J, Morita N, Aihara T, Imajo Y, Maruhashi A. and Ono K., 2006, First clinical trial of neutron capture therapy for thyroid cancer, In: Nakagawa Y., Kobayashi T. and Fukuda H. (eds), Proceedings of ICNCT-12, Kagawa, Japan, 7-9. 30 IAEA, 2001, Current status of neutron capture therapy, IAEA-TECDOC-1223. Ichihashi M., Nakanishi T. and Mishima Y., 1982, Specific killing effect of 10B1-para-boronophenylalanine in thermal neutron capture therapy of malignant melanoma: in vitro radiobiological evaluation, J. Invest. Dermatol, 78, 215. Isaac M.F. and Kahl S.B., 2003, Synthesis of ether and carbonlinked polycarboranyl porphyrin dimers for cancer therapies, J. Organomet. Chem., 680, 232. Ivanov D., Bachovchin W.W. and Redfield A.G., 2002, Boron-11 pure quadrupole resonance investigation of peptide boronic acid inhibitors bound to a-lyticprotease, Biochemistry, 41, 1587. Joensuu H., Kankaanranta L., Seppala T., et al., 2003, Boron neutron capture therapy of brain tumors: clinical trials at the Finnish facility using boronophenylalanine, J Neuro-Oncol, 62, 123. Justus E., Awad D., Hohnholt M., Schaffran T., Edwards K., Karlsson G., Damian L. and Gabel D., 2007, Synthesis, liposomal preparation, and in vitro toxicity of two novel dodecaborate cluster lipids for boron neutron capture therapy, Bioconjug. Chem., 18(4), 1287. Kabalka G.W. and Yao M.L., 2003, Synthesis of a potential boron neutron capture therapy agent: 1-aminocyclobutane-1-carboxylic acid bearing a butylboronic acid side chain, Synthesis, 18, 2890. Kato I., Fujita Y., Maruhashi A., Kumada H., et al., 2009, Effectiveness of boron neutron capture therapy for recurrent head and neck malignancies, Appl. Radiat. Isot., 67, s37. 31 Kojo O., 1997, Advances in Neutron Capture Therapy, Excerpta Medica: International Congress Series 1132, Eds. Larsson B., Crawford J. and Weinreich R., Elsevier, 1, 39–45. Kreimann E.L., Itoiz M.E., Dagrosa A., Garavaglia R., Farias S., Batistoni D. and Schwint A.E., 2001, The hamster cheek pouch as a model of oral cancer for boron neutron capture therapy studies: selective delivery of boron by boronophenylalanine, Cancer Res., 61, 8775. Kreimann E.L., Itoiz M.E., Longhino J., Blaumann H., Calzetta O. and Schwint A.E., 2001, Boron neutron capture therapy for the treatment of oral cancer in the hamster cheek pouch model.Cancer Res., 61, 8638. Laramore G.E.,Wootton P., Livesey J.C., et al., 1994, Boron neutron capture therapy: a mechanism for achieving a concomitant tumor boost in fast neutron radiotherapy, IntJRadiat Oncol Biol Phys, 28, 1135. Larsson B., Crawford J. and Weinreich R., 1997, Advances in neutron capture therapy, Medicine and physics, Amsterdam, Elsevier, 1, 10. Lin W.Y., Chi C.W., Ho Y.J., Wu I.C., Chung Y.T.,Chen S.D. , Chou F.I., Kai J.J., Lui W.Y., Chen T.J. and Lin Y., 2002, Boron-lipiodol: a potential new drug for the treatment of liver tumors, Anticancer Res., 22, 3989. Matsumoto T., 2007, Nuclear Instruments and Methods in Physics Research Section A: Accelerators, Spectrometers, Detectors and Associated Equipment, 580, 1, 552-557 Mishima Y., Ichihashi M., Hatta S., Honda C., Yamamura K. and Nakagawa T., 1989, New thermal neutron capture therapy for malignant melanoma. Melanogenesis-seeking 10B molecular-melanoma cell interaction from in vitro to first 32 clinical trial, Pigment Cell Res, 2, 226. Mishima Y., Honda C., Ichibashi M., et al., 1989, Treatment of malignant melanoma by single neutron capture therapy with melanoma-seeking 10B-compound. Lancet, 1, 388. MIT, 2008, The Basics of Boron Neutron Capture Therapy, online, accessed 18/08/08, http://web.mit.edu/nrl/www/bnct/info/description/description.html Miyatake S., Kajimoto Y., Kawabata S., et al., 2005, Modified boron neutron capture therapy for malignant gliomas performed using epithermal neutron and two boron compounds with different accumulation mechanisms: an efficacy study based on findings on neuroimages, J. Neurosurg., 103, 1000. Nakagawa Y. and Hatanaka H., 1997, Boron neutron capture therapy: Clinical brain tumor studies, J. Neurooncol, 33, 105. Nakagawa Y., Pooh K., Kobayashi T., Kageji T., Uyama S., Matsumura A. and Kumada H., 2003, Clinical review of the Japanese experience with boron neutron capture therapy and a proposed strategy using epithermal neutron beams, J. Neurooncol, 62, 87. NCI, 2009, Treatment Choices for Men With Early-Stage Prostate Cancer, online, accessed http://nci.nih.gov/cancertopics/prostate-cancer-treatment-choices/allpages, 22/06/09, National Cancer Institute. Olejiniczak A.B., Koziolkiewcz M. and Lesnikowski Z.J., 2002, Carboranyl oligonucleotides: 4. Synthesis and physicochemical studies of oligonucleotides containing 20-O-(o-carboran-1-yl)methyl group, Antisense Nucleic Acid Drug Dev., 33 12, 79. Olsson P., Gedda L., Goike H., et al., 1998, Uptake of a boronated epidermal growth factor-dextran conjugate in CHO xenografts with and without human EGF-receptor expression, Anticancer Drug Des., 13, 279. Pan X.Q., Wang H. and Lee R.J., 2002, Boron delivery to a murine lung carcinoma using folate receptor-targeted liposomes, Anticancer Res., 22, 1629. Pinelli T., 2004, Neutron capture therapy for liver cancer metastases, Abstracts of the 11th World Congress on Neutron Capture Therapy, Boston, MA, Oct 11-15, 52 Schinazi R.F., Hurwitz S.J., Liberman I., Glazkova Y., Mourier N.S., Olson J. and Keane T., 2004, Tissue disposition of 5-o-carboranyluracil--a novel agent for the boron neutron capture therapy of prostate cancer, Nucleosides Nucleotides Nucleic Acids, 23, 291. Snyder H.R., Reedy A.J. and Lennarz W., 1958, Synthesis of aromatic boronic acids. Aldehydo boronic acids and a boronic acid analog of tyrosine, J. Am. Chem. Soc., 80, 835. Soloway A.H., Wright R.L. and Messer J.R., 1961, Evaluation of boron compounds for use in neutron capture therapy of brain tumors. I. Animal investigationsJ. Pharmacol. Exp Ther., 134, 117. Soloway, A.H., Hatanaka H. and Davis M.A., 1967, Penetration of Brain and Brain Tumor, VII, Tumor-binding Sulfhydryl Boron Compounds, J. Med. Chem., 10, 714.. Soloway A.H., Tjarks W., Barnum B.A., Rong F.G., Barth R.F., Codogni I.M. and Wilson J.G., 1998, The chemistry of neutron capture therapy, Chem. Rev., 98, 1515. 34 Surewein W., Moss R. and Wittig A., (Eds.), 2002, Research and Development in Neutron Capture Therapy, Monduzzi Editore, Bologna, p993, 1107 & 1117. Suzuki M., Sakurai Y., Masunaga S., Kinashi Y., Nagata K. and Ono K., 2004, Dosimetric study of boron neutron capture therapy with borocaptate sodium (BSH)/lipiodol emulsion (BSH/lipiodol-BNCT) for treatment of multiple liver tumors, Int. J. Radiat. Oncol. Biol. Phys., 58, 892. Sweet W.H., Soloway A.H. and Brownell G.L., 1960, Studies relevant to slow neutron capture therapy of brain tumor, Acta Unio. Int. Contra Cancrum., 16, 1216. Sweet W.H., 1997, Early history of development of boron neutron capture therapy of tumors, J Neurooncol, 33, 19-26. Tietze L.F., Griesbach U., Bothe U., Nakamura H. and Yamamoto Y., 2002, Novel carboranes with a DNA binding unit for the treatment of cancer by boron neutron capture therapy, Chembiochem, 3, 219. Tietze L.F., Griesbach U., Schuberth I., Bothe U., Marra A. and Dondoni A., 2003, Novel carboranyl C-glycosides for the treatment of cancer by boron neutron capture therapy, Chem. Eur. J., 9(6), 1296. Tjarks W., 2001, The use of boron clusters in the rational design of boronated nucleosides for neutron capture therapy of cancer, J. Organomet. Chem., 614-615, 37-47. Vos M.J., Turowski B., Zanella F.E., et al., 2005, Radiologic findings in patients treated with boron neutron capture therapy for glioblastoma multiforme within EORTC trial 11961, Int J Rad Oncol Biol Phys 61, 392. 35 Walker S.J., 1998, Boron Neutron Capture Therapy: Principles and Prospects, Radiography, Volume 4, Issue 3, August 1998, 211-219. Wikipedia, 2008, Boron Neutron Capture Therapy, online, accessed 18/08/08, http://en.wikipedia.org/wiki/Boron_Neutron_Capture_Therapy. Wikipedia 1, 2009, Blood-brain barrier, online, accessed 11/07/09, http://en.wikipedia.org/wiki/Blood-brain_barrier. Wikipedia 2, 2009, X-ray computed tomography, online, accessed 11/07/09, http://en.wikipedia.org/wiki/Computed_tomography. Wikipedia 3, 2009, Kerma (physics), online, accessed 11/07/09, http://en.wikipedia.org/wiki/Kerma_(physics). Wikipedia 4, 2009, Linear energy transfer, online, accessed 11/07/09, http://en.wikipedia.org/wiki/Linear_energy_transfer. Wikipedia 5, 2009, Magnetic resonance imaging, online, accessed 11/07/09, http://en.wikipedia.org/wiki/MRI. Yamamoto, T., Matsumura, A., Nakai, K., et al., 2004, Current clinical results of the Tsukuba BNCT trial, Applied Radiat Isotopes, 61, 1089. Yamamoto T., Nakai K. and Y. Matsumura A., 2008, Boron neutron capture therapy for glioblastoma, Cancer Letters, 262, 143. Zamenhof R.G., Solares G.R. and Harling O.K., 1994, Topics in Dosimitry and Treatment Planning for Neutron Capture Therapy, Advanced Medical Publishing: 36 Madison, 1994. 37