Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
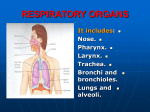
An Overview of the Respiratory System The respiratory system includes many different structures working together for a common purpose. These structures include the nose, the nasal cavity and sinuses, pharynx, larynx, trachea, and smaller conducting passageways leading to the gas exchange surfaces of the lungs. The respiratory tract consists of the airways that carry air to and from the surfaces of these surfaces and can be divided into two parts. The conducting zone extends from the entrance of the nose to the nasal cavity to the smallest bronchioles of the lungs. It consists of the nose, pharynx, larynx, trachea, bronchi, bronchioles, and terminal bronchioles. Their function is to filter, warm, and humidify the air and conduct it into the lungs. The respiratory zone of the tract includes the delicate bronchioles and air sacs, also called alveoli, where gas exchange takes place between the air and blood. The respiratory system also consists of the respiratory tract and its associated tissues, organs, and supporting structures. These are also divided into two parts: (1) The upper respiratory system includes the nose, pharynx, and associated structures. These passageways also filter, warm, and humidify the air, protecting the more fragile conduction and exchange surfaces of the lower respiratory system from debris and pathogens. (2) The lower respiratory system includes the larynx, trachea, bronchi, and lungs. The filtering, warming, and moistening of inhaled air begins at the entrance of the nose to the upper respiratory system and continues throughout the rest of the conducting zone. Most foreign particles and pathogens have been removed by the time the air reaches lung alveoli. The Upper Respiratory System The Nose and Nasal Cavity The head has two openings through which substances such as air and food can enter the bodythe nose and the mouth. Although air can enter through either of these passageways, the nose is the primary passageway for air entering the respiratory system. The nose consists of more than what you see on someone’s face. In fact, the nose can be divided into two parts, the external and internal portions. The external nose, the skin and muscle-covered portion of the nose visible on the face, is an extension of bone and cartilage with two entryways and an internal dividing wall. Three large cartilages that project from the skull to form the framework of the external nose are the septal nasal cartilage, the paired major alar cartilages, and the minor alar cartilages, which define the cartilage skeleton of the nose. The major and minor alar cartilages form the inner part of the lateral sides of the nose. The septal cartilage divides the external nose into right and left chambers. The external nose is flexible to some extent because it consists of hyaline cartilage. Air normally enters the respiratory system through the external nares, also called, nostrils, which open into the nasal cavity. The nasal vestibule is the portion of the nasal cavity enclosed by the flexible tissues of the nose. The skin of the nasal vestibule is composed of many coarse hairs that extend across the external nares and sebaceous and sweat glands that secrete onto its surface. Large airborne particles such as sand, sawdust, and even insects are trapped in these hairs and are prevented from entering the nasal cavity. The upper lining of each nasal vestibule turns into a mucous membrane that continues deeper into the nasal cavity. Deeper into the skull, beyond the nasal vestibules, is the internal nose. The internal nose is a large cavity in the frontal part of the skull that lies below the nasal bone and above the mouth. Anteriorly, the internal nose fuses with the external nose, and posteriorly it connects with the pharynx through two openings called the internal nares or choanae. The lateral walls of the internal nose are composed by the ethmoid, maxillae, lacrimal, palatine, and inferior nasal conchae bones. The ethmoid bone forms the roof of the internal nose and the hard palate, formed by the maxillary and palatine bones, forms the floor of the nasal cavity and separates the oral and nasal cavities. This large cavity within the skull, called the nasal cavity, forms most of the nose and is divided into two regions-the large inferior respiratory region and the small superior olfactory region. Like the nasal vestibules, the nasal cavity is also divided into right and left halves by a nasal septum. The ventral part of the nasal septum is formed by the septal nasal cartilages, which attaches to the vomer bone and perpendicular plate of the ethmoid bone. These bones form the dorsal part of the nasal septum. A deviated septum can result from a strong impact to the nasal region. The fragile nasal septal bones can break or the cartilage portion of the nasal septum can be separated from the bony portion and become displaced to one side during the healing process leading to a narrowing of one side of the nasal cavity. This makes it more difficult to breathe through that side of the nose. Three shelves formed by projections of the superior, middle, and inferior nasal conchae extend out of each lateral wall of the nasal cavity. The conchae, almost reaching the nasal septum, subdivide each side of the nasal cavity into the superior, middle, and inferior meatuses. These are narrow grooves rather than open passageways, and the incoming air bounces off the conchal surfaces and churns around like water flowing over rapids. Mucous membrane lines the cavity and its shelves so this turbulence serves a purpose, as the air eddies and swirls, small airborne particles come in contact with the mucus. The turbulence also allows extra time for warming and humidifying the incoming air. The olfactory receptors lie in the membrane lining the superior nasal conchae and adjacent nasal septum. This region is called the olfactory epithelium and inferior to it is a mucous membrane containing capillaries and pseudostratified ciliated columnar epithelium with many 2 goblet cells. Blood circulating in the capillaries warms inhaled air whirling around the conchae and meatuses. Mucus secreted by the goblet cells traps dust particles and moistens the air. The cilia move the mucus and its contents toward the pharynx, at which point they can be removed from the respiratory tract. The Pharynx The nose, mouth and throat connect to each other by a common passageway or chamber called the pharynx. The pharynx is a funnel-shaped tube shared by the digestive and respiratory systems. It extends between the internal nares and the entrances to the trachea and esophagus. Its wall is lined with mucous membrane and composed of skeletal muscles. The veins of the pharynx drain into the pterygoid plexus and the internal jugular veins. Most of the muscles of the pharynx are innervated by nerve branches from the glossopharyngeal (IX) and vagus (X) nerves. The pharynx serves as a passageway for air and food, provides a chamber for speech sounds, and houses the tonsils, which aid in immunological reactions against foreign invaders. The curving superior and posterior walls are closely bound to the axial skeleton, but the lateral walls are rather flexible and muscular. The pharynx is divided into three regions: the nasopharynx, the oropharynx, and the laryngopharynx. The Nasopharynx The nasopharynx, is the superior portion of the pharynx. Its connected to the posterior portion of the nasal cavity by means of the internal nares and is separated from the oral cavity by the soft palate. There are five openings in the wall of the nasopharynx: two internal nares, two openings that lead into the eustachian tubes, and the opening into the oropharynx. The pharyngeal tonsil is located on the posterior wall of the nasopharynx and the lateral walls contain the openings contain the openings of the eustachian tubes or auditory tubes. The nasopharynx exchanges small amounts of air with the eustachian tubes to equalize air pressure between the pharynx and the middle ear. The Oropharynx The intermediate portion of the pharynx, the oropharynx, extends between the soft palate and the base of the tongue at the level of the hyoid bone. The posterior portion of the oral cavity communicates directly with the oropharynx, just as the posterior and inferior portions of the nasopharynx do. In addition to communicating upward with the nasopharynx and downward with the laryngopharynx, it has an anterior opening, the fauces, which is the passageway between the oral cavity and the oropharynx. The oropharynx is lined with nonkeratinized stratified squamous epithelium because it is subject to abrasion by food particles. Two pairs of tonsils, the palatine and lingual tonsils are also found in the oropharynx. 3 The Laryngopharynx The laryngopharynx, or hypopharynx, is a the most inferior part of the pharynx, and like the oropharynx it is lined by nonkeratinized stratified squamous epithelium that can resist abrasion, chemical attack, and pathogenic invasion. The laryngopharynx is narrow and it includes the region of the pharynx lying between the hyoid bone and the entrance to the esophagus. The Lower Respiratory System The Larynx The larynx, or voice box, is a short passageway that connects the laryngopharynx with the trachea. The larynx is essentially a cylinder whose cartilaginous walls are stabilized by ligaments or skeletal muscles or both. It lies in the midline of the neck anterior to the fourth through sixth cervical vertebrae (C4-C6). Cartilages of the Larynx The wall of the larynx is composed of nine pieces of cartilage. Three occur singly (thyroid cartilage, epiglottis, and cricoids cartilage), and three occur in pairs (arytenoid, cuneiform, and corniculate cartilages). The arytenoids cartilages are the most important of the paired cartilages because the positions and tensions of the vocal cords. The epiglottis is a large, leaf-shaped piece of elastic cartilage that folds back during swallowing to prevent the entry of liquids or solid food into the respiratory passageways. The narrowed passageway through the larynx is called the glottis. The glottis is surrounded and protected by the larynx. It consists of a pair of folds of mucous membrane, the vocal cords in the larynx, and the space between them called the rima glottidis. The thyroid cartilage, or Adam’s apple, is the largest laryngeal cartilage and forms most of the anterior and lateral walls of the larynx. It consists of two fused plates of hyaline cartilage that form its anterior wall and give it a triangular shape. The thyrohyoid membrane is the ligament that connects the thyroid cartilage to the hyoid bone. The thyroid cartilage sits superior to the cricoid cartilage. The cricoid cartilage is a ring of hyaline cartilage that forms the inferior wall of the larynx. The cricotracheal ligament attaches the cricoids cartilage to the first ring of cartilage of the trachea. The thyroid cartilage is connected to the cricoids cartilage by the cricothyroid ligament. The cricoid cartilage is the landmark for making an emergency airway called a tracheotomy. 4 The superior surface of the cricoid cartilage articulates with the small paired arytenoid cartilages. The arytenoids cartilages are triangular pieces of mostly hyaline cartilage that articulate with the superior border of the enlarged portion of the cricoid cartilage. The corniculate cartilages articulate with the arytenoid cartilages. The corniculate and arytenoid cartilages are involved with the opening and closing of the glottis and the production of sound. The cuneiform cartilages are club-shaped elastic cartilages anterior to the corniculate cartilages and support the vocal folds and lateral aspects of the epiglottis. Structures of Voice Production The mucous membrane of the larynx forms two pairs of folds: a superior pair called the ventricular folds (false vocal folds) and an inferior pair called the vocal cords (true vocal cords). The rima vestibuli is the space between the ventricular folds. When the ventricular folds are brought together, they function in holding the breath in the thoracic cavity against pressure, such as might occur when a person strains to lift a heavy object. Laryngeal Muscles The larynx is associated with two different groups of muscles, the intrinsic laryngeal muscles and the extrinsic laryngeal muscles. The intrinsic laryngeal muscles have two major functions. One group regulates tension in the vocal cords, while the second set opens and closes the glottis. The extrinsic laryngeal muscles position and stabilize the larynx. During swallowing, both extrinsic and intrinsic muscles work together to prevent food or drink from entering the glottis. Pitch is controlled by the tension on the vocal cords. If they are pulled firmly by the muscles, they vibrate faster, resulting in a higher pitch. Decreasing the muscular tension on the vocal cords produces lower-pitch sounds. Sounds originate from the vibration of the vocal cords, but other structures are needed for turning sound into recognizable speech. The pharynx, mouth, nasal cavity, and paranasal sinuses all act as resonating chambers that give the voice its individual and human quality. Whispering is accomplished by closing all but the posterior portion of the rima glottidis. Since the vocal cords do not vibrate during whispering, there is no pitch to this form of speech. The Trachea The epithelium of the larynx is continuous with that of the trachea, or windpipe. The trachea is a tough, flexible tubular passageway for air and it is located anterior to the esophagus. It extends from the larynx to the superior border of the fifth thoracic vertebrae where it divides into the right and left primary bronchi. 5 The layers of the tracheal wall, from deep to superficial, are: the mucosa, the submucosa, the middle tunic, and the adventitia. The mucosa of the trachea consists of an epithelial layer and an underlying layer of lamina propia. The lamina propia is a layer of loose connective tissue which separates the respiratory epithelium from underlying cartilages. The submucosa consists of areolar connective tissue that contains seromucous glands and their ducts. The middle tunic contains horizontal rings of hyaline cartilage that resemble the letter C. The rings are stacked one above the other and are connected to each other by dense connective tissue. The open part of each C-shaped cartilage ring faces posteriorly toward the esophagus and is spanned by a fibromuscular membrane. Within this membrane are transverse smooth muscle fibers, called the trachealis muscle, and elastic connective tissue that allow the trachea to change in diameter during inhalation and exhalation. This feature is important for maintaining efficient air flow. The adventitia of the trachea consists of areolar connective tissue that joins the trachea to surrounding tissues. The Primary Bronchi The trachea branches within the mediastinum, dividing into the right and left primary bronchi. Like the trachea, the primary bronchi consist of incomplete rings of cartilage. The internal ridge where the trachea divides into right and left primary bronchi is called the carina. The mucous membrane of the carina is one of the most sensitive areas of the entire larynx and trachea for triggering a cough reflex. The primary bronchi divide to form smaller bronchi once they enter the lungs, called the secondary (lobar) bronchi, one for each lobe of the lung. The secondary bronchi continue to branch, forming even smaller bronchi, called tertiary (segmental) bronchi. These then divide into bronchioles. Bronchioles in turn branch repeatedly, and the smallest ones branch into still smaller tubes called terminal bronchioles. This widespread branching is commonly referred to as the bronchial tree due to its resemblance of an inverted tree. During exercise, activity in the sympathetic division of the autonomic system increases and causes the release of the hormones epinephrine and norepinephrine, both of which cause relaxation of smooth muscle in the bronchioles, which dilates the airways. This results in improved lung ventilation because it allows air to reach the alveoli quicker. The parasympathetic division of the autonomic nervous system and mediators of allergic reactions such as histamine cause contractions of the bronchiolar smooth muscle and result in constriction of distal bronchioles. 6 The Lungs The left and right lungs are located in the left and right pleural cavities in the thoracic cavity. Each lung is like a blunt cone with the tip, or apex, pointing superiorly. The broad concave inferior portion, or base, of each lung rests on the superior surface of the diaphragm. Each lung is surrounded by a protective, double-layered serous membrane called the pleural membrane. The superficial layer is called the parietal pleura and it lines the wall of the thoracic cavity. The deep layer is called the visceral pleura and it is attached to the lungs themselves. The pleural cavity is a small space between the visceral and parietal pleurae. Inflammation of the pleural membrane, called pleurisy or pleuritis, may cause pain in its early stages due to friction between the parietal and visceral layers of the pleura. If the inflammation persists, excess fluid builds up in the pleural space, a condition known as pleural effusion. Removal of this excess fluid can be accomplished without injuring lung tissue by inserting a needle anteriorly through the seventh intercostals space, a procedure termed thoracentesis. The surface of the lung lying against the rib is called the costal surface. The mediatinal (medial) surface of each lung contains a region, the hilum, through which bronchi, blood vessels, lymphatic vessels, and nerves enter and exit. These structures are firmly anchored in a meshwork of dense connective tissue and constitute the root of the lung. Medially, the left lung also consists of a concavity, the cardiac notch, in which the heart lies. Due to the space taken up by the heart, the left lung is smaller than the right lung. One or two fissures divide each lung into lobules. Both lungs have an oblique fissure, which extends inferiorly and anteriorly, and the right lung also has a horizontal fissure. The oblique fissure in the left lung separates the superior lobe from the inferior lobe. In the right lung, the inferior part of the oblique fissure separates the inferior lobe from the middle lobe, which is bordered superiorly by the horizontal fissure. Each lobe has its own secondary (lobar) bronchus. Therefore, the right primary bronchus gives rise to three secondary bronchi called the superior, middle, and inferior secondary bronchi. The left primary bronchus gives rise to superior and inferior secondary bronchi. The secondary bronchi give rise to the tertiary bronchi within the lung. There are ten tertiary bronchi in each lung. The segment of lung tissue that each tertiary bronchus supplies is called a bronchopulmonary segment. Each bronchopulmonary segment of the lungs has many small compartments called lobules. Each lobule is wrapped in elastic connective tissue and contains a branch from a terminal bronchiole. The terminal bronchioles subdivide into even smaller branches called respiratory bronchioles. Respiratory bronchioles then subdivide into several alveolar ducts. The respiratory passages from the trachea to the alveolar ducts contain about 25 orders of branching. 7 Surrounding the alveolar ducts are many alveoli and alveolar sacs. An alveolus is a cup-shaped outpouching lined by simple squamous epithelium and supported by a thin elastic membrane. An alveolar sac is a common chamber connected to several individual alveoli. The walls of alveoli consist of two types of alveolar epithelial cells. Type I alveolar cells, the predominant cells, form a nearly continuous lining of the alveolar wall. These cells are unusually thin and delicate. They are also the main sites of gas exchange. Type II alveolar cells, also called septal cells, are fewer in number and are located between type I alveolar cells. These large cells produce an oily secretion containing a mixture of phospholipids and lipoproteins. This secretion, known as surfactant, coats the inner surface of each alveolus. Associated with the alveolar wall are alveolar macrophages, wandering phagocytes that remove dust particles and other debris in the alveolar spaces. Fibroblasts that produce reticular and elastic fibers are also present. The exchange of oxygen and carbon dioxide between the air spaces in the lungs and the blood takes place by diffusion across the alveolar and capillary walls, which together form the respiratory membrane. The respiratory membrane consists of four layers: the alveolar wall, an epithelial basement membrane, a capillary basement membrane, and endothelial cells. The alveolar wall consists of a layer of type I and type II alveolar cells and associated alveolar macrophages. The epithelial basement membrane underlies the alveolar wall. The capillary basement membrane is fused to the epithelial basement membrane. The endothelial cells are part of the capillary. Despite having several layers, the respiratory membrane is very thin. This thinness allows rapid diffusion of gases. The Blood Supply to the Lungs The lungs receive blood through two sets of arteries: pulmonary and bronchial arteries. Deoxygenated blood passes through the pulmonary trunk, which divides into a left pulmonary artery that enters the left lung and a right pulmonary artery that enters the right lung. Oxygenated blood is returned to the heart by way of the four pulmonary veins, which drain into the left atrium. Bronchial arteries branch from the aorta and deliver oxygenated blood to the lungs. Most blood returns to the heart via pulmonary veins but some blood, however, drains into bronchial veins and returns to the heart via the superior vena cava. The nerve supply of the lungs is derived from branches of the vagus (X) nerves and sympathetic trunks. Pulmonary Ventilation (Breathing) Respiration is the exchange of gases between the atmosphere, blood, and body cells. It takes place in three simple steps: pulmonary ventilation, external (pulmonary) respiration, and internal (tissue) respiration. 8 Pulmonary ventilation, or breathing, is the first process, and it consists of inhalation and exhalation of air. It is the exchange of air between the atmosphere and the air spaces of the lungs. External respiration is the exchange of gases between the air spaces of the lungs and blood in pulmonary capillaries across the respiratory membrane. The blood gains oxygen and loses carbon dioxide during this process. Internal respiration is the exchange of gases between blood in systemic capillaries and tissue cells. The blood loses oxygen and gains carbon dioxide during this process. Inhalation Breathing in is called inhalation or inspiration. For inhalation to occur, the lungs must expand. This involves the contraction of the main muscles of inhalation-the diaphragm and/or external intercostals. The diaphragm is the most important muscle of inhalation and it forms the floor of the thoracic cavity. During inhalation, the diaphragm contracts and flattens, increasing its diameter. At the same time the diaphragm contracts, the external intercostals contract. When these muscles contract, the ribs are pulled superiorly and the sternum is pushed anteriorly, therefore increasing the diameter of the thoracic cavity. During deep, forceful inhalations, accessory muscles of inspiration also participate in increasing the size of the thoracic cavity. Some of these muscles include the sternocleidomastoid muscles which elevate the sternum, the scalene muscles which elevate the first two ribs, and the pectoralis minor muscles which elevate the third through fifth ribs. Exhalation Breathing out is called exhalation or expiration. Normal exhalation depends on two factors: the recoil of elastic fibers that were stretched during inhalation and the inward pull of surface tension due to alveolar fluid. Exhalation begins when the inspiratory muscles relax. As the external intercostals relax, the ribs move inferiorly and the diaphragm relaxes. As the diaphragm relaxes, its dome moves superiorly. These movements decrease the diameters of the thoracic cavity and air then flows outwards into the atmosphere. Respiration allows humans to express certain emotions such laughing, sighing, and sobbing. Furthermore, respiratory air can be used to expel foreign matter from air passages through sneezing and coughing. Although breathing can be voluntarily controlled for short periods of time, the nervous system usually controls it automatically to meet the body’s demand without conscious effort. The respiratory center consists of a widely dispersed group of neurons that send nerve impulses to respiratory muscles. This area can be divided into three areas: the medullary rhythmicity area in 9 the medulla oblongata, the pneumotaxic area in the pons, and the apneustic area also in the pons. The medullary rhythmicity area functions to control the basic rhythm of respiration and within this area are inspiratory and expiratory neurons. Nerve impulses generated in the inspiratory area establish the basic rhythm of breathing. While this area is active, it sends out nerve impulses. These nerve impulses eventually reach the diaphragm and external intercostals muscles, causing these muscles to contract, and inhalation occurs. The neurons of the expiratory area remain inactive during quiet breathing but are activated by nerve impulses from the inspiratory area during forceful breathing. Impulses from the expiratory area cause contraction of the abdominal muscles and internal intercostal muscles, which decreases the size of the thoracic cavity and causes forceful exhalation. The pneumotaxic area in the upper pons transmits inhibitory impulses to the inspiratory area and helps coordinate the transition between inhalation and exhalation. The primary effect of these nerve impulses is to help shut off the inspiratory area before the lungs become too full of air. When the pneumotaxic area is more active, breathing rate is much faster. The apneustic area in the lower pons also coordinates the transition between inhalation and exhalation. This area sends stimulatory impulses to the inspiratory area to prolong inhalation. When the pneumotaxic area is active, it overrides the signals from the apneustic area. Certain chemical stimuli determine how quickly and how deeply we breathe. Sensory neurons that are responsive to chemicals are called chemoreceptors. There are chemoreceptors located in two places. Central chemoreceptors are located in the medulla oblongata in the central nervous system and respond to changes in hydrogen or carbon dioxide concentration, or both, in cerebrospinal fluid. Peripheral chemoreceptors are located in the aortic bodies, chemoreceptor bundles in the wall of the arch of the aorta, and in the carotid bodies, which are oval nodules in the wall the left and right common carotid arteries where they divide into the internal and external carotid arteries. These chemoreceptors are part of the peripheral nervous system and are sensitive to changes in oxygen, hydrogen, and carbon dioxide in the blood. If there is even a slight increase in carbon dioxide, central and peripheral chemoreceptors are stimulated. These in turn send nerve impulses to the brain that cause the inspiratory area to become highly active, and the respiration rate increases. This allows more carbon dioxide to be expelled by the body until its levels are lowered to normal. The Inflation Reflex Located in the walls of bronchi and bronchioles are stretch-sensitive receptors called baroreceptors or stretch receptors. Nerve impulses are sent to the inspiratory and apneustic areas when these receptors become stretched during overinflation. In response, these areas 10 are inhibited and expiration begins. The lungs deflate as air leaves the lungs and the stretch receptors are no longer stimulated. This reflex is referred to as the inflation (Hering-Breuer) reflex and is essentially a protective mechanism for prevention of excessive inflation of the lungs. Exercise and the Respiratory System The respiratory and cardiovascular systems make adjustments in response to both duration and intensity of exercise. When muscles contract during exercise, they consume large amounts of oxygen and produce large amounts of carbon dioxide. Oxygen consumption and pulmonary ventilation both increase dramatically during vigorous exercise. An abrupt increase in breathing is caused by neural changes that send excitatory impulses to the inspiratory area in the medulla oblongata. During moderate exercise the gradual increase in ventilation is due to chemical and physical changes in the bloodstream. In addition, the depth of ventilation changes more than the rate of breathing. When exercise is more arduous, the frequency of breathing also increases. At the end of an exercise session, a sudden decrease in breathing is followed a gradual decline to the resting level. Development of the Respiratory System At about four weeks of development, the respiratory system begins as an outgrowth called the respiratory diverticulum. The endoderm lining the respiratory diverticulum eventually becomes the epithelium and glands of the trachea, alveoli, and bronchi. Splanchnic mesoderm surrounds the respiratory diverticulum and eventually becomes the connective tissue, cartilage, and smooth muscle of these structures. As the respiratory diverticulum lengthens, its distal end enlarges to form a tracheal bud, which gives rise to the trachea. Not much later, it divides into bronchial buds, which repeatedly branch out and develop with the bronchi. By the 24 th week, respiratory bronchioles have been formed. During weeks 6 to 16, all main components of the lungs have developed, except those involved in gaseous exchange (respiratory bronchioles, alveoli, and alveolar ducts). Fetuses born at this time cannot survive because respiration is not yet possible at this stage. During the following weeks, lung tissue and alveoli continue to develop. A fetus born near the end of this period can survive if given intensive care but death still frequently occurs due to the immaturity of the respiratory and other systems. Infants born before 26-28 weeks are at high risk for respiratory distress syndrome (RDS), in which the alveoli collapse during exhalation and must be reinflated during inhalation. However, the condition can be treated by forcing air into the lungs via respirator. As the lungs develop, they obtain their pleural sacs. The visceral pleura develops from splanchnic mesoderm and the parietal pleura develops from somatic mesoderm. The space between the layers is the pleural cavity. At birth, most of the lungs of the fetus are filled with 11 fluid. This fluid is a mixture of amniotic fluid, mucus, and surfactant. Once breathing begins at birth, some of the fluid is reabsorbed by blood and lymph capillaries and the rest is expelled through the nose and mouth during delivery. Aging and the Respiratory System The airways and tissues of the respiratory tract become less elastic and more rigid with advancing age. The result is a significant decrease in lung capacity. In fact, in can decrease as much as 35% by age 70. In addition, a decrease in blood level of oxygen, decreased activity of macrophages in alveoli, and diminished action of cilia of the epithelium lining the respiratory tract occur as well. Elderly people are more prone to pulmonary disorders because of all these age-related factors. It can also contribute to an older person’s reduced ability to exercise vigorously. 12