Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
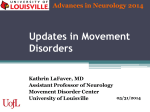
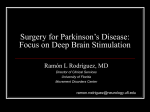
Surgical Treatment of Movement Disorders Stephen Grill, MD, PHD Johns Hopkins University and Parkinson’s and Movement Disorders Center of Maryland Historical Aspects of Surgical Treatment • 1947 – Spiegel & Wycis used stereotactic surgery landmarks within the brain (air encephalograms) and an electrode carrier • 1952 – Cooper inadvertently cut an artery which supplied the globus pallidus and the patient improved. • 1960s – Microelectrode recording was introduced but with the arrival of Sinemet, surgeries lessened Patient Selection For DBS For PD • Secure diagnosis of Parkinson’s Disease: cardinal features • Good response to l-dopa • Either: • Motor complications not controllable pharmacologically including dyskinesias, or • Medically refractory tremor • Exclusions: cognitive impairment/dementia; severe psychiatric illness; other illnesses Surgical Treatment of Movement Disorders • • • • • Historical Aspects Preoperative Issues Surgical Procedure Post-operative care Outcomes New Techniques: Procedure is safer and better • MRI allows better localization • Improved stereotaxis and delivery of the electrode. • Stereotactic techniques involve location of a target in 3-D space by reference to a cartesian coordinate system (3 planes at right angles to each other intersecting at a point) • Advances in understanding of the physiology Patient Selection For Essential Tremor • Medically refractory Essential Tremor – Should have trials of primidone and propranolol • Exclusions: Cognitive impairment; psychiatric disease Patient Selection For Dystonia • Medically refractory generalized dystonia • Cervical dystonia refractory to Botulinum toxin injections • Exclusions: Cognitive impairment; psychiatric disease 1 Evaluation Protocol Evaluation Protocol 35 UPDRS Motor Score 30 25 AIMS 20 Hall Walk (sec) 15 10 Block Sort (sec) 5 0 8:45 10:45 Timed dotting (#) The Team Implanted System Neurosurgeon 2 channels Weight: 67 gm Neuropsychologist PATIENT PRN Movement Disorders Neurologist Psychiatrists Physical therapists Occupational therapists Speech therapists Nurses, NP, PA 1 channel Weight: 45 gm General Neurologist Internist Internist General Neurologist Internist General Neurologist Internist Internist General Neurologist Internist General Neurologist Internist Internist 2 channels Weight: 40 gm Rechargeable Target Sites STN Postoperative Issues STN • Patients usually discharged within 2 days • Initial programming in our center is at 3-4 weeks post-op. Some centers do this earlier Vim Thalamus: Essential Tremor Subthalamic Nucleus: Parkinson’s disease and Dystonia Globus Pallidus: Parkinson’s disease and Dystonia The challenge for neurosurgeon is to get the lead to the desired location. Like “Real Estate”: location, location, location. 2 External Components DBS Programming • Programmable Parameters – – – – Voltage: 0-10.5 V Pulse Duration: 60-450 us Frequency: 30-185 pps Electrode Configuration • Programming Approach – Impedance check – Establish adverse effect threshold: dysarthria, diplopia, muscle contractions, paresthesias, mood changes – Observe for symptom suppression 8840 N’Vision® Clinician Programmer Stimulation Parameters Importance of Lead Location Pulse Width Amplitude Motor Pathways Sensory Pathways Rate Unipolar: Spherical field Bipolar: More focused field STN Properly selected electrode on a properly located DBS™ lead provides optimal therapeutic benefit with minimal stimulation-induced adverse effects. Follow Up Visits and Adjustment of Medications • With STN for PD stimulation there is a 4070% reduction in l-dopa; adjustments of medications are made in parallel with changes in stimulation parameters • Follow up visits are usually at 3 month intervals but may spread out to once a year if the patient has a local neurologist managing their disease - +- Patient Control of Stimulators • With Vim stimulators; patients may turn the stimulator off at night to spare battery life. There may be less development of tolerance • Patients with GPi and STN stimulators leave them on all the time • DBS Patient Programmer allows patients to: • Turn stimulator on and off • Control amplitude, pulse width and rate withing physician-prescribed limits. • Change therapy group that is active • Monitor stimulator battery life 3 “ON” Time Without Dyskinesias Improves from 27% to 74% of a Patient’s Waking Day* Subthalamic Stimulation for IPD 19% 27% 7% 49% 74%* 23% Before Surgery (n=96) 6 Months After Surgery Bilateral STN Activa® Implant (n=91) ‘ON’ with Dyskinesia ‘ON’ without Dyskinesia ‘OFF’ * The Deep-Brain Stimulation for Parkinson’s Disease Study Group. Deep-brain stimulation of the subthalamic nucleus for the pars interna of the globus pallidus in Parkinson’s disease. N Eng J Med. 2001;345:956-63. Bilateral Deep Brain Stimulation vs Best Medical Therapy for Patients With Advanced Parkinson Disease: A Randomized Controlled Trial JAMA. 2009;301(1):63-73. doi:10.1001/jama.2008.929 • Randomized clinical trial of bilateral DBS vs best medical therapy (255 patients) • Subthalamic nucleus (n=60), Globus Pallidus (n=61), best medical therapy (n=134) Off time (hr) On w/o dyskinesias (hr) Working Memory L-dopa* Quality of Life (ADL) Serious Adverse Events • • • #Serious Adverse Event: An undesirable experience associated with use of a medical produce resulting in death or is life threatening or leads to hospitalization or disability or requires treatment to prevent permanent impairment or damage • • • # 49 in DBS group, 19 in controls Most (83%) resolved at 6 months One death due to brain hemorrhage Surgical Site infections: 12 pts Device-related: 8 pts Cardiac complications: 4 pts N Engl J Med 2013: 368:610-622. • 251 PD patients with early motor complications • Randomly assigned to DBS plus medical therapy or medical therapy alone • Primary endpoint: Quality of Life (PDQ-39) significantly improved • UPDRS off medications improved by 17.5 for DBS vs only 1.2 for medical therapy * equivalents Vim Stimulation for Essential Tremor Improvement in Tremor Score After DBS 4 DBS for Dystonia Adverse Events SURGICAL Transient confusion 15.6 % Intracranial Hemorrhage 3.9 % Infection 1.7 % Pulmonary Embolus 0.3 % Miscellaneous 3.3 % DEVICE Electrode/wire replacement 4.4 % Device dysfunction 3.0 % Infection 1.9 % Migration 1.5 % STIMULATION Dysarthria 9.3 % Weight gain 8.4 % Depression 6.8 % Eyelid opening apraxia 3.6 % Stimulation-induced dyskinesia 2.6 % Manic Episodes 1.9 % Miscellaneous motor 4.0 % Miscellaneous psychiatric 3.5 % Kleiner-Fisman G et al (2006) Subthalamic Nucleus Deep Brain Stimulation: Summary and Meta-Analysis of Outcomes. Movement Disorders, 21, Suppl 14, S290-304 Reasons for Inadequate Benefit • • • • • • Incorrect diagnosis Wrong indications Inappropriate expectations Poorly placed leads Device malfunction Sub-optimal programming Conclusions • Deep brain surgeries useful in treating patients with Parkinson’s Disease who are experiencing motor complications including dyskinesias • Deep brain surgeries useful in treating medically refractory Essential Tremor (and other tremors), tremor-predominant Parkinson’s Disease, and Dystonia 5