Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
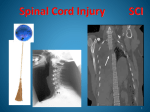
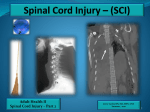
Spinal Cord Injury Management Primary SCI results from cord compression. Secondary injury results from systemic and local vascular insults, which may be a result of hypotension, electrolytes changes, edema, and excitotoxicity. Immobilization Spine immobilization can be uncomfortable, carries potential morbidity of pressure sores and risk of aspiration, and may limit respiratory function; however, it is the usual treatment for all patients with a mechanism of injury that may cause spinal injury. Various methods for complete spine immobilization can be used, but a rigid cervical collar with supportive blocks on a rigid backboard is effective. Hemodynamic Support Systemic hypotension (abnormally low blood pressure), which contributes to secondary SCI, can result from traumarelated hypovolemia (low blood volume) and from neurogenic shock. Treatment typically includes volume resuscitation with fluids or red blood cell transfusion if the patient is anemic. In the subset of patients requiring vasopressors and inotropes (medications to keep up patient’s blood pressure), central venous catheters and invasive monitoring with arterial catheters should be used. Surgical The timing of surgical decompression, reduction of bony structures, and fusion in the treatment of acute SCI remains in debate and left to the experts discretion who are usually neuro surgeons. Pulmonary Support The most common cause of death in patients with SCI is due to pneumonia, pulmonary emboli, and septicemia (severe infection). Patients with high-level cervical injuries (C3–5) may fatigue over the first few hours to days. Early measurements indicating the need for elective endotracheal intubation. Associated Vascular Injury Blunt cervical spinal trauma can result in vertebral artery injury and cause posterior circulation ischemia. Thromboprophylaxis Prophylactic anticoagulation for all patients with acute SCI is a grade 1A recommendation from the American College of Chest Physicians. The recommended anticoagulation is LMWH once primary hemostasis is achieved or a combination of intermittent pneumatic compression and either low-dose unfractionated heparin or LMWH. If anticoagulation is contraindicated, it is recommended that intermittent pneumatic compression with or without graduated compression stockings be used (grade 1C). The period of highest risk for deep vein thrombosis is in the first few months after injury. For this reason, duration of treatment is recommended for at least 6 to 12 weeks. Nutritional Support and Metabolic Changes As described earlier, traumatic injury is associated with a hypermetabolic (increased metabolism), catabolic state with nitrogen loss. Autonomic Dysreflexia Autonomic dysreflexia is a life-threatening hypertensive emergency that typically occurs in patients with motorcomplete SCI above the T6 neurologic level, typically seen in the rehabilitative phase of SCI described as early as 4 days after injury. Noxious stimuli including fecal impaction, bladder distention, or pain to the lower extremities can precipitate it. Recognition of this entity and detection and removal of the inciting noxious stimulus is primary. Prognosis Incomplete injury has a better prognosis than those that are complete.