Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
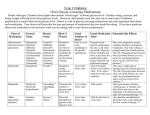
Acute complications of diabetes mellitus: diagnostic criteria and treatment Classification of acute complications of DM Acute complications of DM Hypeglycemic comas Nonketonic hyperglycemichyperosmolar syndrome (NKHHS) Hypoglycemic coma (HC) Diabetic ketoacidisis (DKA) Lactic acidosis (LA) http://www.who.int/mediacentre http://www.who.int/mediacentre http://www.who.int/mediacentre www.undp.org.tt Introduction Occur in both types of DM( type 1 and 2) Mortality rate in NKHHS is raging form 10~50%, depending on underlying disease. Mortality rate in DKA is less than 5%. Thirteen medications and medication classes were implicated, alone or in combination, in hospitalizations for adverse drug events. The four most commonly implicated — warfarin (33.3%), insulins (13.9%), oral antiplatelet agents (13.3%), and oral hypoglycemic agents (10.7%) — accounted for an estimated two thirds of hospitalizations An estimated 2–4% of deaths of people with type 1 diabetes have been attributed to hypoglycemia Pathogenesis of DKA Type 1 diabetes Initiating event Insulin Lypolisis Glucagon Protein catabolism Glycerol FFA´s Amino acids Ketogenesis Hyperglicemia Gluconeogenesis Ketonuria Osmotic diuresis Volumen depletion Dehydration Electrolite depletion Acidosis Ketonemia Precipitating factors: 1) 2) newly diagnosed diabetes (presenting manifestation); inadequate administration of exogenous insulin (inadequate dose, insulin infusion catheter blockage, mechanical failure of insulin infusion pump); 3) increased requirements for insulin caused by the presence of an underlying stressful condition: • an intercurrent infection (pneumonia, cholecyctitis); • a vascular disorder (myocardial infarction, stroke); • an endocrine disorder (hyperthyroidism, pheochromocytoma); • trauma; • pregnancy; • surgery ; • medication (eg, corticosteroids, pentamidine, clozapine) 4) Idiopathic (no identifiable cause) Clinical presentation Diabetic ketosis. It is status which is characterized by increased level of ketones in blood, without clinical signs of dehydration and can be corrected by diet (fat restriction) and regular insulin injection. DKA develops over a period of days or weeks. Clinical presentation nausea, vomiting abdominal pain palpitation Signs and symptoms. Laboratory findings Investigations 1. A presumptive bedside diagnosis is justified if the urine is strongly positive for both glucose and ketones. 2. Measurement of blood ß-hydroxybutyrate (ß OHB) concentration, may not be available in all labs, besides, urine Ketone testing can be misleading due the following reasons: • ◦ The used method does not detect the major ketone body B-hydroxybutyrate. (sodium nitroprusside only measures acetoacetate and acetone). Serum ß-OHB concentrations, may be increased to levels consistent with DKA when a urine ketone test is negative or shows only trace or small ketonuria • ◦ The readings are qualitative depending on color comparisons • ◦ High doses of Vitamin C may cause falsenegative results, while some drugs may, on the other hand, give false-positive results. Diagnostic Criteria PG mg/dl Arterial pH Serum HCO3 Urine Ketones Serum ketones Effective SO (mOsm/kg) Anion gap Mental status Mild >250 Moderate >250 Severe >250 7.25-7.3 15-18 7.0-7.24 10 -15 <7.00 <10 positive positive positive positive positive positive variable variable variable >10 Alert >12 alert/drowsy >12 stupor/coma Treatment The goals of therapy include: 1. Reduction of hyperglycemia 2. Rehydratation 3. Correction of electrolyte imbalance 4. Correction of acid-base imbalance 5. Investigation of precipitating factors, treatment of complications. 6. Frequent patient monitoring Fig. Management of adult patients with DKA. 2003 American Diabetes Association. ©2003 by Canadian Medical Association Chiasson J et al. CMAJ 2003;168:859-866 Nonketotic hyperglycemic-hyperosmolar state (NKHHS or HNS). HNS is a syndrome characterized by impaired consciousness, sometimes accompanied by seizures, extreme dehydration, , and extreme hyperglycemia that is not accompanied by ketoacidosis. The syndrome usually occurs in patients with type II DM, who are treated with a diet or oral hypoglycemic agents, sometimes it is a complication of previously undiagnosed or medically neglected DM (type II). HNC usually develops after a period of symptomatic hyperglycemia in which fluid intake is inadequate to prevent extreme dehydration from the hyperglycemiainduced osmotic diuresis. Predisposing factors 1. 2. 3. • • • 5. 6. 7. HNS seems to occur spontaneously in about 5 – 7 % of patients. Infection (e.g., pneumonia, urinary tract infection, gram-negative sepsis) is underlying frequent precipitating cause. Use of certain drugs has been associated with this condition: steroids increase glucogenesis and antagonize the action of insulin; potassium-wasting diuretics (hypokalemia decreases insulin secretion), e.g., thiazides, furosemide; other drugs, e.g., propranolol, azathioprine, diazoxide. Other medical conditions such as cerebrovascular accident, subdural hematoma, acute pancreatitis, and severe burns have been associated with HNS. Use of concentrated glucose solutions, such as used in peripheral hyperalimentation or renal dialysis, has been associated with HNC. HNS can be induced by peritoneal or hemodialysis, tube feeding. Clinical presentation 1. Polyuria, polydipsia, weight loss, weakness and progressive changes in state of consciousness from mental cloudiness to coma (present in 50 % of patients) occur over a number of days to weeks. 2. Because other underlying conditions (such as cerebrovascular accident and subdural hematoma) can coexist, other causes of coma should be kept in mind, especially in the elderly. 3. Seizures occur in 5 % of patients and may be either focal or generalized. Physical examination 1. Severe dehydration is invariably present. 2. Various neurologic deficits (such as coma, transient hemiparesis, hyperreflexia, and generalized areflexia) are commonly present. Altered states of consciousness from lethargy to coma are observed. 3. Findings associated with coexisting medical problems (e.g., renal disease, cardiovascular disease) may be evident. Laboratory findings Laboratory findings • Diagnosis and treatment of diabetic ketoacidosis and the hyperglycemic hyperosmolar state. CMAJ April 1, 2003 vol. 168 no. 7 859-866 Laboratory findings Treatment This condition is a medical emergency and the patient should be placed in an intensive care unit. Many of the management techniques recommended for a patient with DKA are applicable here as well. The goals of therapy include: • • • • rehydration; reduction of hyperglycemia; electrolytes replacement; investigation of precipitating factors, treatment of complications. Diabetes Care January 2004 vol. 27 no. suppl 1 s94-s102 Lactic acidosis (LA) DM is one of the major causes of LA, a serious condition characterized by excessive accumulation of lactic acid and metabolic acidosis. The hallmark of LA is the presence of tissue hypoxemia, which leads to enhanced anaerobic glycolysis and to increased lactic acid formation. The normal blood lactic acid concentration is 1mmol/l, and the pyruvic to lactic ratio is 10:1. An increase in lactic acid without concomitant rise in pyruvate leads to LA of clinical importance. Pathogenesis Predisposing factors 1. Heart and pulmonary failure (which leads to hypoxia). 2. Usage of bigyanids. 3. Alcohol intoxication. 4. Ketoacidosis (it is important to have a very high index of suspection with respect to presence of LA). Metformin-Associated Lactic Acidosis • Incidence: 0.03 cases/1,000 patient-years • Mortality: about 50% of cases • Sign and symptoms: non-specific (nausea, vomiting, altered consciousness, fatigue, abdominal pain, and thirst) 1.Gowardman JR. Fatal metformin induced lactic acidosis: case report. N Z Med J 1995;108:230-11. 2.Gan SC, Barr J, Arieff AI, Pearl RG. Biguanide-associated lactic acidosis. Case report and review of the literature. Arch Intern Med 1992;152:2333-6. 3.Bailey CJ, Turner RC. Metformin. N Engl J Med 1996;334:574-9. 4.Lee AJ. Metformin in noninsulin-dependent diabetes mellitus. Pharmacotherapy 1996;16:327-51. Clinical presentation Physical examination 1. 2. 3. 4. 5. 6. Acrocyanosis is common. Tachycardia frequently is present, blood pressure is decreased. Poor skin tugor and dry skin may be prominent. Hypothermia is common in LA. Hyperpnea or Kussmaul respiration are present and related to degree of acidosis. Findings associated with coexisting medical problems (e.g., renal disease, cardiovascular disease) may be evident. Laboratory findings 1. 2. 3. Blood glucose level is not high Glucosurea is absent. Blood lactic acid is high. Treatment of LA LA is treated by correcting the underlying cause. Oxygentherapy Metylen blue (50 – 100 ml of 1 % solution i/v droply) Sodium bicarbonate therapy should be used LA can be treated with low dose insulin regimens with 5 % glucose solution infusion. Symptomatic therapy: - Hydrocortisone (250 mg i/v) - Unitiol (5% solution 10 ml i/v (1- 2 ml/10 kg) - α-lipoid acid (tioctic acid) - thiamine (its deficiency may be associated with cardiovascular compromise and lactic acidosis. The response to thiamine repletion (given as 50-100 mg intravenously [IV] followed by 50 mg/d orally [PO] for 1-2 wk) may be dramatic and potentially lifesaving). Sodium bicarbonate • The starting dose of sodium bicarbonate (NaHCO3-) is one third to one half of the calculated extracellular bicarbonate (HCO3-) deficit, as illustrated by the following formula: HCO3 deficit (in mEq) = 0.5 × (Wt in kg) × (Desired HCO3 – Measured HCO3) • Metabolic alkalosis can ensue after bicarbonate administration if the correction is complete rather than partial. This result can be avoided by titration of the bicarbonate dose to modest therapeutic end points (eg, arterial pH of 7.20). • Because of increased CO2 production, sodium bicarbonate may precipitate ventilatory failure and, as such, must be given with caution. Comparison of DCA, HNC and LA. Hypoglycemia It is a syndrome characterized by symptoms of sympathetic nervous system stimulation or central nervous system dysfunction that are provoked by an abnormally low plasma glucose level. Hypoglycemia represents insulin excess and it can occur at any time. Causes: 1. complication of treatment of diabetes mellitus with insulin or oral medications, 2. excessive insulin produced in the body (hyperinsulinemia), 3. inborn error of metabolism, 4. medications and poisons, 5. alcohol, 6. hormone deficiencies, 7. prolonged starvation, 8. alterations of metabolism associated with infection, and organ failure. Risk factors for hypoglycemia in diabetes (ADA, 2009) www.uspharmacist.com: Cryer PE, Axelrod L, Grossman AB, et al. Evaluation and management of adult hypoglycemic disorders: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab. 2009;94:709-728. Patophysiology Clinical presentation 1. adrenergic symptoms (they are attributed to increased sympathetic activity and epinephrine release): - sweating, - nervousness, - faintness, - palpitation - sometimes hunger; 2. cerebral nervous system manifestations: confusion, inappropriate behavior (which can be mistaken for inebriation); visual disturbances, stupor, coma or seizures. (Improvement in the cerebral nervous system manifestations will be with a rise in blood glucose.) A common symptom of hypoglycemia is the early morning headache, which is usually present when the patient awakes. Patients should be familiar with the symptoms of the hypoglycemia but some of them are not heralded by symptoms. Physical examination 1. The skin is cold, moist. 2. Hyperreflexia can be elicited. 3. Hypoglycemic coma is commonly associated with abnormally low body temperature 4. Patient may be unconsciousness. Laboratory findings 1. Low level of blood glucose • It is suggested that persons with diabetes become concerned about the possibility of developing hypoglycemia when the selfmonitored blood glucose concentration is falling rapidly or is no greater than 70 mg/dl (3.9 mmol/liter) (An Endocrine Society Clinical Practice Guideline, 2009) Treatment Insulin–treated patients are advised to carry sugar lumps, candy, or glucose tablets at all time. Asymptomatic or mild-to moderate symptomatic hypoglycemia are effectively self-treated by ingestion of glucose tablets or carbohydrate-containing juice, soft drinks, milk, candy, other snacks, or a meal. Patients have to teach their family members to give such treatment if they suddenly exhibit confusion or inappropriate behavior. • A commonly recommended dose of glucose in adults is 20 g. Clinical improvement should occur in 15–20 min. Treatment • Parenteral treatment is necessary when a hypoglycemic patient is unwilling (because of neuroglycopenia) or unable to take carbohydrate orally. • Glucagon 1.0 mg in adults by an associate of the patient s/c, i/m. Although glucagon can be administered iv by medical personnel, in that setting the standard parenteral therapy is iv glucose. If the patient does not respond to 1 unit of glucagon within 25 minutes, further injections are unlikely to be effective, and are not recommended; Treatment • A standard initial glucose dose is 25 g. The glycemic response to iv glucose is, of course, transient. • an i/v injection of 20 or 100 ml of 40-50 % glucose, followed by a continuous infusion of 5 % glucose (10 % glucose may be needed) until it clearly can be stopped safely; • Food should be provided orally as soon as the patient is able to ingest it safely. • glucocorticoids and adrenaline are helpful as well. • Octreotide has been used to treat sulfonylureainduced hypoglycemia THANK YOU FOR ATTENTION!!!