Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
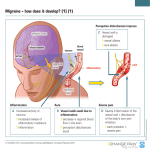
PAIN AND PAIN SYNDROMES Dayna Ryan, PT, DPT Winter 2012 Neuropathic Pain (excluding headache) • What will the patients tell you? • numbness / tingling / pins / shooting / needles / uncomfortable / burning • Definition of pain • “...unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage…” • Neuropathic pain caused by direct lesions or disease affecting somatosensory pathways • e.g. sensory nerves, nerve roots, thalamus, cortex Central Post-Stroke Pain Syndrome • Overview • First described by Déjerine & Roussy in 1906 as “Thalamic Pain Syndrome” • Characterized by gradual onset of neuropathic pain & sensory disturbances after stroke (~50% within 1 month of stroke) • Vascular lesions in somatosensory pathways in the brain, especially spinothalamic cortical tract • Etiology is central sensitization • Signs & Symptoms • Distribution of symptoms • Sensory disturbances • Abnormal sensation • Allodynia: pain evoked by stimuli that is usually not painful (e.g. touch or brush) • Neuropathic pain • A variety of qualities: burning, pricking, aching, lacerating, shooting, squeezing • Spontaneous • Evoked, elicited by mechanical or thermal stimuli • Intense, 3-6 on 10 point scale • Usually a daily pain with varying pain-free intervals lasting a few hours at the most • Diagnosis • History of pain • Imaging confirming a CNS lesion (CT, MRI) • Comprehensive somatosensory test • Rule out other causes • Treatment • Antidepressants (amitriptyline) • Anticonvulsants (gabapentin) • TENS is occasionally helpful Migraine • Overview • Varies in intensity, frequency, duration • Commonly unilateral • Associated with anorexia, nausea & vomiting • Some are preceded by neurologic & mood disturbances • Incidence • 6% of men / 18% of women = 1/3 • 1st attack before age 40 in 90% of patients Lesion involves vasculatures of the brain (blood vessels dilation cause headache) Etiology: unknown • Genetic factors • Environmental factors, e.g. stress, pain • Phases of Migraine • • • • • Prodrome: last hours or days Aura: last < 1 hour prior to pain Headache: last 4 to 72 hours Postdrome: hours or days after pain Classification of Migraine • • Migraine with aura Migraine without aura Visual aura Signs & Symptoms • Prodrome • Mood disturbances, loss or changes in appetite • Aura • Focal neurological symptoms • #1 visual disturbances; #2 paresthesias • Headache • Episodic, commonly unilateral, build up gradually • Dull, throbbing pain • Nausea, vomiting, fatigue, pallor • Photophobia, sonophobia, blurred vision • Aggravated by physical activities • Postdrome • Fatigue, aching, tender head • Increased urination (i.e. diuresis) • Diagnosis • History • Occasionally EEG (focal slowing) • Treatment • Acute • NSAID, narcotics • analgesics (+caffeine) • rest in dark & quiet place • Prophylactic medication • PT • Biofeedback • C-spine manipulation & modalities • Sleep Cluster Headache • Overview • Rare but most painful • Episodic (80% of patients) • Chronic (pain >= 12 months without remission) • Primarily in men age 20 to 50 • Black males • Lesion Site: vasodilation of one external carotid artery • Etiology • Vasodilatation ipsilateral to the pain • ANS dysfunction (activation of trigeminal vascular & parasympathetic systems) • Genetic link Signs & Symptoms • Pain • Sudden, excruciating, mostly unilateral • Orbital & frontotemporal • Boring & non-throbbing • Short duration (15-180 min) • Wake patient up from sleep • Autonomic symptoms • Ipsilateral to the headache • Photophobia • Tearing, nasal congestion • Horner’s syndrome • constricted pupils • droopy eyelid • Diagnosis • History • Treatment • Avoid precipitating factors • alcohol • abrupt changes of sleeping patterns • anger, anxiety • altitude > 5000 feet • laying down • Ergotamine (vasoconstrictor) • Biofeedback & exercise Muscle Tension Headache • Overview • Most common type of headache • “bandlike”, “tightness” head pain • Intermittent, recurrent, or chronic • Etiology • Lesion site: Musculoskeletal disorders at C- spines, TMJ, and atlanto-occipital joint • Previous trauma to neck • Abnormal neck & trunk posture • Stress increases muscle tension • More common in women Signs & Symptoms • Pain • Bilateral forehead, temples, or back of head & neck • Radiates to neck & shoulders • Non-Pulsating, vasoconstricting, moderate intensity • Last <= 7 days • Minimum aggravation by physical activity • Tender scalp, rigidity/spasm of neck • Diagnosis • History, rule out other causes, referred pain • Treatment • NSAID or anagelsics (+ caffeine), TCAs • Biofeedback, massage, heat Trigeminal Neuralgia (CN V) • Etiology • Unknown • Herpes zoster, multiple sclerosis, tumors • Demyelination • pain fibers become hyper-excitable in response to mechanical stimulation (e.g. pressure, touch) • Incidence • More common in women • More common in older adults age 50-70 • Spontaneous remission in some cases • Signs & Symptoms • Sudden onset • “like a lightning bolt inside my head that lasts for seconds to minutes” • Sharp, shooting pain • Most common in 5th CN V2 (maxillary) & V3 (mandibular) branches • Diagnosis • History • No sensory or motor impairment • Imaging studies to rule out other causes • Treatment • Anticonvulsant (Tegretol) • Neurosurgical procedure (rhizotomy) Post-Herpetic Neuralgia: “shingles” • Etiology • Reactivation of varicella zoster virus (chicken pox) causes inflammation in cranial or dorsal roots ganglia • Demyelination & degeneration of affected nerves secondary to inflammation • Onset & Course • Mostly in older adults age 50 to 70 • Immuno-compromised individuals at risk • 1%-2% (rarely) develops motor paralysis • Prognosis is good unless motor neurons or vision is affected • Early Signs & Symptoms • Fever, malaise, GI disturbances • Tingling and pain, followed by rash and blisters along affected dermatomes • Thoracic & trigeminal most commonly affected • Skin lesions last ~ 1 month • Later Signs & Symptoms • Pain • chronic • severe • constant • aching, burning, cutting, stabbing • Diagnosis • Clinical presentation • Treatment • Treat symptoms. No cure. • Corticosteroids (for itching), antiviral (Acyclovir) • Analgesics, Lidocaine patches • Controlled-release oxycodone • Implications for PT • Relaxation • Avoid heat & ultrasound • Get vaccinated yourself! • Don’t touch the skin lesions! (Contagious!) Complex Regional Pain Syndrome • Overview – usually affect arm or leg – uncommon, chronic condition – Classification • CRPS1: Type 1 (“Reflex Sympathetic Dystrophy”) – 90% of cases – Occurs after an illness or injury that did not directly damage the nerves • CRPS2: Type 2 – Occurs after a distinct nerve injury • Etiology: secondary to some type of trauma usually • Lesion site: Overactive sympathetic efferent fibers • General Signs & Symptoms • Intense burning or aching pain • Swelling (cycles with pain) • Trophic skin changes • Thinning • Shininess • Loss of wrinkling • Stages • Stage 1 • Pain increases with stress • Changes in skin & nails • Stage II • Tremor, dystonia, inability to initiate movements • Joint stiffness, swelling • Stage III • Muscle atrophy • Joint contracture • Diagnosis • X-ray, bone scan identifies the bone affected • Thermographic to study skin temperature • Sympathetic ganglion block will abolish pain • Medications • Sympathetic nerve block • Corticosteroids (prednisone) • NSAIDs for pain and inflammation • Antidepressants (amitriptyline) & anticonvulsants (neurotin) • Intrathecal Baclofen to control dystonia • Implanted dorsal column stimulation to reduce pain • PT to increase mobility, TENS, modalities Phantom Limb Pain • Overview – Pain is felt distal to residual limb – Pain varies from mild electrical shock, tingling, to intense shooting, throbbing or burning – Present in 75% of amputee, persistent & chronic in ~ 5% of amputees – Prognosis is poor with pain > 6 months • Etiology – Overactive central pain pathways due to loss of peripheral sensory inputs – Maladapted cerebral cortex remapping • Treatment • Anesthesia to brachial plexus fibers • Pain medications • Surgery to remove scar entangling a nerve • Mirror Therapy • Virtual Reality • Biofeedback, relaxation • Heat & massage (PT) • TENS (PT)