Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
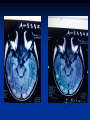
Tacrolimus-associated posterior reversible encephalopathy syndrome (PRES) in a bone marrow transplant recipient. G. Ntetskas, E. Spanou, V. Papastergiou, M. Stampori, E. Asonitis, E. Anastasiou, F. Alourda,F. Lambrianou, A. Kotis, S. Karatapanis First Department of Internal Medicine, General Hospital of Rhodes, Posterior Reversible Encephalopathy Syndrome (PRES) Clinicoradiological entity Described by Hinchey et al in 1996 Reversible ischemia of the posterior cerebral vasculature Vasogenic edema (parietal-occipital region) Posterior Reversible Encephalopathy Syndrome (PRES) Neurologic features (consciousness impairment, seizures, headaches, visual abnormalities, nausea/vomit, focal neurological signs) Cerebral imaging abnormalities (often symmetric and predominate in the posterior white matter) Posterior Reversible Encephalopathy Syndrome (PRES) Unknown incidence (rare) Most commonly occur in middle-aged adults (39-47 years) Female predominance Associated comorbidities: Hypertension, bone marrow or solid organ transplantation, chronic renal failure, medications, eclampsia. Usually reversible once the cause is removed Need for mechanical ventilation in 35-40% Permanent neurological impairment or death (up to 15%) may occur in a minority of patients Posterior Reversible Encephalopathy Syndrome (PRES) Pathogenesis is unknown Hypertensive PRES: failure of cerebrovascular autoregulation Non-hypertensive PRES: autoimmune or immune response to various stimuli There are no consensual guidelines to validate diagnosis of PRES Case presentation Female 55 years old History of acute myeloid leukemia treated with bone marrow transplantation 12 months ago Since the last 3 months the patient was under Tacrolimus to prevent graft-vs-host disease. Case presentation Presentation to the ER Altered mental status Confused Disoriented GCS score was 10 (eye response to verbal command, incomprehensive speech, purposeful movements to painful stimulus) Case presentation History obtained from the patient’s husband revealed no recent infection, fever, weight loss or trauma. She was moving her extremities equally, bilaterally. Reflexes were brisk throughout with equivocal plantar response Rest of the neurological exam was limited as the patient was not following commands consistently. Case presentations blood pressure was 220/110 mmHg Blood count, routine biochemical tests and ABG were normal No ECG abnormalities Chest X-Ray was normal D.D. Cerebrovascular accident Seizures Complicated PRES migraine MRI BRAIN Bilateral regions of edema (hyperintensities in FLAIR and T2-weighted sequences) located in the white matter and predominating in the posterior part of the parietal and occipital lobes. Management Supportive care Discontinuation of Tacrolimus Nicardipine/labetolol to control BP (rapid BP reduction may aggravate cerebral perfusion and promote ischemia!!!) Outcome Gradual resolution of PRES symptoms Follow-up MRI, 1 mo after discharge, demonstrated normal findings Conclusions PRES should be considered in the differential diagnosis of patients with a history of bone marrow transplantation and/or under tacrolimus-based immunosuppresion. Toxic agents in association with PRES Legriel S et al., Annual Update in Intensive Care and Emergency Medicine, 2011 Thank you!!!