Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
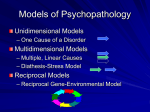
Discussion Serotonin Syndrome Serotonin • 5-hydroxytryptamine or 5-HT • Discovered in 1948 • Major role in multiple clinical states. Lack of serotonin linked to: - Aggression, pain, sleep, appetite - Anxiety, depression - Migraine, emesis Serotonin Metabolism • Dietary tryptophan - Series of reactions to convert to 5-HT • Specific transport system into cells • Degradation - Mainly by monoamine oxidase (MAO) - Excreted as 5-HIAA in urine Serotonin Syndrome (SS) • • • • 1st described in 1960 by Oates; diagnostic criteria developed in 1991 by Sternbach With the introduction of numerous serotonergic agents in the past 2 decades, SS has become an important & common adverse drug effect. Occurs in 15% of SSRI overdoses. Potentially life-threatening adverse drug reaction that results from therapeutic drug use, intentional self-poisoning, or inadvertent interactions between drugs • 3 features of SS are critical to an understanding of the disorder: 1. SS is not an idiopathic drug reaction; it is a predictable consequence of excess serotonergic agonism of the CNS and peripheral NS 2. Excess serotonin produces a spectrum of clinical findings 3. Clinical manifestations range from barely perceptible to lethal • Severe SS only occurs with combinations of drugs acting at different sites, most commonly MAOI + SSRI. Less severe toxicity occurs with other combinations, overdoses & single-drug therapy. • Drugs assoc. with Serotonin Toxicity Serotonin Reuptake Inhibitors • Selective serotonin reuptake inhibitors (SSRIs): fluoxetine (prozac), fluvoxamine, paroxetine, citalopram, sertraline (zoloft), escitalopram (lexapro) • Serotonin-Noradrenaline Reuptake Inhibitors (SNRIs): venlafaxine (effexor), desvenlafaxine (pristiq), duloxetine (cymbalta) • Tricyclic Antidepressants (TCAs): imipramine, clopipramine • Opioid analgesics: tramadol, pethidine, fentanyl • St John’s Wort Monoamine oxidase inhibitors • Irreversible MAOi: phenelzine, tranylcypromine • Reversible MAOi: moclobemide • Others: linezolid Serotonin-releasing agents • Amphetamines • MDMA (ecstasy) Miscellaneous • Tryptophan • Lithium • Most SSRIs have half lives of ~ 24 hours. • Fluoxetine has an active metabolite (norfluoxetine). It has a long half life of 16 days. Adverse effects and interactions may persist after tx has stopped. Serotonin Syndrome is a Clinical Diagnosis • Clinical triad of: 1. Neuromuscular abnormalities 2. Autonomic hyperactivity 3. Mental state changes Clinical Features of SS The neuromuscular features of CLONUS and HYPERREFLEXIA are highly diagnostic for SS, and their occurrence in setting of serotonergic drug use establishes the diagnosis. (Boyer and Shannon, 2005) Sternbach criteria Diagnosis likely if ≥ 3 features 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. Mental state changes (confusion, hypomania) Agitation Myoclonus Hyperreflexia Diaphoresis Shivering Tremor Diarrhoea Incoordination Fever Hunter Serotonin Toxicity Criteria more specific Severity of Serotonin Syndrome Mild • Serotonergic features that may or may not concern the patient Moderate • Symptoms cause the patient significant distress and deserve symptomatic treatment Severe Serotonin Toxicity/ Serotonin Crisis • Rapid onset of severe hyperthermia associated with muscle rigidity. • Will progress to multiorgan failure. • It is a medical emergency. • Most commonly as a result of MAOI + SSRI Differentiating between NMS and Serotonin Syndrome NMS is an idiopathic reaction to dopamine antagonists, such as atypical antipsychotics (clozapine, risperidone, olanzapine), anti-emetics (metoclopramide, promethazine), TCAs. Defined by a SLOWER ONSET (days), bradykinesia, “lead-pipe” muscular rigidity, hyperthermia, fluctuating LOC and autonomic instability. Management • Treatment depends on severity • Cessation of serotonergic medication and supportive care for all patients • Drugs that can be used in moderate-severe serotonin toxicity include: - Non-specific serotonin antagonists: Cyproheptadine Methysergide - Beta blockers Propanolol - Neuroleptics Chlorpromazine Mild • Monitor Moderate • When oral tx suitable - Cyproheptadine 8mg stat, then 4mg q4-6hr • When oral tx not suitable or cyproheptamide fails - Chlorpromazine 50mg ini.ivi stat, then up to 50mg PO/imi/ivi q6hr Severe • When symptoms are not progressive & fever < 39OC - Chlorpromazine 50-100 mg imi/ivi stat, then 50-100 mg PO/im/iv q6hr • When symptoms are progressive & fever < 39OC - Chlorpromazine 100-400mg imi/ivi over 1st 2 hours • When symptoms are progressive & fever > 39OC - Barbiturate anaesthesia, muscle relaxation ± active cooling - Chlorpromazine 100-400mmg imi/ivi over 1st 2 hours Posterior Reversible Encephalopathy Syndrome (PRES) • A not always posterior, not always reversible, not always white matter syndrome… • A clinicoradiological entity • 1st well described in 1996 by Hinchey et al. • Also known as Reversible Posterior Leukoencephalopathy Syndrome (RPLS) Reversible Posterior Cerebral Oedema Syndrome Reversible Occipital Parietal Encephalopathy Hyperperfusion Encephalopathy Brain Capillary Leak Syndrome • PRES is the current accepted term, despite the mortality rate of up to 15% (Lee et al., 2008) • “Potentially” Reversible Encephalopathy Syndrome Epidemiology • Global incidence of PRES is unknown • Only epidemiological data come from retrospective studies of patients between 1998-2008 • Occurs at any age (2 - 90 years) • Preferentially affects patients with severe co-morbidities • More common in women, even when eclampsia excluded • Risk Factors: 1. Hypertensive disorders 2. Renal disease 3. Immunosuppressive therapies Conditions Most Commonly Associated with PRES • Immunosuppressive/cytotoxic drugs (e.g. cyclosporin, antineoplastic drugs, interferon-α, HAART) • Hypertensive encephalopathy • Pre-eclampsia/Eclampsia/HELLP syndrome • Autoimmune diseases (e.g. SLE, scleroderma) • • • • • • • • • • Acute or chronic renal diseases (e.g. glomerulonephritis, dialysis disequilibrium syndrome) TTP/HUS High-dose steroid therapy Liver failure/transplantation Endocrine dysfunctions Hypercalcaemia/hyperparathyroidism Bone marrow transplantation Massive blood transfusion/erythropoietin therapy Porphyria Other causes (e.g. IVIg, stimulants abuse) (Servillo et al., 2007) Pathophysiology of PRES is unclear 2 conflicting hypotheses 1. Autoregulatory Failure with Hyperperfusion 2. Endothelial Dysfunction with Hypoperfusion Both result in cerebral blood perfusion abnormalities causing BBB dysfunction & cerebral vasogenic oedema 1. Autoregulatory Failure with Hyperperfusion • Normal autoregulation maintains constant cerebral blood flow over range of systemic BP (MAP 60-120 mmHg; ~ 220/110 mmHg) by arteriolar constriction & dilatation. • As upper limits of cerebral autoregulation are surpassed (e.g hypertensive encephalopathy, with MAP > 170 mmHg), focal dilatations of cerebral vessels occur. • Regions of both vasoconstriction and vasodilation (“sausage-string pattern”) develop, especially in arterial boundary zones, resulting in ↑ cerebral blood flow • Cerebral hyperperfusion leads to release of vasodilators (NO, prostacyclin) & inflammatory cytokines (IL-6, NF-κB) leading to disruption of BBB extravasation of fluid into the brain parenchyma (cerebral vasogenic oedema) (Schwartz, Jones & Kalina, 1992) • Brain biopsy findings have been reported that show oedematous white matter with no evidence of vessel wall damage or infarction (Schiff & Lopes, 2005) • Chronic Hypertension – Vascular changes “reset” range of autoregulation – In setting of longstanding HTN or even in patients with normal BP – they may only require small acute increases in MAP of 50 mmHg (~ 160/100 mmHg) to trigger severe vasoconstriction &, consequently, PRES. 2. Endothelial Dysfunction with Hypoperfusion • Not all patients with PRES have hypertension. • In pts with PRES & normal BP, cytotoxicity is thought to be the main mechanism underlying brain oedema. • Associated conditions include: cytotoxic therapies (e.g. cyclosporin, tacrolimus), preeclampsia/eclampsia, infection/sepsis/shock, autoimmune disease • Cytotoxic therapies – Exposure to toxic agents is the most common condition associated with PRES. – May have direct toxicity on vascular endothelium leading to capillary leakage & BBB breakdown which triggers vasogenic oedema (Hinchey et al., 1996) – May occur with nontoxic levels of these drugs • Pre-eclampsia • An alternate theory for PRES suggests spasm of cerebral arteries in response to acute hypertension resulting in ↓ cerebral blood flow, ischaemia & cytotoxic oedema, esp. in the border zones between arterial territories (“watershed zones”) PRES preferentially affects white matter & posterior circulation • The cortex, structurally more tightly packed than white matter, resists accumulation of oedema, hence predilection of abnormalities in white matter • Primary involvement of posterior brain regions not well understood. • One explanation is the lower sympathetic innervation of posterior cerebral arterial circulation than in the internal carotid artery territory, with consequent ↓ autoregulation of already impaired cerebral areas (Kaplan, 2002) Clinical Features of PRES • • • • • • • Acute encephalopathy Acute hypertension (median MAP 122 mmHg) Seizures/Status epilepticus Headaches Visual impairment Nausea/vomiting Focal neurological signs • Patients have an acute/subacute neurological presentation, often heralded by convulsions. May begin focally, but usually become generalised. • Tendon reflexes are usually brisk and some patients may also present with weakness and incoordination of the limbs. (Hinchey et al., 1996) Radiographic Findings • CT can be used preliminarily to detect hypodense lesions of posterior encephalopathy, but MRI is the gold standard. • CT may not be sensitive enough to provide differentiation between vasogenic oedema (assoc. with cerebrovascular dysfunction) and cytotoxic oedema (assoc. with neoplasm, SOL, or infarct). • Diffusion-weighted MRI (DWI) is the modality that best differentiates between vasogenic and cytotoxic oedema – and is considered to be the gold standard. • PRES lesions are isodense on DWI, hyperintense on FLAIR, hyperintense on T2 images, iso- or hypointense on T1 views, and hyperintense on apparent diffusion coefficient (ADC) maps. • PRES mainly involves the parietal-occipital lobes; however, cerebellar hemispheres, basal ganglia, frontal lobes, and brainstem are also often involved (Servillo et al., 2007). • A repeat MRI with normal results obtained after symptoms resolved confirms the diagnosis of PRES. • Note: clinical outcome is generally excellent, with recovery within a few days-weeks, while the MRI abnormalities resolve much more slowly • The anatomical extent of MRI findings have been shown to correlate with patient outcome (esp. if brainstem involvement). • More severe PRES can show evolution to infarct or haemorrhage. Neuroimaging in PRES showing bilateral parieto-occipital involvement CT FLAIR DWI Resolution after 2 weeks Differential Diagnoses – Stroke – Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy (CADASIL) – Cerebral Venous Sinus Thrombosis – Toxic or metabolic encephalopathy – Demyelinating disorders – Vasculitis • Bilateral posterior cerebral artery infarction (“top of the Basilar syndrome”) – Encephalitis – Creutzfeld-Jacob disease Management principles • Patients generally require ICU admission for systemic support. • Treat the underlying cause – lowering BP, reducing/stopping causative immunosuppressive medication, delivery/caesarean in pregnant woman. • Persistence of the cause carries a risk of ischaemia, bleeding & death. • Control seizures with anticonvulsants or MgSO4 in pregnant patients (No indication pts at long-term risk for seizure recurrence or epilepsy (although long term studies are lacking)) • Manage hypertension with iv antihypertensives, aiming for MAP 105-125 mmHg. • Hypoglycaemia should be monitored and corrected. Management of Hypertension • The aim is to ↓ MAP by 20 – 25 % within the 1st 2 hours; and to bring the BP down to 160/100 mmHg within the 1st 6 hours. Lower diastolic BP to 100-105 mmHg within 2-6 hrs. • Max initial fall of BP should not exceed 25% of presenting value • More aggressive tx may reduce beyond autoregulatory range and possibly lead to ischaemic event • Nicardipine (5-15 mg/h) or labetalol (2-3 mg/min) are 1st line agents. • ACE-I should be avoided in obstetric patients due to their toxic effect on the foetal kidney. • Nitroglycerin should be used with caution as it has been reported to aggravate oedema, probably by further enhancing cerebral vasodilatation. Determinants of Recovery from severe PRES • Few outcome data available about PRES • In retrospective cohort study in Europe involving 24 ICUs over a 9 year period, 70 patients with a diagnosis of PRES were evaluated. • By day 90 after admission for severe PRES, 44% of survivors had severe functional impairments. • Highest glycaemia on day 1 and time to causativefactor control were strong early predictors of outcomes. (Legriel et al., 2012) References • • • • • • • • • Boyer EW, Shannon M (2005) The Serotonin Syndrome N Engl J Med 352: 11121120 Hinchey J, Chaves C, Appignani B, Breen J, Pao L, Wang A, Pessin M, Lamy C, Mas JLM, Caplan LR (1996) A reversible posterior encephalopathy syndrome N Engl J Med 334: 494-500 Kaplan PW (2002) Neurologic aspects of eclampsia. In: Hainline B and Devinsky O (eds) Neurological complication of pregnancy, 2nd ed. Lippincott Williams & Williams, pp 87-101 Lee VH, Wijdicks EF, Manno EM, Rabinstein AA (2008) Clinical spectrum of reversible posterior leukoencephalopathy syndrome. Arch Neurol 65: 205-210 Legriel et al. (2012) Determinants of Recovery from severe posterior reversible encephalopathy syndrome PLOS one org Schiff D, Lopes MB (2005) Neuropathological correlates of reversible posterior leukoencephalopathy Neurocrit Care 2: 303-305 Schwartz RB, Jones KM, Kalina P (1992) Hypertensive encephalopathy: findings on CT, MR imaging, and SPECT in 14 cases. AJR Am J Roentgenol 159: 379-383 Servillo G, Bifulco F, Piazza O, Striano P, Tortora F, Striano S, Tufano R (2007) Posterior reversible encephalopathy syndrome in intensive care medicine Intens Care Med 33: 230-236