Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Anaphylaxis
Massive
allergic reaction
Always call 911
Causes of Anaphylactic Shock
– Medications
– Foods and food additives
• Monosodium glutamate, peanuts
– Plant pollens
– Bee stings
– Radiographic dyes
Characteristics of Anaphylaxis
– Usually comes on in minutes / Peaks in 1530 minutes
– Sensation of warmth
– Intense itching of soles of feet and palms
of hands
– Breathing difficulties
– Tightness and swelling in throat
– Coughing, sneezing, wheezing
– Tightness in chest
Characteristics of Anaphylaxis #2
– Increased pulse rate
– Swollen face, tongue, mouth
– Nausea and vomiting
– Dizziness
– Blue around lips and mouth
Anaphylaxis: What To Do
– Check ABC’s
• Use ice pack on bee sting
– Inject epinephrine (dilates bronchioles)
• (hopefully victim will have some)
• Inject in outside part of thigh, hold for 10
seconds
• May need to repeat
– Get help immediately - 911(float trip)
– Benedryl – too slow for major emergency,
but worth a try
PATOGENESI DELLO SHOCK ANAFILATTICO
S.N.C.
Allergene
IgE
M.C.
APP. RENALE
CIRCOLO
ISTAMINA
LEUCOTRIENI
CHININE
APP. CARDIOVASCOLARE
APP. INTESTINALE
APP. POLMONARE
A. TURSI
Chemical Structure of Histamine and Representative H1-Receptor-Antagonist Drugs
Simons, F. E. R. et al. N Engl J Med 1994;330:1663-1670
Dealing With Anaphylaxis
Give EPIPEN.
Remove grey cap from end.
Press EPIPEN firmly into side of thigh until a
click is heard, then hold in place and count to
10.
Administer Benadryl (for breathing difficulties).
Call 911 (emergency) to transport to hospital.
Notify parents immediately after emergency call.
Frequency of symptoms in
Anaphylaxis
Urticaria/angioedema
Upper airway edema
Dyspnea or wheeze
Flush
Dizziness,
hypotension, syncope
Gastrointestinal sx
Rhinitis
88%
56%
47%
46%
33%
30%
16%
Formulations and Dosages of Representative H1-Receptor Antagonists
Simons, F. E. R. et al. N Engl J Med 1994;330:1663-1670
Anaphylaxis
• Onset of symptoms of anaphylaxis: usually
in 5 to 30 minutes; can be hours later
• A more prolonged latent period has been
thought to be associated with a more benign
course.
• Mortality: due to respiratory events (70%),
cardiovascular events (24%)
Prevention of anaphylaxis
• Avoid the responsible allergen (e.g. food,
drug, latex, etc.).
• Keep an adrenaline kit (e.g. Epipen) and
Benadryl on hand at all times.
• Medic Alert bracelets should be worn.
• Venom immunotherapy is highly effective
in protecting insect-allergic individuals.
Treatment of anaphylaxis
• EPINEPHRINE (1:1000) SC or IM
- 0.01 mg/kg (maximal dose 0.3-0.5 ml)
- administer in a proximal extremity
- may repeat every 10-15 min, p.r.n.
• EPINEPHRINE intravenously (IV)
- used for anaphylactic shock not
responding to therapy
- monitor for cardiac arrhythmias
• EPINEPHRINE via endotracheal tube
Treatment of anaphylaxis
•
•
•
•
Place patient in Trendelenburg position.
Establish and maintain airway.
Give oxygen via nasal cannula as needed.
Place a tourniquet above the reaction site
(insect sting or injection site).
• Epinephrine (1:1000) 0.1-0.3 ml at the site
of antigen injection
• Start IV with normal saline.
Treatment of anaphylaxis
• Benadryl (diphenhydramine)
- H1 antagonist
• Tagamet (cimetidine)
- H2 antagonist
• Corticosteroid therapy: hydrocortisone IV
or prednisone po
Treatment of anaphylaxis
• Biphasic courses in some cases of
anaphylaxis:
- Recurrence of symptoms: 1-8 hrs later
- In those with severe anaphylaxis,
observe for 6 hours or longer.
- In milder cases, treat with prednisone;
Benadryl every 4 to 6 hours; advise to
return immediately for recurrent symptoms
Treatment of Anaphylaxis in Beta
Blocked Patients
• Give epinephrine initially.
• If patient does not respond to epinephrine
and other usual therapy:
- Isoproterenol (a pure beta-agonist)
1 mg in 500 ml D5W starting at
0.1 mcg/kg/min
- Glucagon 1 mg IV over 2 minutes
Use of epinephrine in
Food Allergy
• Epinephrine should be used immediately
after accidental ingestion of foods that have
caused anaphylactic reactions in the past.
• An individual who is allergic to peanut,
nuts**, shellfish, and fish should
immediately take epinephrine if they
consume one of these foods.
• A mild allergic reaction to other foods (e.g.
minor hives,vomiting) may be treated with
an antihistamine
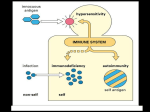
Immediate Hypersensitivity
• Acute (type I) hypersensitivities begin in
seconds after contact with allergen
• Anaphylaxis – initial allergen contact is
asymptomatic but sensitizes the person
– Subsequent exposures to allergen cause:
• Release of histamine and inflammatory chemicals
• Systemic or local responses
Immediate Hypersensitivity
– The mechanism involves IL-4 secreted by T
cells
– IL-4 stimulates B cells to produce IgE
– IgE binds to mast cells and basophils causing
them to degranulate, resulting in a flood of
histamine release and inducing the
inflammatory response
Acute Allergic Response
Figure 21.20
Anaphylaxis
• Reactions include runny nose, itching
reddened skin, and watery eyes
• If allergen is inhaled, asthmatic symptoms
appear – constriction of bronchioles and
restricted airflow
• If allergen is ingested, cramping, vomiting,
or diarrhea occur
• Antihistamines counteract these effects
Anaphylactic Shock
• Response to allergen that directly enters the
blood (e.g., insect bite, injection)
• Basophils and mast cells are enlisted throughout
the body
• Systemic histamine releases may result in:
– Constriction of bronchioles
– Sudden vasodilation and fluid loss from the
bloodstream
– Hypotensive shock and death
• Treatment – epinephrine is the drug of choice
Definizione di anafilassi (AAAAI)
• Sindrome multisistemica, dovuta al rilascio di
mediatori da basofili e mast-cell
• Inizio acuto
• Gravità variabile da lieve e autolimitantesi a
mortale
Università di Torino - Divisione Universitaria di Allergologia e Immunologia Clinica - Ospedale Mauriziano Umberto I
Sintomi e segni dell’anafilassi
• sensazione di calore
• flushing e prurito
• orticaria e
angioedema
• sensazione di stare
per svenire
• tosse, dispnea,
respiro sibilante
• dolore addominale,
nausea, vomito,
diarrea
• sensazione di vie
aeree chiuse e
dispnea
• incapacità a
deglutire, parlare
• disorientamento
• sudorazione
• aritmia cardiaca,
sincope, shock
• incontinenza
Frequenza delle manifestazioni cliniche
nell’anafilassi
• Segni e sintomi cutanei:
• Segni e sintomi respiratori:
100
%
75
%
• Segni e sintomi cardiovascolari: 30-50 %
• Segni e sintomi gastrointestinali: 25
%
Patogenesi dell’anafilassi
Classificazione fisiopatologica dell’anafilassi
• IgE mediata: cibi, farmaci, insetti
• Rilascio diretto dei mediatori da basofili/mastcell
(farmaci, esercizio, freddo, idiopatica)
• Alterazione del metabolismo ac arachidonico
(aspirina, FANS)
• Immunoaggregati (gammaglobuline, IgG antiIgA, destrano, albumina)
• Reazioni trasfusionali
• Attivazione del complemento non IC mediata
(mdc, protamina, membrana dialitica)
Università di Torino - Divisione Universitaria di Allergologia e Immunologia Clinica - Ospedale Mauriziano Umberto I
Diagnosi differenziale dell’anafilassi:
sindrome vaso-vagale
•
•
•
•
•
Pallore vs flush, orticaria, angioedema, prurito
Sudorazione
Bradicardia vs tachicardia (eccezioni)
Nausea e vomito +++
Circostanze (prelievo, stazione eretta prolungata
in ambiente affollato e caldo, secondaria a
dolore fisico etc)
Università di Torino - Divisione Universitaria di Allergologia e Immunologia Clinica - Ospedale Mauriziano Umberto I
Terapia immediata dell’anafilassi
• Valutazione segni vitali
• Adrenalina 0.3-0.5 ml i.m. ogni 10-20 min
(nei bambini 0.1-0.3 ml , o 0.01 mcg/Kg)
• Posizione supina, gambe sollevate
• O2
Università di Torino - Divisione Universitaria di Allergologia e Immunologia Clinica - Ospedale Mauriziano Umberto I
Terapia dell’anafilassi
(in base alla valutazione clinica)
• Liquidi e.v. : fisiologica 1 l nei primi 20 min
• Antistaminici (anti-H1 + anti-H2)
• Salbutamolo 2.5/5 mg in aerosol ogni 20-30 min (se
broncospasmo ++)
• Metilprednisolone 50 mg ogni 6 ore (4 dosi)
• SE IPOTENSIONE GRAVE: adrenalina e.v. 10 ml della
sol. 1:100.000 (10 mcg/ml) in 5-10 min oppure 1-2
ml ogni 5-20 min della sol. 1: 10.000 (100 mcg/ml)
Università di Torino - Divisione Universitaria di Allergologia e Immunologia Clinica - Ospedale Mauriziano Umberto I
Symptoms-Food Allergy*
•
•
•
•
•
•
•
•
•
•
Nausea
Diarrhea
Abdominal cramps
Pruritic rashes
Angioedema
Asthma/rhinitis
Vomiting
Hives
Laryngeal edema
Anaphylaxis
* Exercise exacerbates symptoms
Definition of Terms
Anaphylactoid events vs. Anaphylaxis
Anaphylaxis: an immediate systemic
reaction caused by rapid, IgE-mediated
immune release of potent mediators from
tissue mast cells and peripheral blood
basophils
Anaphylactoid events: immediate systemic
reactions that mimic anaphylaxis but are not
caused by IgE-mediated immune responses
Anaphylactic Shock
• A type of distributive shock that results from
widespread systemic allergic reaction to an
antigen
• This hypersensitive reaction is LIFE
THREATENING
Pathophysiology Anaphylactic Shock
• Antigen exposure
• body stimulated to produce IgE antibodies
specific to antigen
– drugs, bites, contrast, blood, foods, vaccines
• Reexposure to antigen
– IgE binds to mast cells and basophils
• Anaphylactic response
Anaphylactic Response
• Vasodilatation
• Increased vascular permeability
• Bronchoconstriction
• Increased mucus production
• Increased inflammatory mediators
recruitment to sites of antigen interaction
Clinical Presentation Anaphylactic
Shock
• Almost immediate response to inciting
antigen
• Cutaneous manifestations
– urticaria, erythema, pruritis, angioedema
• Respiratory compromise
– stridor, wheezing, bronchorrhea, resp. distress
• Circulatory collapse
– tachycardia, vasodilation, hypotension
Management Anaphylactic Shock
• Early Recognition, treat aggressively
• AIRWAY SUPPORT
• IV EPINEPHRINE (open airways)
• Antihistamines, diphenhydramine 50 mg IV
• Corticosteroids
• IMMEDIATE WITHDRAWAL OF ANTIGEN
IF POSSIBLE
• PREVENTION
Management Anaphylactic Shock
• Judicious crystalloid administration
• Vasopressors to maintain organ perfusion
• Positive inotropes
• Patient education
•
Table 4 The main important conditions to be distinguished
in a patient presenting with a rash and/or itching Rash+/–
itchItching alone Immune system mediatedImmune
system mediated Anaphylaxis AnaphylaxisAnaphylactoid
reactionAnaphylactoid reactionAllergic reaction—
localSystemicUrticaria ("hives") and/or angioedema
Idiopathic thrombocytopaenicSystemic upset (for example,
uraemia, cholestasis, blood disorders)purpura
(ITP)OtherInfectiveSenile itchBacterialSolid
tumours Meningococcal
septicaemiaHIV Cellulitis Impetigo Scarlet
feverViral Varicella zoster
Primary infection
(chickenpox)
Reactivation (herpes zoster or
"shingles") Measles Rubella (German measles) Nonspecific viral rashOther conditions Henoch Schonlein
purpura Psoriasis Eczema
Heat
Redness
Swelling
Pain
Loss of Function
Nature Reviews/Immunology
Management of Allergic
Reactions
Generalized anaphylaxis involves all of
the previously mentioned systems
When hypotension occurs, it is termed
Anaphylactic Shock
Affected Area Manifestation
Skin
Flare
Urticaria-Wheal &
pruritis, angioedema,
erythema
Respiratory
Dyspnea,wheezing,flushing,
cyanosis,perspiration,tachycardia,
Affected Area Manifestation
Gastrointestinal
Abdominal cramps,
nausea, vomiting,
diarrhea,
incontinence
Cardiovascular
headedness,
Pallor, lightpalpitations,
tachycardia,
Sequence of Reaction
1. Skin reaction
2. Smooth muscle spasm
(GI, GU, and bronchial)
3. Respiratory distress
4. Cardiovascular collapse
Type of Reaction
Quick Onset==> Rapid Progression==>
Intense Reaction
Delayed Onset==> Slow
Progression==>
Less Severe Reaction
Drugs Used in Allergic Reactions
Epinephrine
Has Alpha and Beta adrenergic effects
Acts as a physiologic antagonist to the
events that occur during an allergic
reaction
Epinephrine
Actions Include
Bronchodilation
Increased heart rate
Arterial constriction
Cutaneous, mucosal, and splanchnic
vasoconstriction
Reverses rhinitis and urticaria
Epinephrine
Risks of repeated use:
Excessive elevation of blood pressure
CVA
Cardiac rhythm abnormalities
Antihistamine
Benadryl (chlorpheniramine) most often
used
H-1 blocker
Inhibits action of histamine released
during reaction to allergen
Corticosteroids
Hydrocortisone used most often
Stablilizes cell membranes against
actions of histamines, bradykinins, and
prostaglandins
Supplements adrenal steroid output
during stress
Treatment of
Immediate Skin Reactions
Epinephrine 0.3 mg IM or SC
(0.3ml of a 1:1000 Solution)
Antihistamine
Diphenhydramine (Benadryl) 50 mg
IM
Gell and Coomb’s reactions
Type I- Immediate Hypersensitivity
– Immediate
– Allergen binds 2 molecules of IgE
– Intracellular degranulation and immediate
release of products
– Ex. Allergic rhinitis, anaphylactic shock,
asthma
27.
Type I
Hypersensi
tivity
Type I
Hypers
ensitivi
ty
Reactio
n
28.
3 R’s for treating
anaphylaxis
recognize symptoms
react quickly
review what happened
to try and prevent
reoccurrance
Anaphylaxis
3 Rs of An Allergic Emergency
Plan
• Recognize symptoms early
• React quickly
• Review what caused the reaction
Anaphylaxis Management
An emergency plan of action should
include:
• What symptoms to look for
• What medications to use
• Medication dosage instructions
• Where will medications be kept
• What others should do
• Allergy emergency practice drills
Key Steps in Anaphylaxis
Management
• Recognize students
• Know what symptoms to look for
• Administer epinephrine quickly
• Transport to hospital after EpiPen®
use, then call parents
How to Use EpiPen®
How to Hold
• Form a fist around the
center of the unit
• Pull off gray activation cap
How to Use
• Hold black tip near outer thigh
(always apply to thigh)
Count to 10
• Swing and jab into outer thigh.
Hold in place and count to 10
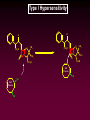
Type I Hypersensitivity: Sensitization
BB7
7
B-cell
MHCII-Peptide
CD28
MHCII
Peptide CD3
TH-2
TCR
CD4
Memory
B-Cell
Plasmacyte
IgE Production
Type I Hypersensitivity: Sensitization
Plasmacyte
IgE Binding
to Mast Cell
Fc/IgE
Receptor
Sensitized
Mast Cell
IgE Production
Sensitized Mast Cell
Type I Hypersensitivity: Effector
Calcium
Influx
Allergen
Sensitized
Mast Cell
Eosinophil &
Neutrophil Attraction
Degranulation
(enzymes, histamine)
Histamine
Cytokines
Lipid Mediators
Type I Hypersensitivity
Type I Hypersensitivity
Type I Hypersensitivity
Preformed Mediators:
stored in granules in mast cells
1) Histamine - most important mediator in humans, although a similar
function is performed by serotonin in other species, e.g.,rodents
most of the characteristics of anaphylaxis can be mimicked in humans by injection
of histamine alone
present in granules at very high concentrations as an electrostatic complex with
heparin. After fusion of the granules histamine is released from the heparin complex
by ion-exchange effects
stimulates contraction in most smooth muscle, vasodilation and permeability in
post-capillary venules, drop in blood pressure
Type I Hypersensitivity
Preformed Mediators:
2) Eosinophil chemotactic factor - attracts and prevents further migration of
eosinophils and neutrophils
3) Neutrophil chemotactic factor - attracts and prevents further migration of
neutrophils
4) Degradative enzymes including: Arylsulfatase - inactivates leukotrienes chymase degrades proteins N-acetylglucosaminidase - degrades heparin
Type I Hypersensitivity
2. Causes and Results
for humans can result from, bee or wasp sting, seafood, nuts.
can also result from cross linking of drug to self protein (i.e., penicillin,
insulin)
• can result in asthma, hayfever, systemic or localized anaphylaxis
Type I Hypersensitivity
Lipid Mediators:
formed and secreted after mast cells are activated
1) Leukotrienes B4, C4, D4:
formerly known as SRS-A, slow reacting substance of anaphylaxis
arachidonic acid metabolites structurally related to prostaglandins
contracts bronchioles and increases capillary permeability
2) Platelet-activating Factor (PAF):
synthesized from phospholipids in the cell membranes
active at l0l0 M
potent hypotensive agent
most potent bronchorestricting agent in asthma and allergic rhinitis (hay fever)
aggregates and lyses platelets releasing serotonin and other mediators
promotes eosinophil infiltration
PAF antagonists represent an active area of research, particularly for drugs to
prevent abnormalities in reproduction
3) Prostaglandin D2 and other prostaglandins
Type I Hypersensitivity
Cytokines:
stimulates production of lymphokines (IL-3, IL-4, IL-5, IL-6, GM-CS~),
which stimulate production of leukocytes, more mast cells - stimulates
production of bradykiniin, which causes vasodilation, hypotension
Type I Hypersensitivity
O
O
S
CO2 H
N
O
CH 3
CH 3
S
CO2 H
S
NH
O
Self
Protein
SH
Self
Protein
SH
CH 3
CO 2H
CO 2H
SH
CH 3
Type I Hypersensitivity
Systemic Anaphylaxis:
most severe and life-threatening type of allergic response
characteristics:
- generalized flush, palpitations, dizziness, apprehension, urticaria,
angioedema and abdominal cramps
- may proceed to dyspnea, seizures, cyanosis, shock, and/or death
- begins 3 to 4 min after administration
causes:
-xenogenic sera, allergenic extracts, dextrans, therapeutic enzymes,
polypeptide hormones, penicillins and cephalosporins.
localized anaphylaxis affects only certain vasodilation smooth muscles
most common is hayfever (allergic rhinitis) and asthma (localized brochial
constriction)
Skin grids are useful for detecting if a person will respond to an allergen;
Risk of sensitizing the individual as well as leading to shock.
Type I Hypersensitivity
3. Drugs that Affect TYPE I
-Antihistamines
-Cromolyn Sodium
-Theophylline
-Epinephrine
-Cortisone
Block Hl&H2 receptors
Blocks Calcium influx
Prolongs cAMP levels (inhibits phosphodiesterases).
Degranulation is increased by lowering levels of cAMP
Stimulates cAMP production through b-adrenergic receptor
Blocks histimine production, stimulates mast cell cAMP
production
Type I Hypersensitivity
Histamine Causes a Wide Array of Effects
smooth muscle cells - Constriction
small blood vessels - Vasodilation
mucous glands - Mucous secretion
blood platelets
sensory nerve endings
Histamine Receptors
(H1 and H2 receptors
Type I Hypersensitivity
4. Therapeutic Immediate-Hypersensitivity Antigens
Therapy for allergies based on hyposensitivity
Typical therapy depends on the injection of known
quantities of an allergen in the hope of increasing the
amount of IgG over IgE capable of reacting with the
allergen
IgG blocks the binding of the allergen with IgE
Type I Hypersensitivity: Immunomodulation
Type I Hypersensitivity
Allergen extracts, Aqueous & Glycerinated
Antigen Source
FDA licenses over 600 distinct allergen extracts as safe and effective for immunotherapy.
Composed of proteins and other components
-Foods: Chicken egg albumin, casein, almond, scallops, etc.
-Animals:
cat, dog, horse, rat, chicken, duck, pigeon feathers, etc.
-Grasses:
Kentucky blue, red top, perennial rye, Bermuda, fescue, etc.
-Insects:
Cockroach, house-dust mite
-Molds:Aspergillus, Rhizopus, etc.
-Trees: White oak, cypress, cottonwood, maple, elm
-Weeds:
Ragweed, sagebrush, saltbush, wingsscalel, etc.
Dosage and Route
Progressive, escalating dose, modified to patient needs; SC
Indications
Treatment of patients with allergies upon natural exposure to allergens.
Effective against rhinitis, allergic asthma from cat, dog, grass, dust mite.
Adverse Reactions
Most common cause of systemic anaphylaxis, managed by dosing with epinephrine and in
some cases antihistimines.
Efficacy
7~90% of patients demonstrate improvement in symptoms within 12 weeks and
continuing for 1-2
years
Type I Hypersensitivity
Hymenoptera (Bee) Venom Protein
Antigen Source
Venoms of the following flying insects: Honey bee, Wasp, White-faced
hornet, Yellow hornet, Yellow jacket-, Composed of purified venom.
Dosage and Route
Progressive, escalating dose, modified to patient needs; SC
Indications
Treatment of patients with history of systemic reaction to stings
Adverse Reactions Anaphylaxis without warning within 20 mins. of
injections, managed by dosing with epinephrine and in some cases
antihistimines.
Efficacy
97% of patients have reduced anaphylaxis from stings, without therapy
60% will develop anaphylaxis with next sting.
Type I Hypersensitivity
Benzylpenicilloyl Polylysine
Antigen Source
Hapten(Benzylpenicilloyl moiety-polypeptide (lysine) containing
Dosage and Route Sterile skin test area on upper or outer arm, 5-10
mins. reaction time.
Indications
Used to assses risk of administering benzylpenicillins (i.e., penicillin G)
Adverse Reactions
Allergic reactions occur in <1% of recipients and is usually
characterized by intense 1ocali inflammation.
Efficacy
The test is 89-96% sensitive and specific. Consequently, 4-11% of
patients who test negative will react to treatment with penicillins.
Urticaria
Anaphylaxsis
Histamine binds to H1 receptors
triggers inflammatory responses
these are exaggerated responses
Histamine
blood vessels
vasodilation
increased blood flow
increased permeability
tissue edema
fluid leaking into
interstitial space
•Hypotension
•Laryngeal edema
•Angioedema
•Conjunctivitis
Extravascular Smooth Muscle
bronchial and laryngeal smooth muscle
constriction
restricted airway
Wheezing
Bronchoconstriction
NOTE: combined with
laryngeal edema
= high risk of losing
airway
GI Tract
Inflammation of intestinal mucosa
cramping
malabsorption
Mucosal Tissue
conjunctivitis
inflammation of eyelids
nose
rhinitis
bronchial (asthma)
bronchoconstriction
hypersecretion of mucus
Antihistamines
Treatment for nonlifethreatening allergies
H1 vs. H2 Receptors
H1: Receptors located on
Bronchial smooth muscle
histamine causes constriction
Arterioles
dilation of capillaries in skin
H1 vs. H2 Receptors
Vascular epithelium
increased permeability
H1 vs. H2 Receptors
H2
Gastric mucosa
secretion
of gastric acid and pepsin
Mast cells
tissues
Basophils
circulation
blocks histamine
release
Drugs
H1 Receptor Antagonists
oldest class of antihistamines
have a rapid onset
Actions (H1 Receptor Antagonists)
Bind to H1 receptors to block action of
histamine
**do block release
cannot
reverse effects of histamine
already bound
Indications (H1 antagonists)
Allergic response (non-life-threatening)
Motion sickness
Sedation
Cough
H1 Receptor Antagonists
Many possess anticholinergic effects
Side effects:
Increase heart rate
Constipation
Urinary retention
Insomnia
Nervousness
First Generation Antihistamines
bind with H1 receptors in the periphery
and in CNS
CNS effects
sedation
Peripheral effects
decrease itching, mucus production,
capillary permeability, saliva
production
Prototype First Generation
H1 Antagonists
Benadryl (diphenhydramine)
Travist (clemastine)
Zyrtec (cetirizine hydrocloride)
Chlor-Trimetron (chlorpheniramine)
Second Generation
Bind selectively to peripheral H1 receptors
do not cross the BBB
Prototypes
Zyrtec (cetirizine)
Allegra (fexofenadine)
Claritin (loratadine)
H2 Receptor Antagonists
AKA: H2 blockers
Actions
Target H2 receptors in the gastric mucosa
Decrease secretion of gastric acid
Examples
Tagamet (cimetadine)
Pepcid (famotidine)
Zantac (ranitidine HCL)
What would these drugs do during a Type I
hypersensitivity reaction?
MEDIATORS
A VARIETY OF CHEMOTACTIC, VASOACTIVE AND SPASMOGENIC
COMPOUNDS MEDIATE THE ANAPHYLACTIC REACTION.
•
IMMEDIATE (5-30 mins): histamines, leukotrienes
Intense reaction characterised by oedema, mucus secretion, and smooth
muscle spasm.
•
LATE (2-8 hours): leukotrienes, PAF, TNF-, cytokines
Recruit other inflammatory cells and release additional waves of mediators that
cause injury
Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display.
Blood Pressure (BP)
(continued)
Summary of
Effector Organ Responses
to Autonomic Stimulation
Part I
Be sure to memorize
all entries in this table
Goodman and Gilman’s
The Pharmacological Basis of Therapeutics
9th Ed. p. 110-111
Summary of
Effector Organ Responses
to Autonomic Stimulation
Part II
This part of the table you
do not need to memorize
Goodman and Gilman’s
The Pharmacological Basis of Therapeutics
9th Ed. p. 110-111




















































































































![[A] t - Dr. Agus Setiabudi, M.Si.](http://s1.studyres.com/store/data/008628332_1-495b65fba206219a51428cbf0e7b4981-150x150.png)