Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
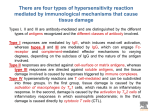
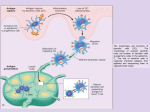
IPERSENSIBILTA’ e I MISFATTI DELLA RISPOSTA IMMUNITARIA • Risposta immunitaria diretta specificamente verso definite strutture molecolari (antigeni) • Risposta infiammatoria, processo aspecifico innescato da “ogni tipo” di danno tessutale e varia poco a seconda del tipo dell’agente scatenante • Ipersensibilità è l’eccessiva o non necessaria risposta immunitaria (anticorpale o dei linfociti T) che determina un rischio maggiore dell’antigene che l’ha evocata. • Classificazione secondo Coombs e Gell (1975) RISPOSTA IMMUNITARIA • INSUFFICIENTE Immunodeficienze • INADEGUATA Autoimmunità (rivolta contro il bersaglio sbagliato) • ECCESSIVA Ipersensibilità Consequences of Defective or Excessive Inflammation • Defective inflammation typically results in increased susceptibility to infections and delayed healing of wounds and tissue damage. – reflects the fundamental role of the inflammatory response in host defense, – Delayed repair is because the inflammatory response is essential for clearing damaged tissues and debris, and provides the necessary stimulus to get the repair process started. • Excessive inflammation is the basis of many categories of human disease. – allergies, in which individuals mount unregulated immune responses against commonly encountered environmental antigens, – autoimmune diseases, in which immune responses develop against normally tolerated selfantigens, are disorders in which the fundamental cause of tissue injury is inflammation. – cancer, atherosclerosis and ischemic heart disease, and some neurodegenerative diseases such as Alzheimer disease (not primarily disorders of the immune system). – prolonged inflammation and the fibrosis that accompanies it are responsible for much of the pathology in many chronic infectious, metabolic and other diseases. Immune response Adaptive immunity serves the important function of host defense against microbial infections, but immune responses are also capable of causing tissue injury and disease. Disorders caused by immune responses are called hypersensitivity diseases. This term arose from the clinical definition of immunity as "sensitivity," which is based on the observation that an individual who has been exposed to an antigen exhibits a detectable reaction, or is "sensitive," to subsequent encounters with that antigen. Normally, the immune response eradicates infecting organisms without serious injury to host tissues. However, sometimes these responses are inadequately controlled or inappropriately targeted to host tissues, and in these situations, the normally beneficial response is the cause of disease. Immunologic tissue injury and immunopathology, and some specific immunologic diseases • Hypersensitivity reactions, which give rise to immunologic injury in a variety of diseases, discussed throughout this book • Autoimmune diseases, which are caused by immune reactions against self • Immunologic deficiency syndromes, which result from genetically determined or acquired defects in some components of the normal immune system • Amyloidosis, association. a poorly understood disorder having immunologic Immunologic tissue injury and immunopathology, and some specific immunologic diseases • Contact with antigen leads not only to induction of a protective immune response, but also to reactions that can be damaging to tissues • Exogenous antigens occur in dust, pollens, foods, drugs, microbiologic agents, chemicals, and many blood products used in clinical practice. • The immune responses that may result from such exogenous antigens take a variety of forms, ranging from annoying but trivial discomforts, such as itching of the skin, to potentially fatal diseases, such as bronchial asthma. • The various reactions produced are called hypersensitivity reactions, and tissue injury in these reactions may be caused by humoral or cell-mediated immune mechanisms. Immunologic tissue injury and immunopathology, and some specific immunologic diseases • Injurious immune reactions may be evoked not only by exogenous environmental antigens, but also by endogenous tissue antigens • Some of these immune reactions are triggered by homologous antigens that differ among individuals with different genetic backgrounds. • Transfusion reactions and graft rejection are examples of immunologic disorders evoked by homologous antigens. • Another category of disorders, those incited by self-, or autologous, antigens, constitutes the important group of autoimmune diseases. Hypersensitivity diseases can be classified on the basis of the immunologic mechanism that mediates the disease • In immediate hypersensitivity (type I hypersensitivity), the immune response releases vasoactive and spasmogenic substances that act on vessels and smooth muscle and proinflammatory cytokines that recruit inflammatory cells. Immediate (typeI) Hypersensitivity Anaphylaxis; allergies; bronchial asthma (atopic forms) Production of IgE antibody → immediate release of vasoactive amines and other mediators from mast cells; recruitment of inflammatory cells (late-phase reaction) Vascular dilation, edema, smooth muscle contraction, mucus production, inflammation Hypersensitivity diseases can be classified on the basis of the immunologic mechanism that mediates the disease • In antibody-mediated disorders (type II hypersensitivity), secreted antibodies participate directly in injury to cells by promoting their phagocytosis or lysis and injury to tissues by inducing inflammation. Antibodies may also interfere with cellular functions and cause disease without tissue injury. Hypersensitivity diseases can be classified on the basis of the immunologic mechanism that mediates the disease • In immune complex-mediated disorders (type III hypersensitivity), antibodies bind antigens and then induce inflammation directly or by activating complement. The leukocytes that are recruited (neutrophils and monocytes) produce tissue damage by release of lysosomal enzymes and generation of toxic free radicals. Hypersensitivity diseases can be classified on the basis of the immunologic mechanism that mediates the disease • In cell-mediated immune disorders (type IV hypersensitivity), sensitized T lymphocytes are the cause of the cellular and tissue injury. Ipersensibilità di tipo I: allergia • Reazioni allergiche si manifestano quando un individuo che ha già prodotto IgE in risposta ad un antigene innocuo (allergene) viene successivamente in contatto con lo stesso Ag • IgE presenti principalmente nei tessuti si legano alla superficie dei mastociti attraverso il recettore ad alta affinità FceRI causando un cross-link dei recettori e stimolando la secrezione di mediatori chimici • FceRI sono presenti anche su basofili ed eosinofili attivati • Immediate (Type I) Hypersensitivity Immediate, or type I, hypersensitivity is a rapidly developing immunologic reaction occurring within minutes after the combination of an antigen with antibody bound to mast cells in individuals previously sensitized to the antigen The systemic reaction usually follows injection of an antigen to which the host has become sensitized. Many local type I hypersensitivity reactions have two well-defined phases: • The immediate, or initial, response is characterized by vasodilation, vascular leakage, and depending on the location, smooth muscle spasm or glandular secretions. These changes usually become evident within 5 to 30 minutes after exposure to an allergen and tend to subside in 60 minutes. • In many instances (e.g., allergic rhinitis and bronchial asthma), a second, late-phase reaction sets in 2 to 24 hours later without additional exposure to antigen and may last for several days. This late-phase reaction is characterized by infiltration of tissues with eosinophils, neutrophils, basophils, monocytes, and CD4+ T cells as well as tissue destruction, typically in the form of mucosal epithelial cell damage. Immediate hypersensitivity Kinetics of the immediate and late-phase reactions. The immediate vascular and smooth muscle reaction to allergen develops within minutes after challenge (allergen exposure in a previously sensitized individual), and the late-phase reaction develops 2 to 24 hours later Downloaded from: StudentConsult (on 15 March 2010 05:03 PM) © 2005 Elsevier Morphology The immediate reaction (B) is characterized by vasodilation, congestion, and edema, and the late phase reaction (C) is characterized by an inflammatory infiltrate rich in eosinophils, neutrophils, and T cells. (Courtesy of Dr. Daniel Friend, Department of Pathology, Brigham and Women's Hospital, Boston, MA.) Downloaded from: StudentConsult (on 15 March 2010 05:03 PM) © 2005 Elsevier Allergic reactions can be divided into an immediate response and a late-phase response. direct effects on blood vessels and smooth muscle of rapidly metabolized mediators such as histamine released by mast cells. The late-phase response is caused by the effects of an influx of inflammatory leukocytes attracted by chemokines and other mediators released by mast cells during and after the immediate response Photographs courtesy of A.B. Kay. Pathogenesis of immediate (type I) hypersensitivity reaction. The late-phase reaction is dominated by leukocyte infiltration and tissue injury. Downloaded from: StudentConsult (on 15 March 2010 05:03 PM) © 2005 Elsevier The differentiation of Th cells depends on the antigen source, the quantity of allergen, and the cytokines produced. Bacterial antigens or a high dose of antigen will induce IL-12 from macrophages. In addition, the developing Th1 cells produce IFNγ, which further enhances the production of Th1 cells. Low-dose antigen without adjuvant will induce Th2 cells, which produce both IL-4 and IL-5. IL-4 plays a role in (i) enhancing the growth of Th2 cells; (ii) the expression of the gene for IgE. In turn IgE binds to the high-affinity receptor for IgE on mast cells. Downloaded from: StudentConsult (on 16 March 2010 11:42 AM) © 2005 Elsevier (1) The serum concentration of IgE (which is around 100 IU/ml) is only approximately 0.001% that of IgG (around 10 mg/ml) and comprises less than 0.001% of the total immunoglobulin. Levels in atopic patients tend to be raised, and this is especially so in atopic eczema (1 IU = 2.4 ng). (2) The higher the level of IgE the smaller the percentage of the population affected, but the greater the likelihood of atopy. Where the level is greater than 450 IU/ml the majority of subjects are atopic. Downloaded from: StudentConsult (on 16 March 2010 11:42 AM) © 2005 Elsevier Activation of mast cells in immediate hypersensitivity and release of their mediators. ECF, eosinophil chemotactic factor; NCF, neutrophil chemotactic factor; PAF, platelet-activating factor. Downloaded from: StudentConsult (on 15 March 2010 05:03 PM) © 2005 Elsevier Primary Mediators Primary mediators contained within mast-cell granules can be divided into three categories: • Biogenic amines. The most important vasoactive amine is histamine. Histamine causes intense smooth muscle contraction, increased vascular permeability, and increased secretion by nasal, bronchial, and gastric glands. • Enzymes. These are contained in the granule matrix and include neutral proteases (chymase, tryptase) and several acid hydrolases. The enzymes cause tissue damage and lead to the generation of kinins and activated components of complement (e.g., C3a) by acting on their precursor proteins. • Proteoglycans. These include heparin, a well-known anticoagulant, and chondroitin sulfate. The proteoglycans serve to package and store the other mediators in the granules. Secondary Mediators Secondary mediators include two classes of compounds (1) lipid mediators and (2) cytokines • Leukotrienes. Leukotrienes C4 and D4 are the most potent vasoactive and spasmogenic agents known. On a molar basis, they are several thousand times more active than histamine in increasing vascular permeability and causing bronchial smooth muscle contraction. Leukotriene B4 is highly chemotactic for neutrophils, eosinophils, and monocytes. • Prostaglandin D2. This is the most abundant mediator derived by the cyclooxygenase pathway in mast cells. It causes intense bronchospasm as well as increased mucus secretion. Secondary Mediators Secondary mediators include two classes of compounds (1) lipid mediators and (2) cytokines • • • • • • • • Platelet-activating factor (PAF). PAF is produced by some mast-cell populations. It causes platelet aggregation, release of histamine, bronchospasm, increased vascular permeability, and vasodilation. In addition, it has important pro-inflammatory actions. PAF is chemotactic for neutrophils and eosinophils. At high concentrations, it activates the newly recruited inflammatory cells, causing them to aggregate and degranulate. Because of its ability to recruit and activate inflammatory cells, it is considered important in the initiation of the late-phase response. Although the production of PAF is also triggered by the activation of phospholipase A2, it is not a product of arachidonic acid metabolism. Secondary Mediators Secondary mediators include two classes of compounds (1) lipid mediators and (2) cytokines • Cytokines. Mast cells are sources of many cytokines, which play an important role in the late-phase reaction of immediate hypersensitivity because of their ability to recruit and activate inflammatory cells. The cytokines include TNF, IL-1, IL-3, IL-4, IL-5, IL-6, and GM-CSF, as well as chemokines, such as macrophage inflammatory protein (MIP)-1α and MIP-1β. Mast cell-derived TNF and chemokines are important mediators of the inflammatory response seen at the site of allergic inflammation. Inflammatory cells that accumulate at the sites of type I hypersensitivity reactions are additional sources of cytokines and of histaminereleasing factors that cause further mast-cell degranulation. Normal larynx Laryngeal oedema MECCANISMI EFFETTORI: EFFETTO DELL’ATTIVAZIONE DEI MASTOCITI IN DIVERSI TESSUTI TRATTO GASTROINTESTINALE Aumento della SECREZIONE FLUIDI Aumento della PERISTALSI ATTIVAZIONE DEI MASTOCITI Espulsione contenuto del tratto intestinale (vomito diarrea) VASI SANGUIGNI Aumento del FLUSSO SANGUIGNO Aumento della PERMEABILITA’ Aumento di fluidi nei tessuti causa aumento di flusso VIE AEREE Aumento della SECREZIONE di MUCO Diminuizione del DIAMETRO Congestione e blocco delle vie aeree (starnuti tosse e muco) Gonfiore e secrezione di muco nel tratto nasale linfonodi, aumento di cellule e proteine nei tessuti, Aumento di risposta effettrice nei tessuti Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier Downloaded from: StudentConsult (on 18 November 2008 01:51 PM) © 2005 Elsevier