Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
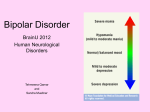
Definition A group of disorders of variable severity in which the central symptom is pervasive disturbance of mood (either depression or mania) usually accompanied by other characteristic symptoms. Major depressive disorder Epidemiology The lifetime prevalence is 10% for women, and 5% for men. The lifetime prevalence in monozygotic twins of patients is 50%. I- Presence of one or more major depressive episodes. Major depressive episode A- five or more of the following symptoms; at least one of the symptoms is either (1) depressed mood or (2) loss of interest: 1- Depressed mood for at least two weeks. 2- Loss of interest and pleasure in previously interestable activities. 3- Insomnia or hypersomnia. 4- Psychomotor retardation or agitation. 5- Decreased or increased appetite and loss or increase in weight. 6- Easy fatigability. 7- Decreased concentration. 8- Feelings of worthlessness or guilt. 9- Recurrent thoughts of death or suicidal ideation, plan or attempts. B- Not substance-induced or not due to general medical condition. II- There has never been a manic or hypomanic episodes. III- Significant impairment of occupational and social functioning. 1- Dysthymic disorder: a- Depressed mood for at least 2 years. b- two or more of the following: Poor appetite or overeating. Insomnia or hypersomnia. Low energy or fatigue. Low self-esteem. Poor concentration. Feelings of hopelessness. c- Significant impairment of occupational and social functioning. 2- Minor depressive disorder: episodes of at least 2 weeks of depressive symptoms but with fewer than the five items required for major depressive disorder. 3- Recurrent brief depressive disorder: recurrent episodes of depression that last less than two weeks. 4- Premenstrual dysphoric disorder: symptoms of depresed mood, anxiety, affective lability, decreased interest in activities regularly occur during the last week of luteal phase and remit within a few days of the onset of the menses. 5- Secondary mood disorder: Substance-induced mood disorder. Mood disorder due to general medical condition. I- Neurotransmitter hypothesis: decreased activity of biogenic amines serotonin, norepinephrine, and dopamine. II- Genetic theory: Increase the incidence of depression in subjects related to an affected person. No consolidated studies correlate between depression and specific chromosomes. III- Brain structure theory: Some patients showed smaller caudate nuclei, and frontal lobes. Diminished basal ganglia blood flow. IV- Psychosocial theory: as indicated by cognitive triad; Negative self-view “things are bad because I’m bad”. Negative interpretation of experience “ everything has always been bad” Negative view of future “anticipation of failure”. A- Pharmacotherapy: Serotonin specific reuptake inhibitors (SSRIs): Mode of action: inhibit reuptake of serotonin so promote its action on postsynaptic receptors. Indications: major depressive disorder, anxiety disorder, bulimia nervosa. Adverse effects: nausea, decreased appetite, delayed ejaculation. Examples: fluoxetine, paroxetine. Tricyclic antidepressants: Mode of action: inhibit reuptake of serotonin and norepinephrine so promote their actions on postsynaptic receptors. Indications: major depressive disorder, panic disorder. Adverse effects: sedation, atropine-like action. Examples: imipramine, clomipramine. Buprobion: Mode of action: inhibit reuptake of dopamine and norepinephrine so promote their actions on postsynaptic receptors. Indications: major depressive disorder, attention deficit/hyperactivity disorder, smoking cessation. Adverse effects: mild symptoms of weight loss, dry mouth or constipation. B- Electro-convulsive therapy: is useful in refractory major depressive disorder, major depressive episode with suicidal attempts or with psychotic symptoms (like delusions and hallucinations). C- Psychotherapy: 1- Cognitive therapy: aims to correct negative cognitions. 2- Supportive psychotherapy: aims to provide emotional support. 3- Family therapy: if patient’s depression is disrupting the family stability, or when depression is related to family dynamics. Bipolar I disorder Epidemiology: The lifetime prevalence is 0.4-1.6%. The lifetime prevalece in monozygotic twin of patients is up to 90%. I- Presence of one or more manic episodes. Manic episode A- Elated mood or irritable mood for one week or more. B- If mood is elated (3) or more of the following must be present but if mood is irritable (4) or more of the following must be present: 1- Inflated self-esteem or grandiosity. 2- Decreased need for sleep. 3- More talkative than usual. 4- Flight of ideas. 5- Distractability. 6- psychomotor agitation. 7- Loss of normal social and sexual inhibition. 8- Excessive involvement in pleasurable activities that have a high potential for painful consequences. C- Not substance-induced or not due to general medical condition. II- With or without presence of major depressive episodes. III- Significant impairment of occupational and social functioning. 1- Bipolar II disorder: major depressive episodes with hypomanic episoes. 2- Cyclothymic disorder: Numerous episodes of hypomania and numerous episodes of depressive symptoms for at least 2 years. The symptoms are not sufficient to diagnose manic episodes or major depressive episodes. Significant social and occupational impairment. 3- Secondary mood disorder: Substance-induced mood disorder. Mood disorder due to general medical condition. I- Neurotransmitter hypothesis: increased activity of biogenic amines serotonin, norepinephrine, and dopamine. II- Genetic theory: Increase the incidence of bipolar I disorder in subjects related to an affected person. Associations between bipolar I disorder and genetic markers have been reported for chromosomes 5, 11, X. III- Brain structure theory: Some patients showed enlarged cerebral ventricles. Magnetic resonance spectroscopy showed abnormal regulation of membrane phospholipid metabolism. IV- Psychosocial theory: feeling of inadequacy and worthlessness are converted by means of denial, reaction formation and projection to grandiose delusions. A- Hospitalization: especially with severily psychomotor agitated patients. B- Pharmaotherapy: Mood stabilizers: used in the treatment and prevention of manic and depressive episodes of bipolar disorders. Lithium: it is the standard treatment of bipolar disorder. the therapeutic blood level is 0.8-1.2 mEq/litre. Serum level must be done regularly to safeguard againt subtherapeutic or toxic levels. Valproate: the first-line drug in bipolar disorder with dysphoric mood, and rapid cycling bipolar disorder. has broad therapeutic index and effective at levels of 50-125 microgram/ml. Lamotrigine: the most effective drug in controling depressive episodes of bipolar disorder, and do not require blood monitoring. During manic episode antipsychotic drugs (see treatment of schizophrenia) are used to promote rapid amelioration of the symptoms. During major depressive episode antidepressant drugs (see treatment of major depressive disorder) may be used especially buprobion or SSRIs in combination with mood stabilizers to avoid switching to mania. B- Electroconvulsive tharpy: is at least equal to lithium in the treatment of acute and severe manic episodes. D- Psychotherapy: Cognitive therapy; to increase compliance with pharmacotherapy. Supportive therapy: with chronic patients who may have significant interepisodic residual symptoms and social dysfunction. Family therapy: if patient’s disorder is disrupting the family stability, and because the disorder is strongly familial.