Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Developmental disability wikipedia , lookup
Factitious disorder imposed on another wikipedia , lookup
Depersonalization disorder wikipedia , lookup
Schizoaffective disorder wikipedia , lookup
Antisocial personality disorder wikipedia , lookup
Conversion disorder wikipedia , lookup
Mental status examination wikipedia , lookup
Conduct disorder wikipedia , lookup
Generalized anxiety disorder wikipedia , lookup
Mental disorder wikipedia , lookup
Separation anxiety disorder wikipedia , lookup
Narcissistic personality disorder wikipedia , lookup
Pyotr Gannushkin wikipedia , lookup
History of psychiatry wikipedia , lookup
Dissociative identity disorder wikipedia , lookup
Causes of mental disorders wikipedia , lookup
Abnormal psychology wikipedia , lookup
Diagnostic and Statistical Manual of Mental Disorders wikipedia , lookup
Controversy surrounding psychiatry wikipedia , lookup
Classification of mental disorders wikipedia , lookup
Sluggish cognitive tempo wikipedia , lookup
History of mental disorders wikipedia , lookup
Autism therapies wikipedia , lookup
Attention deficit hyperactivity disorder wikipedia , lookup
Spectrum disorder wikipedia , lookup
Attention deficit hyperactivity disorder controversies wikipedia , lookup
Child psychopathology wikipedia , lookup
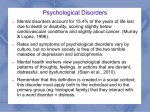
Back to Basics Review of ADHD, Learning Disabilities, and Pervasive Developmental Disorders Dhiraj Aggarwal, MD, FRCP (C ) Child and Youth Psychiatrist, Children’s Hospital of Eastern Ontario Assistant Professor, University of Ottawa [email protected] April 2nd , 2013 Disclosures • No affiliations to disclose Causes/Sources of School Refusal 1. 2. 3. 4. 5. 6. Separation Anxiety Disorder (50%-80%) Truancy Mood Disorders (Major depressive Disorder/Bipolar Disorder) Other Anxiety Disorders Overt Psychotic Disorder Realistic fear of bodily harm in a dangerous school setting (bullying, gangs) 7. Academic Underachievement (Learning disabilities, ADHD, Developmental delay) 3 Pervasive Developmental Disorders Outline • Diagnosis • Epidemiology • Etiology • Assessment • Treatment –Non medication treatments –Medication treatments Back to Basics – Dr. D. Aggarwal Classification of Pervasive Developmental Disorders (PDDs) According to DSM-IV TR Pervasive Developmental Disorders Autistic Disorder Asperger’s Disorder PDD-NOS Autism Spectrum Disorders Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Childhood Disintegrative Disorder Rett’s Disorder Pervasive Developmental Disorder • Prevalence 1% (1/88) (2010, Can. J. Psych. 55(11) 71520; Arch Gen Psyc 2011, 68(5), 459-65) • Male to female ratio: 5: 1 • < 40% are mentally retarded (intellectual disability) • Affects social interactions +/- communication, play, interests and behaviour Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Autistic Disorder • Problems in all 3 core domains – Social abnormality – Language abnormality – Stereotyped repetitive pattern of behavior • Onset of symptoms before 3 yrs of age • Most severely affected group of ASD Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Diagnostic criteria for Autism • require the presence of 6 symptoms from 3 categories: – Impaired reciprocal social interaction (at least 2/4 symptoms) – Impaired communication (1/4) – Restricted, repetitive and stereotyped behaviors (1/4) Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Qualitative impairment in Social Interaction Qualitative impairment in Social Interaction - Impairment in the use of multiple nonverbal behaviors: eye to eye gaze (eye contact), facial expression, body postures and gestures to regulate social interaction - Failure to develop peer relationships appropriate to developmental level - Lack of spontaneous seeking to share enjoyment, interests or achievements with other people (not showing, bringing or pointing out objects of interests) - Absence of social or emotional reciprocity Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Qualitative impairment in Communication – Delay in or total lack of development of spoken language (no attempt to compensate with gestures or mime) – If speech present, marked impairment in the ability to initiate or sustain conversation with others – Stereotyped and repetitive use of language or idiosyncratic language – Lack of varied, spontaneous make-believe play or social imitative play appropriate to developmental level Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Restricted repetitive and stereotyped patterns of behavior, interest and activities – Encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or in focus – Inflexible adherence to specific, nonfunctional routines or rituals – Stereotyped and repetitive motor mannerisms: hand or finger flapping or twisting, complex whole-body movements – Persistent preoccupation with parts of objects Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Etiology • Genetic - increased risk in siblings and in twins – Twin concordance, monozyg. 60% vs 5% dizygotic – ASDs tend to occur more often in people who have certain genetic or chromosomal conditions. About 10% of children with autism are also identified as having Down syndrome, fragile X syndrome, tuberous sclerosis, and other genetic and chromosomal disorders • Environmental, toxins, gastrointestinal, immunological factors inconclusive Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Unproved Theories • Vaccines containing thimerosal are not associated with autism. • No association between MMR vaccine and autism (MMR vaccine producing enterocolitis, causing “leaky gut”, which then leads to increased absorption of peptides with bioactive properties of endogenous opioids that produce the symptoms of autism.) Consider Evaluation if by: • 12 months: No babbling or gesturing (pointing, waving byebye), not responding to own name • 16 months: No single words • 24 months: No spontaneous 2 word phrases (i.e. not echolalia or repeating someone else’s words) • Any age: any loss of any language or social skills Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Asperger’s Disorder -Hans Asperger 1944 (1980’s) -Diagnosed later than Autism -IQ within normal range -Qualitative impairment in Social Interaction -Restricted repetitive and stereotyped patterns of behavior, interest and activities Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Language in Asperger's “Unusual but not Absent” • There is no clinically significant general delay in language • Normal language milestones but atypical: – Language is one sided (lecture) – Perseverates on topic of interest – Pragmatics- turn taking, facial expression, body language, overly formal “little professor” – Prosody- intonation, volume, rhythm – Conversational intent- sarcasm, metaphors Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal PDD-NOS • Symptoms/impairment : – Social interaction and – Communication OR Behavior • That do not reach threshold for diagnosis of a specific PDD. • Most common but least studied Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Differential Diagnosis for PDD • • • • • • • • • • • Specific Developmental Disorder eg language Mental Retardation not associated with PDD OCD, Social Phobia, and other anxiety disorders Tourette’s and tic disorders ADHD, oppositional defiant disorder (ODD) Giftedness/precocity Selective mutism Reactive attachment disorder, PTSD Schizophrenia of childhood onset Schizotypal/schizoid personality disorder Specific medical/neurological conditions Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Evaluation • History – Pregnancy, neonatal and developmental hx, medical hx, family and psychosocial factors, intervention hx. • Direct interaction and behavioural observations of child • Collateral of observations of child in social settings • Screening and diagnostic questionnaires • Psychological evaluation • Speech/language/communication assessment • OT evaluation Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Autism-Specific Questionnaires • M-CHAT (Modified Checklist for Autism in Toddlers) • CARS (Childhood Autism Rating Scale) • GARS (Gillian Autism Rating Scale) • Autism Diagnostic Interview-revised (ADI-R) • Autism Diagnostic Observation ScheduleGeneric (ADOS-G) Medical Evaluation • Physical exam to identify dysmorphic physical features • Audiology/visual evaluation • Chromosomal microarray analysis recommended: submicroscopic chromosome deletions, duplications (copy number variant) detected in 10%% of people with ASD. • Metabolic testing based on clinical features. • EEG if history of seizure or history of significant regression in social or communication functioning. Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Goals of treatment • In order to optimize outcome, it is important to screen/diagnose early and to initial intensive behavioral therapy. • Promote functional conversational language. • Promote social interactions while mitigating repetitive, self-stimulatory behaviors, tantrums, aggression and self-injurious behaviors. Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Interventions • Applied Behavior Analysis (ABA). Uses the principles of operant conditioning to teach specific social, communicative, and behavioral skills to children with ASD. It involves teaching new behaviors by explicit reinforcement of these behaviors, • Typical Target Behaviors • Attentional skills • Imitation skills • Adaptive and self help skills • Social skills Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal Medications • No medication is available to treat the core symptoms of autism (deficits in communication and social interaction). • Risperidone and aripiprazole are approved and helpful to assist in irritability, managing tantrums, aggression and self-injurious behaviors. • Stimulant (eg methylphenidate) medication is helpful to assist with inattentive, impulsive and hyperactive behaviors. – ADHD not diagnosed in presence of PDD according to DSM-IV, but ADHD symptoms are common in PDD (>50%) Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal References • www.autism-society.org • www.teacch.com • http://www.nichd.nih.gov/health/topics/autism/Pages/def ault.aspx • http://www.aspergers.com/ • http://www.asatonline.org/ • ASD video glossary: Autism Speaks http://www.autismspeaks.org/video/glossary.php • Management of Children With Autism Spectrum Disorders SM Myers, CP Johnson, Pediatrics, 120 (5), 1162-1182 (2007) Unit 3 – Autism Spectrum Disorders – Dr. D. Aggarwal ADHD Outline • Diagnosis • Assessment • Co-morbidity • Epidemiology • Etiology • Natural History • Treatment – Non medication options – Medication options Case 10 year old boy Joshua presents with difficulty sitting still, distractibility and aggressive behaviour. Mother “The teacher thinks he has ADHD and she told me to put him on Ritalin….I told the school he is just an active boy and the school should be able to manage him…..Dr. what do you think is going on?” Differential Diagnosis of ADHD • Not every inattentive or disruptive child has ADHD • A child may be inattentive or act out because of: – – – – – Learning problems, Mental Retardation Mood (Depression or Bipolar) Anxiety, including OCD Autism Spectrum Disorder Substance related disorder NOS – Sleep problems – Impaired hearing or vision – Personality Change Due to a GMC (ie head injury) – Age appropriate behaviours in active child – Understimulating environment (gifted child) APA, DSM-IV TR, 2000 DSM-IV-TR Symptoms for ADHD Inattention Hyperactivity 1. 1. 2. 3. 4. 5. 6. 2. 3. 4. 5. 6. 7. 8. 9. Doesn’t attend to details in schoolwork Difficulty sustaining attention in tasks/play Doesn’t listen Doesn’t complete tasks Difficulty organizing Avoids tasks requiring focus Loses things Distractible Forgetful Fidgets Leaves seat Runs about Doesn’t play quietly “On the go” Talks excessively Impulsivity 7. 8. 9. Blurts out answers Doesn’t await turn Interrupts or intrudes (APA, DSM-IV TR, 2000) DSM-IV-TR Diagnostic Criteria for ADHD • Threshold: Symptoms of inattention and/or hyperactivity-impulsivity for ≥6 months: – At least 6/9 inattentive symptoms: ADHD, inattentive type – At least 6/9 hyperactive-impulsive symptoms: ADHD, hyperactiveimpulsive type – At least 6/9 in each category*: ADHD, combined type • Onset before age 7 years* • Impairment in at least two settings • Exclusion: Symptoms do not occur in the context of PDD* or psychosis, and are not better accounted for by another mental disorder *May be changed in the new DSM-5 (APA, DSM-IV TR, 2000) What part of the assessment is the least helpful in making the dx of ADHD in a 15year old teen? a) Parent interview b) Teen interview c) Teen mental status d) Rating scale completed by parent e) Rating Scales completed by teacher What part of the assessment is the most helpful in making the dx of ADHD in a 15year old teen? a) case conference with teachers and parents to get a better understanding of the teens behaviour at school b) interview with parent about developmental history and past academic history c ) interview with the teen d) observing the teen in class e) rating scales completed by teacher and parent Assessment in Children and Adolescents • Parent interview including developmental history • Child/adolescent interview • Information from teachers and other sources • Rating Scales -useful to support clinical evaluation and monitor progress, but should not be used on their own to make a diagnosis • Conners Rating Scale-Revised (Parent/Teacher) • SNAP-IV Teacher/Parent Rating Scale (available at www.caddra.ca) Assessment (cont.) • Medical evaluation: – History and physical examination – Hearing and vision tests – Laboratory and imaging tests only if indicated by the clinical evaluation • Consider a psychoeducational evaluation, including both cognitive and academic testing, to assess for learning problems Co-morbidity • Children with ADHD have high rates of comorbid psychiatric disorders • Almost 70% of children with ADHD had at least one co-morbid condition • Disorders that are frequently co-morbid with ADHD: – – – – – Learning disorders Anxiety & depressive disorders Oppositional defiant disorder & conduct disorder Substance use disorders Tic disorders Pliszka et al., 2007; Spencer et al., 2007; Spencer et al., 1999; MTA Cooperative Group, 1999 Father “How common is ADHD? What causes ADHD? Will Joshua outgrow ADHD ? “ Prevalence of ADHD • School age children: 6-9% (Wolraich et al., 1998; CDC, 2010; Ontario Child Health Study, 1989) • Gender differences: 9.0% in boys (4-16 yrs old) and 3.3% in girls (OCHS, 1989) • Adult : 4.4% (NCS-R, 2006) • ADHD accounts for 30-50 % of mental health referrals (MTA Cooperative Group, 1999) • ADHD Subtypes in children: (Polanczyk et al., 2007) – – – Combined (50-75%) Inattentive (20-40%) Hyperactive-impulsive (<5-15%) Etiology • Genetic factors are most important: – Heritability is about 75% – Implicated genes: DAT1, DRD4.7, DRD5, DBH, 5-HTT, HTR1B, SNAP-25 • Nongenetic factors: – – – – Perinatal stress & low birth weight Traumatic brain injury Maternal smoking during pregnancy Severe early deprivation Faraone et al., 2005; Pliszka et al., 2007 Etiology (cont.) • Neurobiology: – Implicated brain regions: prefrontal cortex, basal ganglia, corpus callosum, and cerebellum – Implicated neurotransmitter systems: dopamine and norepinephrine • No evidence that ordinary variations in child-rearing practices contribute to the etiology of ADHD Krain & Castellanos, 2006; Pliszka et al., 2007 ADHD Persists from Childhood to Adulthood Children with ADHD Prevalence in juvenile population 6%-9% 60% will exhibit symptoms into adulthood Adults with ADHD Prevalence in adult population 3%-5% (Biederman et al., 2000; Rasmussen et al., 2000; Weiss et al., 1993) ADHD Course of the Disorder - Hyperactive-impulsive symptoms are more likely to improve or become internalized (e.g. changed into nervous tension) Hyperactivity -inattentive symptoms are more likely to persist Impulsivity Inattention --Time-- (Faraone et al., 2005) Father “I think my wife has ADHD. I made a video to show you. what do you think ?” Mother “ How do you treat ADHD? Are there any side effects with medications? Are there any long-term side effects of medications? Behavioural Management vs. Medication for ADHD Non-Medication Interventions • Psychoeducation • Behavioural Parent Management Training • Behavioural School and Academic Intervention AACAP ADHD Practice parameter. JAACAP. 2007 American Academy of Pediatrics. Pediatrics. 2011 Stimulants • • Duration of Action (hours) Methylphenidate • Ritalin • Ritalin SR • Biphentin • Concerta 4 (3-4) 8 (4-6?) 8-10 12 (8-14) Amphetamines • Dexedrine • Dexedrine spansule • Adderall XR • Lisdexamfetamine (Vyvanse) 4 (3-6) 10-12 (5-8?) 10-12 12-13 Pharmacodynamics • Methylphenidate: –Blocks DA and NE transporters in the presynaptic neuron, thus inhibiting reuptake and resulting in increased synaptic concentrations of these neurotransmitters •Amphetamines: –Stimulate release of DA and, to a lesser extent, NE, from presynapticsites –Have secondary effects on inhibiting DA reuptake Lisdexamfetamine (Vyvanse) • Lisdexamfetamine dimesylate (LDX) is a pharmacologically inactive prodrug >>Low abuse potential • Clinical effect for 12 hours or more (12h: monograph information, 13h in a clinical trial in children and 14h in adults) • Can be diluted in water if the child has difficulties swallowing Stimulant Adverse Effects • • • • • • • Initial insomnia Decreased appetite, weight loss Small increases in HR and diastolic BP Nausea/vomiting, abdominal pain Headache Thirst Palpitations • Anxiety • Social withdrawal, decreased spontaneity • Increased activity, aggression, irritability, dsyphoria • Tics • Risk of growth supression Monitoring for Stimulants • Height and weight on growth charts • HR and BP at baseline, with dose changes and periodically thereafter • Use parent and teacher rating scales to monitor response and side effects at different doses Atomoxetine (non stimulant) • Atomoxetine has been studied as a potential treatment for depression, but was found to be ineffective • Selective norepinephrine (NE) reuptake inhibitor (NRI) Health Canada (October 2011) • A safety announcement which warns of the risk of increased blood pressure and increased heart rate with the use of atomoxetine • Atomoxetine should not be prescribed to patients with symptomatic cardiovascular diseases, moderate to severe hypertension or severe cardiovascular disorders whose condition would be expected to deteriorate if they experienced clinically important increases in blood pressure or heart rate • Following similar principles for stimulants with respect to cardiac work up and monitoring 2012 CADDRA Guidelines Medical Treatment of ADHD 1st line 2nd line Long Acting Short Acting XR®) MAS (Adderall CR MPH MLR (Biphentin ®) OROS MPH (Concerta ®) Atomoxetine (Strattera ®) Lisdexamphetamine (Vyvanse ®) Dexedrine® Dexedrine ® Spansules Ritalin ® IR Ritalin ® SR 3rd line off label Imipramine Modafinil Wellbutrin® (CADDRA ,2011) Suggested Pharmacological Algorithm for ADHD 1a. Stimulants* (try methylphenidate and at least one amphetamine before moving on) 1b. Atomoxetine* 2. α-2 agonists** (clonidine, clonidine XR, guanfacine XR) 3a. Bupropion 3b. Tricyclic antidepressants 4. Modafinil 5. Other medications and medication combinations *Only the stimulants and atomoxetine are approved by Health Canada to treat ADHD in youth and adults ** Clonidine XR and guanfacine XR are approved by the FDA to treat ADHD in youth (neither agent is available in Canada) (Wilens, AACAP 57th Annual Meeting, 2010) (Slide by Dr. D. Gorman, 2011) (CADDRA, 2011) (CADDRA, 2011) Mother “what should I tell the school?” Online ADHD Resources • www.teachadhd.ca This site is designed specifically for teachers, but the information and down-loadable materials are also of interest for parents and clinicians. This website is developed and maintain by The Hospital for Sick Children, Toronto. • http://www.aacap.org/galleries/defaultfile/adhd_parents_medication_guide_english.pdf • www.caddac.ca – Centre for ADHD Awareness Canada – national, umbrella organization providing leadership in education and advocacy for ADHD organizations and individuals across Canada. Questions ?