Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
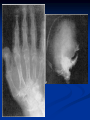
Parathyroid Glands HUSSEN.S.ALNAKHLY PARATHYROID GLAND Location: •Usually paired. •Very small (less than 5 mm). •Called parathyroid glands because of their position on posterior margins outer surface of thyroid gland. •More superior of each pair usually near middle of margin of lobe. •More inferior of each pair usually at inferior apex of lobe. Development: Like thyroid gland, develop from endodermal thickening in floor of early pharynx and epithelium of 3rd and 4th gill slit pouches. Anatomy Arterial supply usually from inferior thyroid art Superior glands usually imbedded in fat on posterior surface of middle or upper portion of thyroid lobe Lower glands near the lower pole of thyroid gland In 1-5% pts, inferior gland in deep mediastinum Histology 50/50 parenchymal cells, stromal fat Chief cells – secrete PTH Waterclear cells Oxyphil cells Parathyroid Hormone Synthesized in chief cells as large precursor – preproparathyroid hormone Cleaved intracellularly into proparathyroid hormone then to final 84 AA PTH PTH then metabolized by liver into hormonally active N-term and inactive C-term PTH function Hyperparathyroidism Primary Hyperparathyroidism Normal feedback of Ca disturbed, causing increased production of PTH Secondary Hyperparathyroidism Defect in mineral homeostasis leading to a compensatory increase in parathyroid gland function Etiology Unknown cause Single gland adenomatous disease Multiglandular disease – exogenous stimulus Ionizing radiation exposure Clinical Presentation Nephrolithiasis Bone Disease Peptic Ulcer Disease Psychiatric disorders Muscle weakness Constipation Polyuria Pancreatitis Myalgia Arthralgia Hypercalcemia Hyperparathyroidism (most common) Malignancy (most common in hospitalized) Lytic metastases to bone PTHrP producer Sarcoidosis / granulomatous disease Vit D intoxication Thiazides Hyperthyroidism Familial hypocalciuric hypercalcemia Renal Complications Generally the most severe clinical manifestations Many have frequency, polyuria, polydipsia Usually present w/ nephrolithiasis (20-30%) Calcium phosphate or Calcium oxalate Nephrocalcinosis (in 5-10%) – calcification w/in parenchyma of kidneys Severe renal damage Hypertension secondary to renal impairment Bone Disease Osteitis fibrosa cystica In early descripts of disease, many had severe bone disease (50-90%), but now 5-15% Subperiosteal resorption – pathognomonic of hyperparathyroidism Gastrointestinal Manifestations Peptic Ulcer disease Pancreatitis Cholelithiasis – 25-35% Neuromuscular complications Muscular weakness, fatigue More commonly in proximal muscles Sensory abnormalities also possible Laboratory Diagnosis Elevated Serum Ca and PTH Must measure Ionized Ca (subtle cases of hyperPTH will have normal Serum Ca) 50% will have hypophosphatemia Elevated Alkaline Phosphatase in 10-40% Hyperchloremic metabolic acidosis Low Mg in 5-10% High Urinary Ca in almost all cases