Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
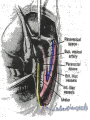
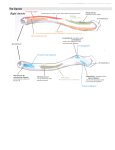
Retroperitoneal surgery 3 By Dr. Khattab Omar, MD Prof. & Head of Obstetrics and Gynaecology Department Faculty of Medicine, Al-Azhar University, Damietta Introduction Retroperitoneal space of the true pelvis differs from retroperitoneal areas elsewhere in the abdomen by the presence of the sub-peritoneal areolar (cellular) connective tissue. We can recognize about 6 retroperitoneal spaces. Cardinal lig The subperitoneal area of the pelvis is partitioned into potential spaces by the various organs & their respective fascial coverings, and by the selective thickenings of the endopelvic fascia into ligaments and septa. Vesical fascia Cut edge of the peritoneum Vesicovaginal lig. & space Indications for development of retroperitoneal surgical approaches 12345- Malignancy & Lymphadenectomy. Endometriosis. Chronic PID. Tubo-ovarian abscess. Complications in post-hysterect. reserved ovaries. 6- Hypogastric artery ligation. 7- Large, cervical, ligamentous myoma 8-Vaginally-inaccessible urinary fistula 9- Colpopexy. 10- Laparoscopic hysterectomy. The vesicovaginal & the rectovaginal spaces The vesicovaginal space Incise the vesicouterine peritoneal fold transversely. Push the bladder down bluntly or by sharp dissection. Moist gauze packing usually controls any encountered slow venous bleeding. A common error is to dissect too close to the cervix and fail to get into the proper plane Surgical importance - Developing this space gives access to the vesicouterine ligament which contains the ureter as it passes to the bladder. - Developing this space gives access to vesicovaginal fistula & cervical fibroid. The rectovaginal space (plane) It extends from the Douglas pouch to the perineal body. It is bounded anteriorly by the rectovaginal septum (firmly adherent to the vagina), and posteriorly by the anterior rectal wall. How to develop? Incise the peritoneum between the insertion of the 2 uterosacral lig. Bluntly dissect the vagina from the rectum by sweeping the palm along the posterior vaginal wall. For adherent areas, sharp dissection against the vagina is used. Surgical importance -Rectocele often results from a defect or avulsion of the septum from the perineal body. -Enterocele -congenital type- results from maldevelop-ment of the The vesicovaginal and rectovaginal spaces may be considerably altered. In such instances, developing the paravesical and the pararectal spaces first is very helpful. Entering the retroperitoneum - A preoperative IVU is recommended. - In most cases, the round ligament may be divided and the peritoneum lateral to the infundibulopelvic ligament incised without difficulty. - With large masses or when the anatomy is severely distorted, a paracolic or lateral psoas approach is required. The round ligament approach Placing a retractor near to the round ligament provides upward traction on it. The ligament is then picked up & transfixed. The broad lig. should be incised sharply in its lateral portion overlying the psoas Ms. The peritoneum can then be incised cephalad lateral and parallel to the ovarian vessels. This is followed by sharp & blunt dissection. The initial dissection should be bounded by the posterior leaflet of the broad ligament & the ureter medially (the ureter attaches to the broad lig. peritoneum) and the iliac vessels and the pelvic side wall laterally. The paracolic approach It is useful when the pelvic anatomy is severely distorted and the round lig not easily identified, or if the pelvis is occupied with a mass. The paracolic peritoneum is elevated and incised. The incision begins over the psoas muscle lateral to the ureter and ovarian vessels. This is followed by combined sharp and blunt dissection to mobilize medially the coecum or sigmoid colon, or to visualize the ureters. Dissection is continued down into the pelvis using the ureter as the landmark (ureteric catheter ± inserted) around which both the ovarian and the iliac vessels may be identified. Post Lt Rt Anter The incision begins over the psoas muscle lateral to the ureter and ovarian vessels. The lateral psoas approach The retroperitoneal space may also be entered over or lateral to the psoas muscle. Begin and stay medial to the iliac vessels. Opening the pelvic sidewall triangles: The uterus is deviated to one side to delineate the triangle in the opposite wall. The base of the triangle is the round lig., the lateral border is the external iliac a., the medial border is the infundibulopelvic lig, and the apex is where the infundibulopelvic ligament crosses the common iliac artery. The peritoneum in the middle of the triangle is incised and the broad lig is opened by bluntly separating the extraperitoneal areolar tissue. Even tiny vessels should be coagulated. The incision is extended to the round ligament which is not divided at this time and then to the apex of the triangle lateral to the infundibulopelvic ligament. The paravesical space is opened and the infundibulopelvic ligament is pulled medially. Thanks prof morad k hasanein